NHs Plan of Safe and Supportive Care POSC
 for Substance-exposed Infants July 17, 2019")
 Overview & Introduction to NH POSC Resources")























 • Inconsistency amongst staff")

 and OB Providers help complete POSC")








 – ideally")


 •")
 •")
 •")
 • See NH Center of Excellence website")

 • Individualize to the woman, acknowledging that")

 • Start early and update often")
 • Create")








 NOON WEBINAR Community Partners for POSC Development")

- Slides: 60
NH’s Plan of Safe and Supportive Care (POSC) for Substance-exposed Infants July 17, 2019 webinar
AGENDA NH Plan of Safe Care (POSC) Overview & Introduction to NH POSC Resources � Lucy C. Hodder JD, Director, Health Law and Policy; Professor of Law, UNH School of Law and Institute for Health Policy and Practice Q&A period with: Lucy C. Hodder JD � Joseph Ribsam Jr. JD, Director, NH Division for Children, Youth and Families � Patricia M Tilley MS Ed, Deputy Director, New Hampshire Division of Public Health Services, Department of Health and Human Services � NH hospital POSC Experience: NH POSC Hospital Survey results � NH Birth Hospital POSC Implementation Processes � Dartmouth-Hitchcock: Bonny Whalen MD & Sandi Decato MSW Wentworth Douglass: Lyndsey Wyma MSW � Brainstorming NH POSC Challenges & Strategies - Bonny Additional POSC Resources/ Upcoming Events
https: //jsi. webex. com/recordingservice/sites/jsi/recording/playback/47 e 0 a 90 cbee 1464 d 8 b 1 bff 2 bcb 378 ed 9 https: //jsi. webex. com/recordingservice/sites/js i/recording/playback/47 e 0 a 90 cbee 1464 d 8 b 1 bf f 2 bcb 378 ed 9 WHAT IS A PLAN OF SAFE CARE? AN INTRODUCTION TO BEST PRACTICES IN NEW HAMPSHIRE Presented by: Lucy C. Hodder, JD Professor of Law and Director of Health Law and Policy UNH Franklin Pierce School of Law, IHPP July 17, 2019
NH Governor’s Commission on Alcohol and Other Drugs Perinatal Substance Exposure Task Force Plans of Safe Care (POSC) 4
Overview of POSC Process Is the infant affected by prenatal drug and/or alcohol exposure? Baby Born It is best practice to begin developing a POSC prenatally. No Yes It is best practice to develop POSC for all mothers and infants Notification of Birth* & POSC Developed POSC is sent to DCYF and sent home with mother upon discharge Yes Is a mandatory report made? No POSC is required by law No POSC is sent home with mother upon discharge. *Notification is captured through two situational surveillance questions on the birth certificate. 5
Framework to Support Mothers & Infants • How can we engage mothers in a collaborative process to plan for healthy outcomes? • How can we work with existing supports and coordinate new services to help infants and families stay safe and connected? State Community Mothers & Infants • How can Plans of Safe Care support mothers and infants during pregnancy, delivery, safe transition home and in parenting? Clinical Teams 6
What is a Plan of Safe Care? A Plan of Safe Care also referred to as “Plan of Supportive Care” for mothers and infants is developed by a health care provider collaboratively with the mother and coordinates existing supports and referrals to new services to help infants and families stay safe and connected when they leave the hospital. 7
When is the POSC developed with a mother? POSC must be developed when “an infant is born identified as being affected by substance abuse or withdrawal symptoms resulting from prenatal drug exposure or fetal alcohol spectrum disorder. ” See RSA 132: 10 -e. However, best practices support developing POSCs prenatally to serve as a living document throughout the pregnancy and after birth, especially when there is a risk of prenatal exposure to substance use. 8
Federal CAPTA/CARA Requirements Notification of Birth Federal Data Reporting POSC Development Monitoring Referrals and Service Delivery Child Abuse and/or Neglect Reporting Process – not changed by CARA 9
NH’s Plan of Safe Care Statutory Process SB 549: RSA 132: 10 -e and f Infant Born… Health Provider Shall. . “When an infant is born identified as being affected by substance abuse or withdrawal symptoms resulting from prenatal drug exposure or fetal alcohol spectrum disorder…” “… the health provider shall develop a Plan of Safe Care in cooperation with the infant’s parents or guardians and NH DHHS, Division of Public Health Services, as appropriate. ” 10
What is the purpose of a POSC? RSA 132: 10 -e and f Infant and Parent(s) The POSC must account for: • Safety and well-being of • Whether the infant’s family • Address health and substance use treatment needs • Make appropriate referrals prenatal exposure is due to prescribed medication • Whether the mother is or will be actively engaged in treatment upon discharge and deliver appropriate interdisciplinary health and social services 11
What is Notification? • New Hampshire has a federal data reporting requirement, which is referred to as “notification”. • The state reports annually to the federal Children’s Bureau the aggregate number of infants born affected by prenatal drug and/or alcohol exposure for whom a POSC was created and for whom services were referred. Notification ≠ Reporting 12
Notification Questions Exposure Concern Was there documented opioid exposure at any time during the pregnancy? Was the infant monitored for signs of opioid withdrawal or neonatal abstinence syndrome (NAS)? Aim: Determine the number of infants exposed to opioids in utero. Aim: Determine the number of infants considered to be at risk for withdrawal by the medical team. q Yes q No q Unknown 13
Best Practices: POSC Process Notify • Notify public health of the birth of exposed and affected infants as requested on birth certificate. Develop • Develop POSC with all mothers or caregivers early in pregnancy. * Provide • Provide a copy of the POSC to the mother and the infant’s primary care provider upon hospital discharge. Coordinate Submit • Coordinate the mother’s referrals and access to appropriate supports and services. • Submit the POSC to DCYF when a report of child abuse or neglect is made. Include *POSC must be developed when an infant is born with and identified as being affected by substance abuse or withdrawal symptoms resulting from prenatal drug exposure or fetal alcohol spectrum disorder. 14
What is Reporting? Reporting • • • A provider may determine circumstances warrant a mandatory report to DCYF. A report must be made when a provider ‘has a reason to suspect’ an infant has been abused or neglected pursuant to RSA 169 -C: 3. If a report is made to DCYF, a copy of the POSC must accompany the report. Guidance Mandatory reporting is required under NH RSA 169 -C: 29 whenever anyone has a reason to suspect child abuse and/or neglect. The fact an infant is born with prenatal exposure to drugs and/or alcohol does not itself require a mandatory report. 15
Considerations: Abuse and Neglect NH does not have a bright line rule Has the child’s health suffered or is it likely to suffer serious impairment? Are the parents unable to discharge responsibilities to or for the child because of hospitalization or mental incapacity? What is the infant’s contact with other persons involved in the illegal use or sale of controlled substances or the abuse of alcohol? 16
Does the POSC contain confidential information? YES! The POSC is developed with the mother. She is encouraged to share the plan with others who can support her. Use best practices to avoid stigma and encourage access to supports and services. The POSC includes patient information and can be shared consistently with your privacy practices. If a report of child abuse and/or neglect is made, the POSC must be shared with DCYF. The POSC contains identifying information about the mother and infant that is private and is protected from disclosure by health privacy laws, and even substance use disorder record confidentiality laws if the developing provider is a SUD program (42 CFR Part 2) 17
Overview of POSC Process For an additional 30 minute Overview of Plans of Safe Care in New Hampshire, go to: https: //jsi. webex. com/recordingservice/sites/jsi/recording/playback/47 e 0 a 90 cbee 1464 d 8 b 1 bff 2 bcb 378 ed 9 Is the infant affected by prenatal drug and/or alcohol exposure? Baby Born It is best practice to begin developing a POSC prenatally. No Yes It is best practice to develop POSC for all mothers and infants Notification of Birth* & POSC Developed POSC is sent to DCYF and sent home with mother upon discharge Yes Is a mandatory report made? No POSC is required by law No POSC is sent home with mother upon discharge. *Notification is captured through two situational surveillance questions on the birth certificate. 18
POSC Question and Answers What is “Notification”? How is it different than a mandatory report? What happens to the POSC when a report of child abuse and/or neglect is made? What if a mother declines to participate in developing a POSC? Does the POSC contain information protected by 42 CFR Part 2 (Part 2)? Guidance Document: http: //1 viuw 040 k 2 mx 3 a 7 mwz 1 lwva 5 - wpengine. netdna-ssl. com/wp-content/uploads/2019/01/POSC_FAQ_v. 61. pdf Additional Question and Answers: http: //1 viuw 040 k 2 mx 3 a 7 mwz 1 lwva 5 -wpengine. netdna-ssl. com/wpcontent/uploads/2019/05/POSC_Questions_5. 24. 19. pdf 19
Additional Resources POSC Website • Guidance Document • Q and A • Trainings • Pregnant & Parenting Services and Supports: List & Map • Questions about POSC, email: 2019 POSC@gmail. com 20
Slides Developed and Modified by: Lucy C. Hodder, JD, Professor of Law, Director of Health Law and Policy, Institute for Health Policy and Practice at UNH School of Law David J. Laflamme, Ph. D, MPH, UNH Institute for Health Policy & Practice, NH DHHS Maternal & Child Health Epidemiologist Kali Giovanditto, Community and Family Support Specialist, Division for Children, Youth and Families Rekha Sreedhara, MPH, JSI Research and Training, NH Center for Excellence Melissa Schoemmell, MPH, JSI Research and Training, NH Center for Excellence Developed in collaboration with the Perinatal Substance Exposure Task Force of the NH Governor’s Commission on Alcohol and Other Drugs with funding provided by the New Hampshire Charitable Foundation. 21
Q&A Time! • Lucy C. Hodder JD, Director, Health Law and Policy; Professor of Law, UNH School of Law and Institute for Health Policy and Practice • Joseph Ribsam Jr. JD, Director, NH Division for Children, Youth and Families • Patricia M Tilley MS Ed, Deputy Director, New Hampshire Division of Public Health Services, Department of Health and Human Services
What is the status of NH birth hospital POSC implementation?
NH Birth Hospital POSC Survey May 2019 12/17 NH birth hospitals responded: • 9 implementing POSCs • 3 in planning phase Hospitals willing to serve as a Peer Resource: Concord, Cheshire, DHMC, Frisbie, Speare, St. Joes, Wentworth Douglass
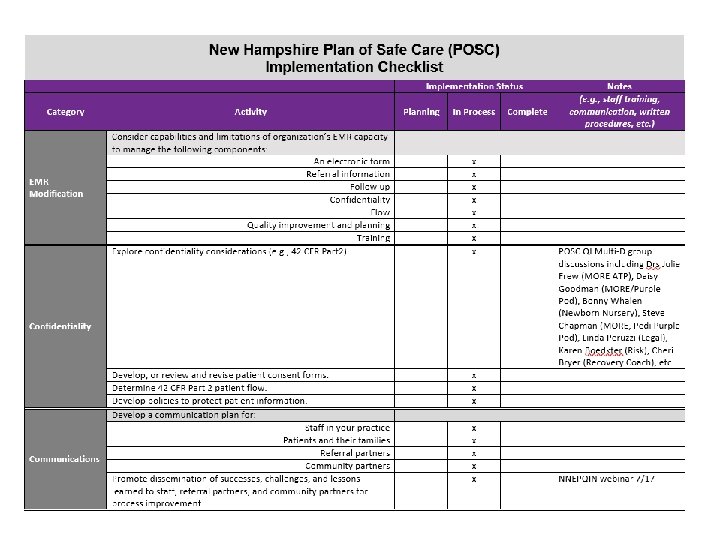
NH POSC Challenges General Challenges • • Difficulties with how to start prenatally / operationalize (4) Limited resources (3) Bandwidth for all patients rather than just SUD (2) POSC not accessible in the EMR due to transitioning to a new EMR Patient Challenges • Patient engagement/ownership (3) • No shows, drop ins, and unexpected use (2) • OB provider may never see mom again, or only for brief period of time • Many moms do not even have a PCP
NH POSC Challenges Provider Challenges • Workload and share-ability (2) • Inconsistency amongst staff members; who will be filling it out in a way that it is meaningful to the parents and the staff (2) • Difficult to cross train other social workers (2) • Lack of provider buy-in • Initiation of POSC tool with temporary staff and new staff • Pediatrician concern about revealing too much of mom's PHI
DHMC PLANS OF SAFE CARE POSC Workflow for Prenatal Providers, & Inpatient Social Workers and Infant Providers Sandy Decato MSW and Bonny Whalen MD – Birthing Pavilion/Newborn Nursery Notes from Daisy Goodman, DNP, MPH, CNM, CARN-AP – Purple Pod Prenatal Clinic
Prenatal Clinic POSC Workflow Community Health Worker (s) and OB Providers help complete POSC supports/services grid, where appropriate / needed, documenting needs present and any education provided, resources present, and any supports/services offered in pregnancy Maintained in a Care Coordination Note in mom’s Problem List
PRENATAL POSC PROCESS All prenatal patients are screened for social determinants of health, depression, substance use (SUD), and intimate partner violence. If positive for SUD, they are offered Purple Pod care (a dedicated prenatal clinic for women with SUD). Some women decline, but many accept. Those who decline are encouraged to to be seen in Purple Pod at least once per trimester for SUD-related education and services (including support of a Recovery Coach). Discussion of the Plan of Safe Care is part of that education and we strive to do this for every Purple Pod patient (shared or not). We have built two templates to help us standardize this process. These are depicted on the prior slide, the top one is a checklist for overall prenatal care for a woman with SUD which includes a reminder to introduce the Plan of Safe Care discussion early in pregnancy and then complete the POSC in the third trimester.
PRENATAL POSC PROCESS The second is the portion of the NH POSC template most relevant to the prenatal setting, specifically targeting resource needs and services to ensure that when a woman has her baby she has as many things in place already as possible. Both of these templates are designed as living documents, to be updated regularly; and also serve as handoff tools for the inpatient setting. We also offer a copy of the POSC template to the pregnant woman, along with the CDC’s Safe Sleep brochure and the NNEPQIN ESC parent education pamphlet.
“POSC For Newborns Inpatient Social Work Procedure” In OCM shared drive for information about the process of developing POSCs with families
MSW E-DH PROCESS: USE. POSCPILOT SMART PHRASE TO OPEN POSC TEMPLATE & DOCUMENT WITHIN
POSC is placed in Multi-Disciplinary Discharge Instructions and auto-populates into the After Visit Summary which is printed and reviewed with mother/family.
BP/NBN Transitions to Home for ESC Babies At Time of Discharge, Infant Provider: • Requests 1 -2 day appointments with VNA and 1 -2 day and 2 week visits with PCP (and LC if available). • Places “. NBNNASDCINSTRUCT” smartphrase in Provider Instructions (includes ESC/ NAS concerns to watch for, details of feeding plan if baby >=10% down from birthweight or if feeding difficulties present, and importance of no substance use in parenting/breastfeeding. • Signs VNA referral in the discharge order reconciliation. • Includes the “. POSCINSERT” smartlink in the newborn’s discharge summary (as found in “. NBNDCSUMM”) to pull in the: • POSC Multi Disciplinary Instructions • Discharge f/u appointments – newborn visit 1 -2 d after d/c, paired w/ LC appt if available • VNA referral information – 1 st visit 1 -2 d after d/c (day opposite PCP newborn visit) • Provider discharge instructions
INFANT’S DISCHARGE SUMMARY
Overview of POSC Process Lindsey Wyma MSW; Inpatient Social Worker
OVERVIEW OF POSC PROCESS POSC completed for all substance-exposed infants (including THC) – ideally initiated during prenatal Care Planning Session; otherwise started on birthing unit Katie White, RNC-LRN; Perinatal NAS Care Coordinator Allow parent(s)/caregiver to work on POSC on their own and then Inpatient SW assists in finishing/typing up Original POSC given to parent(s)/caregiver & copy sent to pediatrician Eventually will be placed into infant's medical chart Copy given to DCYF as requested for mandated reports
WHO ARE YOU DEVELOPING A “PLAN OF SAFE/SUPPORTIVE CARE” FOR? WHAT ARE YOUR CHALLENGES?
PEER BRAINSTORMING POSC CHALLENGES AND STRATEGIES
GENERAL CHALLENGES Challenges Strategies Difficulties with how to start prenatally / operationalize (4) • Start with just one patient (Plan Do Study Act) … explaining value of the Plan of Safe Care • Initiate for all women with NH POSC resource grid – identifying needs & filling in only what is needed • Have dedicated staff help initiate as early as possible during the prenatal period (e. g. , clinic nurse, care coordinator, social worker, community health worker, home visiting nurse, parent resource center, recovery coach, multi-D team meetings) • Keep in mom’s care coordination note, update with each visit with all providers contributing/updating, where appropriate • Meet with pregnant women as early and as often as possible, co-developing POSC at each visit • Share paper copies with OB hospital at 36 weeks so hospital has information available at time of admission
GENERAL CHALLENGES Challenges Strategies Difficulties with how to start prenatally / operationalize (4) • Educate pregnant women in varied manners / settings • Patient education handouts / videos • Community classes • Prenatal education group visits • Prenatal education intake / follow-up visits • 1: 1 prenatal visits with care coordinator or social worker • “Preparing for Baby” community baby shower • Recovery support groups
GENERAL CHALLENGES Challenges Strategies Difficulties with how to start prenatally / operationalize (4) • Provide a copy to the woman and have her co-develop with a care provider at and in any/all of the following times and manners: • Send “Congratulations on Pregnancy” cover letter & POSC template handout to home address for all newly pregnant women, requesting them to start ahead of time, and to bring to 1 st prenatal visit to finish completing with prenatal provider at that time • Provide copy in the prenatal clinic, asking her to start filling it out while waiting for her provider, then have provider review together and help further co-develop • Send home a copy with her and ask that she start filling it out at home, together with her partner and/or other caregivers, and then bring with her to next visit • Initiate and/or update together in her room before and after her baby is born, providing her with a final copy at the time of her baby’s hospital discharge
GENERAL CHALLENGES Challenges Strategies Limited resources (3) • See NH Center of Excellence website resources: https: //nhcenterforexcellence. org/governorscommission/perinatal-substance-exposure-taskforce/plans-of-safe-care-posc/ • Peer resources: Concord, Cheshire, DHMC, Frisbie, Speare, St. Joes, Wentworth Douglass Bandwidth for all patients rather than just SUD (2) • Start early and update often • Individualize, fill in only what is needed POSC not accessible in the EMR due to transitioning to a new EMR • Use paper template, scan into EMR • Share copies with OB hospital at 36 weeks so hospital has information available at time of admission
PATIENT CHALLENGES Challenges Strategies Patient • Explain value of the Plan of Safe Care with goal to be engagement/ownership developed collaboratively with the mother to reinforce existing (3) supports and to coordinate new referrals to help infants and families stay safe and connected when they leave the hospital • Make the process and message about support vs what they are doing wrong, sharing that we think Plans of Safe Care should be developed for all moms and babies not just those with substance exposure with goal of helping infants and families stay safe and connected through the pregnancy and after delivery • Provide a copy to the woman and have her co-develop prenatally and in the birth hospital in any/all manners discussed under how to start prenatally / operationalize • Review role that social worker or other staff/providers can play in helping develop POSC to help highlight mom’s and family’s strengths & supports in place, with goal to help connect them with additional supports and services for their own physical and mental health, their infant’s health and development, and for their whole family’s health, safety and security
PATIENT CHALLENGES Challenges Strategies Patient engagement/ownership (3) • Individualize to the woman, acknowledging that some women will be harder to connect and/or engage with due to poor experiences in the past. In these cases, team members will need to adjust their approach. A one size does not fit all • Consider that a woman may have some form of trauma in her background, and that she has likely faced a lot of adversity and criticism with her addiction; the more supportive you are, the better chance you have No shows, drop ins, and unexpected use (2) • Keep the form readily available, initiate any time need is identified • Have all staff trained in how to discuss & initiate, so that can be initiated just in time • Start when meet for prenatal education / hospital tour session
PATIENT CHALLENGES Challenges Strategies “Plan of Safe Care” wording sounds judgmental and stigmatizing for women with substance use disorder • Consider using “Plan of Supportive Care” wording instead to emphasize a non-judgmental approach to supporting mothers as crucial partners in their babies’ care and review that best practice recommendation is to develop a POSC for all mother-baby dyads OB provider may never see mom again, or only for brief period of time • Understand that any support / completion of POSC, and connection with woman can be helpful Many moms do not even • Help identify PCP when need identified have a PCP • Have list of Recovery Friendly PCPs readily available
PROVIDER CHALLENGES Challenges Strategies Workload and shareability (2) • Start early and update often • Have all prenatal staff trained to share in POSC development / updating • Maintain close / effective communication with social worker / birth hospital, sharing updated POSC after 36 week visit • Create a resource group for pregnant women / mothers with substance use disorder Lack of provider buy-in; • Share value of completing Plan of Safe Care with Inconsistency amongst women, helping develop supportive care in pregnancy staff members; who will and for discharge to home be filling it out in a way • Have expectation that all are responsible for that it is meaningful to the assisting in POSC development in some way parents and the staff (2)
PROVIDER CHALLENGES Challenges Strategies Difficult to cross train other social workers (2) • Create SW POSC resource / implementation guide Initiation of POSC • Include overview and instruction on POSC development tool with temporary in staff orientation staff and new staff Pediatrician / provider concern about revealing too much of mom's PHI • It is appropriate to share information relevant to baby’s medical care consistent with individual hospital’s privacy practices • Most information shared is already in baby’s discharge summary • Information that is obtained by maternal consent from her addiction treatment program records may not be included in her or her baby’s medical record without the mother consenting to or confirming that information is accurate when reviewed together with her. For more information: https: //www. samhsa. gov/about-us/who-weare/laws-regulations/confidentiality-regulations-faqs
PROVIDER CHALLENGES Challenges Strategies Community supports desire a copy of the POSC but do not receive one: “Many of the moms • Initiate and share a written or electronic copy of the POSC with the mother during the pregnancy, encouraging her to share with her existing community supports so that they can help reinforce existing supports and help refer to new ones, as needed • Connect with local community support agencies to 1) educate re: clinic/hospital POSC process, 2) develop systems to help encourage mothers to sign release of information to share POSC with their community supports, and 3) request assistance in co-developing POSCs with women in pregnancy and after discharge to home including in helping identify current strengths and goals, and helping identify and refer to any additional supports / services needed we serve are experiencing SUD. We help develop the POSC prenatally by connecting women and families to supports and services when needs are identified but I never receive a copy of the POSC during the pregnancy and/or after their discharge to home. How might Family Resource Centers (or other community agencies) receive a copy of the POSC so that they can help consistently reinforce and further develop Plans of Safe Care with families? ”
NH POSC RESOURCES https: //nhcenterforexcellence. org/governors-commission/perinatal-substance-exposure-task-force/plans-of-safe-care-posc/
NH POSC FACT / FAQ SHEETS
NH’S POSC TEMPLATE
NH’s POSC Template
OTHER NH RESOURCES AVAILABLE
Maternal Transitions in Care for the Mother. Infant Dyad Affected by Opioid Use § Caitlin E. Martin, MD, MPH § Lisa Cleveland, Ph. D, RN, PNP-BC, IBCLC, FAAN Webinar link: https: //safehealthcareforeverywoman. org/wpcontent/uploads/2019/07/Pediatric-Transitions-in-Care-for-the-Mother-Infant-Dyad. Affected-by-Opioid-Use-Disorder-1. mp 4 Pediatric Transitions in Care for the Mother. Infant Dyad Affected by Opioid Use Disorder § Eileen Costello, MD, Chief, Ambulatory Pediatrics, Boston Medical Center § Davida Schiff, MD, Medical Director, HOPE Clinic, Massachusetts General Hospital § Lori Sprecher, MS, RNC-LRN, Clinical Manager, Special Care Nursery and LDRP, Meritus Health Webinar link: https: //safehealthcareforeverywoman. org/wp-content/uploads/2019/07/Pediatric -Transitions-in-Care-for-the-Mother-Infant-Dyad-Affected-by-Opioid-Use-Disorder-1. mp 4 Sponsored by: ACOG’s Alliance for Innovation on Maternal Health, Maternal– Infant Health and Opioid Use Project in collaboration with the American Academy of Pediatrics
AUG 13 ESC WEBINAR Presented by Farrah and Bonny CME available – register at link below Objectives: Highlight perinatal quality improvement work happening through the Northern New England Quality Improvement Network (NNEPQIN) Provide an overview on Eat Sleep Console (ESC) QI work at Dartmouth and in NNEPQIN hospitals to improve care for opioidexposed newborns, including potential outcome impact Provide an update on the ESC Care Tool & hospital implementation guide https: //zoom. us/webinar/register/WN_iire 9 rem. Q 1 Ct 5 Ca 6 z_bw. AA
TH AUG 28 (4 WED) NOON WEBINAR Community Partners for POSC Development
https: //med. dartmouth-hitchcock. org/carpp. html Please call 603 -653 -1800 or email your mother/baby questions and challenges to: CARPP@hitchcock. org