NEWBORN ASSESSMENT ALICIA A STONE RN MS FNP

NEWBORN ASSESSMENT ALICIA A. STONE RN, MS, FNP ASSISTANT PROFESSOR OF NURSING MOLLOY COLLEGE

Everyone is kneaded out of the same dough but not baked in the same oven. ~Yiddish Proverb

Nursing Objectives To promote physical well-being. Nursing care Physical assessment Nutrition To promote and establish a functioning family. Support Education

Fetus to Newborn: Respiratory Changes Initiation of respirations Chemical surfactant reduces surface tension 34 -36 wks decrease in oxygen concentration Thermal sudden chilling of moist infant Mechanical compression of fetal chest during delivery normal handling

Apgar Scoring

Neurologic Adaptation: Thermoregulation The maintenance of body temperature is a major task for the NB infant (normal temperature is 97. 7 -98. 6) 1) their skin is thin and blood vessels are close to the surface 2) they have little SQ fat to serve as a barrier to heat loss 3) they have 3 x the surface to body mass as an adult 4) Preterm infants are especially susceptible to heat loss because their tone is poor and they have even less fat and thinner skin than full term babies.
 Evaporation-occurs when wet surfaces are exposed to air. 2)")
Methods of Heat Loss 1) Evaporation-occurs when wet surfaces are exposed to air. 2) Conduction- occurs when the NB comes in direct contact with objects that are cooler than their skin. 3) Convection- occurs when heat is transferred to air that surrounds the NB. 4) Radiation- occurs when there is a transfer of heat to cooler objects that are not in direct contact with the infant.

Convection Radiation Evaporation Conduction
")
Nonshivering thermogenesis The distribution of brown adipose tissue (brown fat)
 Metabolic Rate: leads to use of glucose and production")
Effects of Cold Stress 1) Metabolic Rate: leads to use of glucose and production of Surfactant. This can lead to hypoglycemia and respiratory distress. 2) Non-Shivering Thermogenesis-metabolism of Brown fat. This leads to increased production of free fatty acids, which leads to metabolic acidosis and jaundice. 3) Vasoconstriction: leads to pale, mottled skin and shut down of pulmonary vessels, which leads to fetal circulation patterns.

Bonding Kennell and Klaus En face Encourage Breastfeeding Skin to skin
 Vital signs, Color, Eyes wide open.")
Periods of Reactivity First Period (30 -60 minutes) Vital signs, Color, Eyes wide open. Encourage attachment (Bonding) Apgar Scoring, radiant warmer Medications Sleep Phase (1 – 4 hours) Second Period (4 – 12 hours) Intense sensitivity to internal and external stimuli. Void and meconium Watch mucus, apnea, emesis

Nursing Assessments Vital signs Measurements Gestational Age Medications Glucose levels Temperature stabilization. What is a successful transition? ? ?

General Survey Appearance Symmetry, any obvious deformities, size, smell, muscle tone, sex, posture Behavior Crying, lethargic, responsive, reflexes, jittery

Measurements Normal Weight 2500 -4000 gms 5 ½lbs. – 8 lbs, 13 oz. (AGA-appropriate for gestational age) Below normal (SGA- small for gestational age)- <10% Above normal (LGA-large for gestational age)- >90%

Normal Length- 18 -22” or 48 -52 cm. Head circumference- 13 -14” or 32 -36 cm. (measure right above eyebrows) Chest circumference- 12 -13” or 30 -34 cm (measure at nipple line)

Vital Signs Temperature- first is usually taken axillary, but may be taken rectally to assure anal patency (36. 5 -37. 5 C or 97. 599. 5 F) Pulse- 110 -160 bpm, unless sleeping (100) or crying (180) Respirations- 30 -60 with periodic breathing B/P- only if suspected heart problem or premature infant

Gestational Age Assessment

Physical Characteristics of Gestational Age
 Erythromycin Ointment")
Medications in the Delivery Room Vitamin K (Aquamephyton) Erythromycin Ointment

FONTANELLES Bulge – IICP Depressed – dehydration

Molding Overriding sutures. Resolve quickly

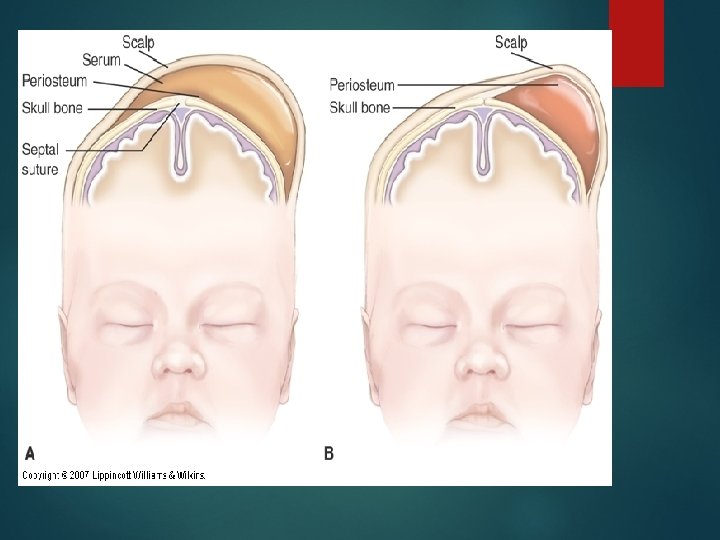
Caput Succedaneum Soft tissue edema from birth trauma. Crosses suture lines.

Cephalohematoma Bleeding between the cranial bone and the periosteum in periosteal space. Does not cross suture lines What will happen when it starts to resolve?

SKIN Reddish in color, smooth, puffy. Edema Turgor Cord Nails

Acrocyanosis Mottling Jaundice

PHYSIOLOGIC JAUNDICE Hyperbilirubinemia not associated with hemolytic disease or other pathology in the newborn. Jaundice that appears in full term newborns 24 hours after birth and peaks at 72 hours. Bilirubin may reach 6 to 10 mg/dl and resolve in 5 to 7 days.

Vernix Milia
 - Forcep marks - Mongolian spots - Birthmarks: Port")
Rashes/Marks Erythema Toxicum (Newborn Rash) - Forcep marks - Mongolian spots - Birthmarks: Port wine stain Stork bite/Nevi Strawberry mark Café au lait - Petechiae -

Erythema Toxicum Mongolian spot Forcep mark

Port wine stain Stork bite/ Nevi Strawberry hemangioma

Eyes Check color, red reflex. Subconjunctival Hemorrhage From birth trauma Chemical Conjunctivitis from a reaction to eye prophylaxis.

Ears Pinna top on horizontal line with outer canthus of eye Loud noise elicits Startle Reflex Flexible pinna with cartilage present

Nose EXPECTED FINDINGS COMMON VARIATIONS Nostrils patent bilaterally Obligate nose breathers No nasal discharge Sneezes to clear nostrils Bridge appears absent Thin white nasal mucus discharge Signs of potential distress or deviations from expected findings Malformation Nasal flaring beyond first few moments after birth

MOUTH AND THROAT Mucosa moist Palate high arched Well developed fat pads bilateral cheeks Sucking, rooting, gag, and extrusion reflex. Epstein’s pearls, thrush, supernumerary teeth, cleft palate

Cleft lip and palate

CHEST Expected findings Evident xiphoid process Equal anteroposterior and lateral diameter Bilateral synchronous chest movement Symmetrical nipples Common variations "Witch's milk" Enlarged breasts Accessory nipples Apical Pulse, check for retractions, grunting

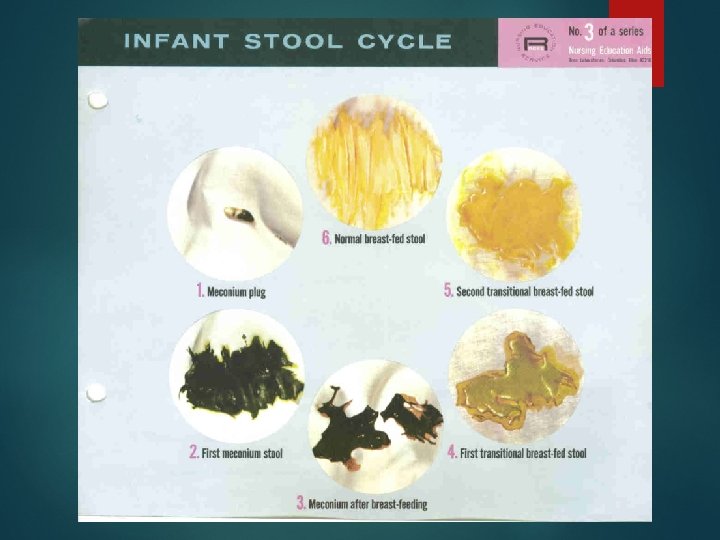
ABDOMEN Expected Findings Dome-shaped abdomen Abdominal respirations Soft to palpation Well formed umbilical cord Three vessels in cord Cord dry at base Liver palpable 2 - 3 cms below right costal margin Bilaterally equal femoral pulses Bowel sounds auscultated within two hours of birth Voiding within 24 hours of birth Meconium within 24 - 48 hours of birth

GENITALIA FEMALE Edematous labia and clitoris Labia majora are larger and surrounding labia minora Vernix between labia MALE Urinary meatus at tip of glans penis Palpable testes in scrotum Large, edematous, pendulous scrotum, with rugae Smegma beneath prepuce Stream adequate on voiding

EXTREMITIES Maintains posture of flexion Equal and bilateral movement and tone Full range of motion all joints Ten fingers and ten toes Legs appear bowed Feet appear flat Palmar and sole creases evident

POLYDACTYLY Count the fingers and toes. Open the hand look!

HIP DISLOCATION Ortolani’s manuver Unequal leg length Asymmetrical skin creases posterior thigh

CLUB FOOT Talipes Equinovarus When the foot turns inward and downward Check for normal positioning and whether it corrects easily. May be positional.

NEUROMUSCULAR SYSTEM Expected findings Maintains position of flexion When prone, turns head side to side Holds head and back in horizontal plane when held prone Ability to hold head momentarily erect Moro reflex Signs of potential distress or deviations from expected findings Hypotonia Quivering Limp extremities or straightening of extremities Clonic jerking Paralysis

BEHAVIORAL Observe how the baby quiets to soothing, cuddling, or wrapping Sleep-wake cycles. Brazelton Behavioral Assessment Scale. Watch for excessive crying, fretfulness, and inability to quiet self (Drug Withdrawal)

ADDITIONAL CARE Suctioning Positioning Wrapping Holding Circumcision Care Newborn Testing PKU, T 4 Hearing

PARENT EDUCATION Axillary temp Bathing Care of nails Diapering Feeding Health care provider visits When to call for immediate attention.
- Slides: 49