NEW ADVANCES IN DIABETIC FOOT MANAGEMENT Saeid Kalbasi

NEW ADVANCES IN DIABETIC FOOT MANAGEMENT Saeid Kalbasi MD. Endocrinologist Loghman Hospital October 2012

Technologies Hyperbaric oxygen therapy Negative Pressure wound therapy Growth factors Bioengineered skin substitutes

Hyperbaric oxygen therapy

Overview Definition, History of Hyperbaric Oxygen therapy Terminology and Indications and protocols Process of Mediating the Healing of wounds a. ) Collagen synthesis b. ) Angiogenesis Rationale for the Use of Oxygen in wounds Antibacterial actions Reperfusion Injury Topical oxygenation Complications of HBO therapy

Definition of HBO Therapy Involves the inhalation of oxygen at partial pressures meeting or exceeding 1. 4 ATA. ---(Whelan, H. T. and Kindwall, E. P. 1999).

History At its inception, lacked a scientific basis. Precursors of modern hyperbaric oxygen simply seemed like good ideas. Henshaw 1662 Compressed air therapy resurfaced in the 19 th century in the European continent: a. ) Some of the devices could be pressurized to 2 ATA (the pressure equivalent of a 33 -foot column of sea water) b. ) Capacity up to 10 occupants.
 and Corning (1891). a. ) Fabricated a mobile operating room on")
History Fontaine (1879) and Corning (1891). a. ) Fabricated a mobile operating room on wheels, b. ) Pressurized in concert with the administration of the anesthetic gas nitrous oxide. Ø Benefits of the hyperbaric surgical environment a. ) Reduction in the size of hernias b. ) Decreased cyanosis, b. ) Decreased cyanosis Ø Corning, a. ) The first physician to administer spinal anesthetic b. ) Imported compressed air therapy into the United States c. ) Pioneered electrical powering of compressors. Ø
 heart")
History Cunningham, Ø Promoted hyperbaric therapy based on epidemiological observations. Individuals A. ) heart disease B. ) circulatory problems Observations 1. ) Fared less well than similarly stricken patients dwelling near sea level. 2. ) Patitents at altitude fared better when relocated to sea level. Hypothesis: Ø PRESSURE WAS THE KEY Ø Elevation of pressure beyond that characteristic of sea level would confer even greater benefit.

History Case Report A young colleague bear death from the flu apparently exhibited a remarkable recovery in conjunction with hyperbaric therapy. Early chambers Created a large chamber measuring 88 feet in length with a 10 -foot diameter in Kansas City. Treatment Protocols Ø No discrimination for clinical indications met by compressed air therapy. Ø Further hypothesized Ø Ailments stemmed from infection with anaerobic bacteria. Ø Elevated partial pressures of oxygen would hinder anaerobic bacteria, Case report 2 Kidney patient underwent a nearly miraculous recovery while under the care of Cunningham.

History Results Techniques of Cunningham were “miracles”, The wealthy patient rewarded Cunningham by constructing the largest hyperbaric chamber ever to have existed. The giant sphere, “Steel Ball Hospital” a. ) Located in Cleveland, Ohio, b. ) Measured an impressive 6 stories in height and 64 feet in diameter. c. ) Interestingly, the enormous chamber, Ø Could sustain pressures of 3 ATA (66 fsw), Ø Was lavishly appointed with carpeting, cafeterias, and a topfloor smoking lounge Ø Cost 1, 000 USD

History Results Unable to gather data sufficient to support his broad hypothesis concerning: A. ) Anaerobic bacteria in disease : (e. g. , hypertension, uremia, diabetes and cancer). The AMA and Cleveland Medical Society in 1930 forcibly closed the hospital, condemning it to scrap for use during World War II.
 1. ) Were the first to employ elevated concentrations")
History Churchill-Davidson and colleagues (1955) 1. ) Were the first to employ elevated concentrations of oxygen, 2. ) Became known as hyperbaric oxygen therapy. 3. ) Oxygen was used in attempts to potentiate therapeutic effect of radiation in cancer patients. Boerema and associates (1956), a. ) Prolonged tolerance to a circulatory arrest related to cardiac surgery.

Concepts Physical properties of gases under pressure, Ø At pressure greater than 1 atm. Ø Oxygen is essential in a variety of enzymatic, biochemical, and physiologic interactions a. ) Promote normal cellular respiration and tissue function. b. ) Collagen deposition and synthesis c. ) Angiogenesis and epithelization also are oxygen dependent.
 Oxygen from air diffuses across the")
Rational for HBO use: The mechanism 1. ) Oxygen from air diffuses across the aveoli Ø From the high pressure in the alveoli (p. O 2 100 mm. Hg) to lower pressure pulmonary capillaries (p. O 2 40 mm. Hg). Ø The pulmonary capillaries carry the deoxyhemoglobin in the blood from the right ventricle to the lungs. Ø After oxygenation blood (carrying oxyhemoglobin) moves into the pulmonary veins for return to the left side of the heart to be pumped systemically.

Rational for HBO use Under normal conditions, > 97. 5% of 02 is carried in the bloodstream bound to hemoglobin. Ø The remaining 2. 5% is dissolved in plasma. Each gram of hemoglobin combined with 1. 34 cm 3 of oxygen. > physiologic maximum. > normal conditions, Sa 02 hb = 97%, SV 02 =70%. The oxygen content can be calculated with the following equation: Ø Ca. O 2=(Sa. O 2 x Hb x 1. 34) +. 003(Pa. O 2) > Increase Pa 02 = increased dissolved 02 in the blood

Boyle’s Law At a constant temperature, the volume and the pressure of a gas are inversely proportional. In other words……. A gas will compress proportionately to the amount of pressure exerted on it.
 1. ) Decompression sickness, 2. ) Carbon monoxide poisoning, 3) Gas embolism,")
Indications (13) 1. ) Decompression sickness, 2. ) Carbon monoxide poisoning, 3) Gas embolism, 4. ) Gas gangrene with positive culture for a clostridial species, 5. ) Acute osteomyelitis refractory to standard medical management, 6) Chronic non-healing (problem) a. ) Documented failure of an intensive wound management program (minimum of 6 weeks) b. ) Failure of surgical management or documentation from a surgeon of poor tissue oxygenation
 Refractory bacterial infections, 8. ) Acute traumatic ischemia in a salvageable")
Indications 7. ) Refractory bacterial infections, 8. ) Acute traumatic ischemia in a salvageable area, 9. ) Radiation necrosis (osteoradionecrosis and soft tissue radiation necrosis) 10. ) Acute cerebral edema 11. ) Profound anemia with exceptional blood loss: a. ) only when blood transfusion is impossible or must be delayed, 12. ) Refractory mycoses, 13. ) Acute cyanide poisoning,

Indications
, bleomycin, disulfiram, cisplatinum and mafemide acetate Untreated pneumothorax")
Absolute Contra-indications Medications like doxorubicin (adriamycin), bleomycin, disulfiram, cisplatinum and mafemide acetate Untreated pneumothorax Pregnancy Implanted pacemakers-electronic Smoking No air plane travel 24 hours after HBOT treatment. Compressive brain or brainstem lesions e. g. unilateral or bilateral subdural hematoma, intracranial hematoma. Sickle Cell and Sickle Cell Trait.

Relative Contra-indications Ø Ø Upper respiratory infections/chronic sinusitis Ø High fevers Ø Claustrophobia Seizure disorders Ø Otosclerosis Ø Congenital spherocytosis Ø Viral infections such as HIV or RSV Emphysema with CO 2 retention Acute asthma

Chambers MULTIPLACE CHAMBER MONOPLACE CHAMBER

Standard Treatment Protocol Chronic wounds Ø 2 ATA for 90 min 3 -4 x weekly Necrotizing infections Ø 2 ATA for 90 min TID CO Poisoning Ø 3 ATA for 30 min Ø ( ½ life of CO at 3 ATA pressure 23 min)

Process of mediating Wound Healing

Process of mediating Wound Healing Ø Ø Ø The many forms of wounds Contused (unbroken skin), Incised (cut tissue), Lacerated (torn skin), Open (free outward opening), Penetrating (affects underlying tissue) Perforating (penetrating wound into viscous or body cavity).

Process of mediating Wound Healing Ø Ø Problem wounds Those failing to respond to the conventional primary and adjunctive management within an expected period of time. Seen in individuals who do not have normal patterns or rates of tissue repair. a. ) Numerous operations b. ) Prolonged hospitalizations. c. ) Most common in the lower extremities.

Process of mediating Wound Healing Chief pathological features of problem wounds Ø Chronic hypoperfusion and contamination. Ø Successful management = Identify etiology and potentially complicating factors a. ) Advanced age, b. ) Nutritional deficits, c. ) Diabetes mellitus, d. ) Use of tobacco, e. ) Radiation damage, f. ) Hypoxia, g. ) Immunosuppression, h. ) Foreign bodies, i. ) Renal failure, j. ) c. Cancer

Normal processes of wound healing: Ø The injured blood vessels allows the wound space to be filled with plasma and red blood cells. Ø The injured endothelium releases Factor III (thromboplastin), which accelerates the clotting cascade. Ø Clotting factors throughout the plasma are activated, forming thrombin and fibrin. Ø The complement system activates and produces various chemoattractive complement protein fragments. Ø Platelets, activated by exposed collagen and activated thrombin, release a number of factors and cytokines. To limit bleeding, traumatized vessels will constrict in response to inputs a. ) ANS b. ) PG’s released by the platelets. Ø Ø The healthy vasculature proximal to the injury will dilate and leak plasma in response to various inflammatory mediators such a histamine, kinins, and serotonin, serotonin

Normal Process of Wound healing Inflamatory process = Hypoxic, acidodic and hyperlactate state Ø Neutrophils , fibroblasts, endothelial cells a. ) few mitochondria = rely on anaerobic glycolyis for ATP Ø Neutrophilic oxidants, will produce lactate a. ) Even if normal levels of 02 are present b. ) Induce an acidodic environment Ø The importance ADPR SYS a. ) Post translational modification of many proteins b. ) Regulates transcription of collagen and VEGR c. ) Lactate in the wound reduce NAD+ to NADH Ø

Normal processes of wound healing: Importance of Hypoxia Increases lactate within the wound environment, This allows the synthesis of collage secondary to (redox) mechanism HOWEVER………. . Ø Studies have proved that fibroblasts NEED 02 a. ) Synthesize collagen b. ) Posttranslational modifications necessary for its cross-linking. Take home message Hypoxia acts as the triggering mechanisms for the repair-related production of collagen, Restoration of oxygenation is required to ensure that the collagendependent processes of repair reach their successful conclusion

Synthesis of Collagen

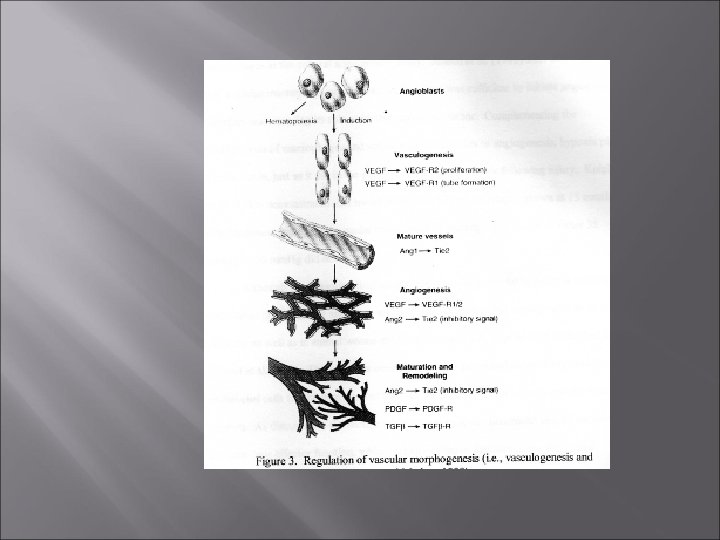
Angiogenesis Ø Vasculogenesis, > Primitive vascular network is established embryologically from endothelial cells precursors called angioblasts. Ø Angiogenesis (i. e. , neovascularization) > Proceeds as preexisting vessels send out capillary buds (sprouts) to create new vessels. > Results the chronic inflammatory process and fibrosis. > Redirection of vasculature seen during growth of tumors.
, injected autologous wound macrophages into rabbit Clark et")
Supporting Research Clark et al. (1976), injected autologous wound macrophages into rabbit Clark et al. (1976), corneas to stimulate neovascularization and Polverini et al. (1977), discovered that activated peritoneal macrophages Polverini et al. (1977), induced more vessel growth than non actviated macrophages in the corneal angiogenesis assay. Jensen et al. (1986), later demonstrated that acellular macrophage Jensen et al. (1986), conditioned media alone was sufficient to cause angiogenesis, therefore underscoring the role of the angiogenic factor. Knighton et al. (Knighton, et al. 1983), for example, demonstrated that Knighton et al. (Knighton, et al. 1983), media conditioned by macrophages grown at 15 mm. Hg p. O 2, supported angiogenesis; media conditioned by macrophages grown at 38 mm. Hg or 76 mm. Hg did not. IMPORTANCE: Despite macrophages and vascular growth factors a. ) The most notable stimulator for angiogenesis is in fact hypoxia, b. ) Similar to initiation of the synthesis of collagen in response to injury.
 BMJ 1998; 317: 1140 -1143 Clinical review ABC of oxygen")
Supporting Research 1. ) BMJ 1998; 317: 1140 -1143 Clinical review ABC of oxygen Hyperbaric oxygen therapy 2. ) Pediatr Emerg Care. Maintaining a high index of suspicion for carbon monoxide poisoning is life saving. 2008 Mar; 24(3): 198. 3. ) AANA J. Oxygen: the two-faced elixir of life. 2008 Feb; 76(1): 61 -8. 4. ). Singapore Med J. Hyperbaric oxygen therapy in the management of diabetic lower limb wounds 2008 Feb; 49(2): 105 -9. 5. ) Undersea Hyperb Med. Hyperbaric oxygen pre-breathe modifies the outcome of decompression sickness. 2006 Nov-Dec; 33(6): 407 -17.

Collagen synthesis and Angiogenesis The common link Angiogenesis and collagen synthesis and deposition share common triggers, Zabel et al. (1996). Cultured macrophages in 0 or 15 m. M lactate and then measured NAD+ and poly (ADP-ribose ) synthesis. The cells incubated with lactate demonstrated a 40% lower NAD+ level and therefore a 40% reduction in poly adenosine diphosphoribose synthetase. Constant et al. (1996) Measured vascular endothelial growth factor in media grown in normoxia, hypoxia, 15 m. M of lactate, or hypoxia and elevated lactate in combination.
 Hypoxia and lactate alone")
Collagen synthesis and Angiogenesis The common link OVERALL: 1. ) Hypoxia and lactate alone stimulate an increase in VEGF 2. ) Synthesis of collagen and the initiation of angiogenesis proceed in relation to metabolic demand, with hypoxia acting as the trigger. 3. ) Maturation of collagen and the finalization of angiogenesis require normal levels of oxygen.

Rational for HBO use I. E Ø Placing an oxygen-breathing individual in a hyperbaric chamber: a. ) Raises arterial oxygen tensions 10 - 13 times b. ) The surplus oxygen carried by the arterial blood under hyperbaric conditions will become available to wounded tissue c. ) Promoting both the maturation/deposition of collagen and angiogenesis and thus the closure of the wound. *****Lactate (associated with hypoxia) is the greatest trigger for stimulating fibroblasts and macrophages to initiate the manufacture of collagen and induce angiogenesis

Antibacterial actions of HBO Oxygen-independent Oxygen-dependent
 Ø Seen in all")
Oxygen Independent Ø More important line of defense against infection) Ø Seen in all wounds and contributes to tissue debris and edema. Neutrophils and macrophages enter the wound environment, a. ) Neutrophils = primary defense b. ) Natural (or nonspecific) immunity, > Neutrophils and macrophages + complement system Ø > Rapidly and independently of previous exposure to specific microorganisms. > The invading bacteria are opsinized by immunoglobins, > Complement proteins bind to receptors found on membranes of neutrophils, culminating in pathogenic recognition by neutrophils and phagocytosis.
")
Oxygen Dependant The respiratory burst first involves the reduction of molecular oxygen (O 2) to the microcidal superoxide anion (O 2 -) via the NADPH oxidase system, Superoxide dismutase catalyzes the interaction of the two superoxide anions to reform oxygen and hydrogen peroxide (H 2 O 2), another antibactericidal oxidant. Myeloperoxidase, released by the azurophilic granules of neutrophils, ). These halide oxygenation products are the potent oxidants that attack the membrane proteins of bacteria, (Hunt, T. 1988). The production of oxygen radicals and killing of pathogens via oxidation proceeds in relation to the availability of oxygen in the wound environment, (Park, M. , 1999).
")
What About Problem Wounds? Oxygen is often ill-equipped to reach the wound a. ) Impaired vascular delivery. b. ) Further limiting the transport of oxygen to problem wounds may be the necessarily limited oxygen-carrying capacity of the blood. Normal circumstances, a. ) The bulk of oxygen is delivered to tissue via hemoglobin with plasma carrying a significantly smaller load of oxygen (in solution). b. ) The concentration gradient may be too small to permit immunologically sufficient quantities of oxygen to diffuse from capillaries to the wound.
 Situation changes favorably b. )")
What About Problem Wounds? Under hyperbaric conditions, a. ) Situation changes favorably b. ) The breathing of 100% oxygen allows plasma to transport a greatly elevated load of dissolved oxygen c. ) Increases the total load of oxygen transported by the blood

What About Problem wounds? Increase the load of oxygen carried by the blood, Ø Concentration gradient of oxygen between the blood and the hypoxic problem wound increases, Ø Promotes diffusion of the gas into its otherwise oxygen-poor target. Ø Disruption of metabolism and proliferation of anaerobic bacteria. Ø If cells of the immune system are able to access the wound, A. ) Oxygen-dependent attacks of the immune system on both anaerobic and aerobic bacteria may increase, B. ) Thereby rendering the wound environment more amenable to healing.

Reperfusion Injury Ischemia, Ø Results from the functional constriction or actual obstruction of the blood vessel). Ø High-energy trauma Ø Compartment syndrome, Ø Amputated body parts Ø peripheral vascular disease RESULT = Some degree of microcirculatory failure and hence necrosis When reperfusion follows necrosis, a. ) There is further injury to the microvasculature, b. ) Leads to further cellular death, c. ) Large partially necrotized muscular areas being particularly vulnerable to the pathological process
 Highly unstable molecules")
The cytotoxic effects of reperfusion Ø oxygen-derived free radicals, A. ) Highly unstable molecules possessing an unpaired electron in the outer shell. B. ) Hazardous to the intracellular environment, Sources: A) Xanthine oxidase (XO), which is located in the microvascular endothelial cells and B) Neutrophils which destroy damaged tissue and invading bacteria
 Ischemia= accumulation hypoxanthine 2. ) membrane-spanning pumps fail, = increase in intracellular")
1. ) Ischemia= accumulation hypoxanthine 2. ) membrane-spanning pumps fail, = increase in intracellular levels of calcium. 3. ) Activates proteases, allowing the conversion of xanthine dehydrogenase to XO. 4. ) When reperfusion occurs, the enzyme XO converts hypoxanthine to xanthine and the superoxide radical. 5. ) hydroxy radical will emerge. . ( Aids neutrophils in the production of the hydroxy radical)

Reperfusion and HBO During reperfusion, Ø Increase in neutrophil adherence to the vascular endothelium, Ø Reflects increasing numbers of neutrophils marginating and extravasating into the surrounding tissues. Results: a. ) Local vessels will eventually become ill defined. neutrophils Releases free radicals= endothelial damage induce microcirculatory problems through adherence.
")
Reperfusion Injury Speculations One might predict that increased availability of oxygen would: a. ) Promote free radical-mediated reperfusion injury. b. ) The increased oxygen-carrying capacity of plasma under hyperbaric conditions, Ø Expect severe reperfusion in. The production of free radicals would simply escalate in concert with increased availability of oxygen. Ø The reverse is actually the case. Ø

Reperfusion and HBO The increase in microvascular flow helps increase tissue survival and therefore decreases necrosis. Decrease neutrophil adherence in the venules, a. )Decreases, problems associated with neutrophilic adhesions, > increase free radicals which= tissue damage The benefits of HBO on the ischemic tissue Ø Systemic Ø Inhalation of oxygen at a higher atmospheric pressure Ø Greater concentration of oxygen to circulate throughout the entire body A. ) Suppress of systemic neutrophils. B. ) Increase in superoxide dismutase, which is a free radical scavenger. Zamboni ( 1992),
 augmented levels")
Reperfusion and HBO Currently available evidence indicates: That systemically (rather than locally) augmented levels of oxygen mitigate the destructive consequences of free radicals in ischemic tissue undergoing reperfusion.

Quick Recap Increases in oxygen tension in a chronic wound in may permit and promote a cascade of events culminating in the full healing of otherwise nonhealing tissue. Means by which oxygen tensions are increased in such a fashion involves the inspiration of 100% oxygen under substantially elevated ambient pressures. Henrys Law, allows oxygen to diffuse readily from capillaries to otherwise inaccessible insufficiently vascularized tissue, thereby initiating oxygendependent cascades related to healing.

Overall

OVERALL

Overall

Topical Oxygenation “Men are nothing without Gods” Homer’s Odyessy

Topical Oxygenation

Topical Hyperbaric Oxygenation The rational for the topical approach is simple: Ø Some investigators believe that topical oxygen dissolves in sufficient quantity a. ) Exert bactericidal and angiogenic effects, Marketed aggressively by companies such as Ø Ø GWR Medical, Hyperbaric solutions Inc. , Sandia-Numotech partnership, which was established in 1998 to create home-use topical oxygen applicators.

The Device The devices employed in the topical application of oxygen typically consist of a compartment to encase the affected portion of the body. When connected to a regulated flow of oxygen from commercially available tanks, the compartment is intended to provide the wound with a therapeutic oxygen-rich external environment, The compartments (commonly called canopies) that enclose the wound may be box-like or function as disposable plastic bags
 Diabetes, b.")
Putative Indications Acute or chronic wounds such as skin ulceration a. ) Diabetes, b. ) venous stasis, c. ) Post surgical infection, d. ) Decubitus ulcers (pressure ulcers), e. ) Skin grafts, f. ) Frost bites, g. ) Amputations, h. ) Grangrenous lesions, i. ) Burns Contraindications: 1. ) Inadquate perfusion to support healing, 2. ) Wounds completely covered with eschar, 3. ) Wounds with fistulae or deep sinus tracts where the end cannot be probed, 4. ) Wounds covered with petroleum based dressing, 5. ) non-compliant patients.
, Nutritional status, Wound")
Screening Medical history, Allergies, Current medications, Psychological status (to predict compliance), Nutritional status, Wound description. ***NO ABI’s, NO AGRAM, NO MRA

Topical Oxygenation Protocol Debridement of the wound with removal of thick eschar. Culturing of the wound to detect pseudomonas (pseudomonas grows in an oxygen-enriched environment). If pseudomonas is detected, 1% acetic acid is applied with a gauze dressing, which remains in place during exposure to topical oxygen. All creams, ointments, and lotions must be removed as well as all dressings (except when wounds are positive for pseudomonas) before oxygen is applied topically. 8. Treatment will cease if improvement does not occur within 28 d
 or during a single")
Topical Oxygenation Applied for either 90 minutes (twice per day) or during a single session lasting 180 minutes. The lesion should be covered with a moist environmental dressing following each treatment. Before and after each treatment, the topical oxygen canopy must be cleaned with antiseptic. A culture of the appliance must be taken periodically to make prevent contamination of wounds by the apparatus. This protocol will not be followed and treatment will not be administered in the patient has acute thrombophlebitis or if there is minimal blood supply to the lesion.

Failures of Topical oxygenation Inability to complete collagen synthesis and angiogenesis Inability to produce a bactericidal effect Inability to prevent reperfusion injury
 Henry’s Law is relevant to the reversal of hypoxia")
Hypoxia (Collagen Formation and Angiogenesis) Henry’s Law is relevant to the reversal of hypoxia associated with the administration of hyperbaric oxygen. Delivery with HBO increase arterial oxygen tensions by 6 volumes percent, Solubility of 02 plasma increases greatly as a function of pressure. Importance = 1. ) Systemic elevations of oxygen tensions depend on the combination of substantially elevated pressure (e. g. , 2. 4 ATA) and pulmonary delivery of the gas. 2. ) A patient is undergoing topical oxygenation of a wound continues to breathe air at ambient pressure. Henry’s Law dictates that, A. ) Even if adequate blood flow and hematocrit are maintained, plasma at the level of the wound will not suspend significantly more oxygen. Ø

Topical oxygen, collagen synthesis and Angiogenesis NO elevated load of oxygen in plasma, Ø One can readily predict the failure of a. ) Oxygen-dependent maturation of collagen b. ) Angiogensis Henry’s Law predicts a. ) Topical oxygenation does not elevate the load of dissolved oxygen available to problematically wounded ischemic tissue, Problem wounds will remain as problems, even in the face of aggressive topical oxygen therapy
")
Putative Antibacterial Effects of Topical Oxygen Hyperbaric oxygen may exert bactericidal effects A. ) Anaerobic species as demonstrated Hill et al, (1972) (hyperbaric oxygenation and Clostridium species of bacteria). B. ) Enhance the ability of the immune system to kill even aerobic bacteria, (Ollodart, 1966). Topical Oxygenation a. ) Look at the HBO literature b. ) Oxygen delivered systemically at partial pressures lower than 1. 4 ATA does not fulfill the criteria of bacteriostatic agents (i. e. , agents that suppress the growth and proliferation of bacteria; (Park, M. , 1999).
 reported 1. ) Local")
Putative Antibacterial Effects of Topical Oxygen Park et al. (1999) reported 1. ) Local environmental conditions permits the proliferation of Pseudomonas aeruginosa. 2. ) Topical oxygen does not augment the capacity of the immune system Topical Oxygenation enthusiasts 1. ) Apparently aware (but perhaps unconcerned) by the notable contradiction, 2. ) Recommend , application of acetic acid when problems wounds are Pseudomonas-positive, Acetic Acid: 1. ) Adjunctive topical acetic acid may act as an irritant
 Bactericidal effects of")
Putative Antibacterial Effects of Topical Oxygen Mechanism of HBO 1. ) Bactericidal effects of HBO YOU NEED free radicals by YOU NEED cells of the immune system. 2. ) THEREFORE, topical oxygen therapy would need to THEREFORE augment free radicals. 3. ) BUT, therapeutic free radical production is systemically BUT, rather than locally medicated. Conclude: Basic premise upon which topical oxygen therapy is built is false.

Reperfusion Injury and Topical Oxygenation Hyperbaric oxygen exerts its beneficial effects through systemic rather than local actions. 1. ) Zamboni et. al, (Zamboni, 1999). rendered the hindlimb of rabbits ischemic for 8 hours, after which the flow of blood was restored. 2. ) Functional tests of the reperfused muscle revealed beneficial effects of hyperbaric oxygen, 3. ) Suggests that systemic factors contributed positively to the recovery of function following reperfusion. 4. ) Conducted in Humans
 What is the mechanism? ?")
Reperfusion Injury and topical oxygenation Topical oxygen 1. ) What is the mechanism? ? diminishing reperfusion injury. 2. ) Another assumption = a. ) Pure oxygen on a wound pure oxygen at marginally elevated pressures would deliver oxygen to the body at a rate similar to the lungs receiving a load of pure oxygen at pressures commonly in excess of 2 ATA.
 Unable to")
Reperfusion injury and Topical Oxygenation Topical oxygen is non systemic 1. ) Unable to have the beneficial suppression on neutrophils which play a significant role in reperfusion injury ( Zamboni et al) 2. ) May play a detrimental role in conditions in which ischemia is present
 Heng MCY: Topical Hyperbaric Therapy for Problem Skin")
Evidence Basis of Evidence 1. ) Heng MCY: Topical Hyperbaric Therapy for Problem Skin Wounds. J Dermatol Surg. Oct 1975: 1: 3: 55 -58 2. ) Heng MCY, Kloss SG: Endothelial Cell Toxicity in Leg Ulcers Treated with Topical Hyperbaric Oxygen. AM J Dermatopathol 1986; 8: 403 -410 3. ) Leslie CA, Sapico FL, Ginunas VJ, Adkins RH: Randomized Controlled Trial of Topical Hyperbaric Oxygen for Treatment of Diabetic Foot Ulcers. Diabetes Care Feb 1988 11: 2: 111 -115. Investigators reported tendencies for healing to decelerate in the presence of topical

Complications Of HBO vs Topical Oxygenation
 effects in")
Free radicals and Oxygen Toxicity Potential for oxygen to exert (potentially damaging) effects in healthy tissue located far from the wound. Increase availability of cytotoxic free radicals. Therapeutically beneficial effects of hyperbaric oxygen are achieved through the production of free radicals (e. g. , immune system-guided antibacterial effects). Toxic effects of hyperbaric oxygen well documented (Kindwall, E. , 1999). A. ) central nervous system, B. ) lungs, C. ) eyes,
 Dependent on the partial pressure of oxygen")
Free radicals and the CNS 1. ) Dependent on the partial pressure of oxygen (Whelan et. al, 1999). 2. ) central oxygen toxicity is a clinical concern at partial pressures of oxygen greater than 2. 0 ATA. Manifestations 1. ) Behavioral 2. ) Dramatic seizures on EEG. a. ) overt signs (e. g. , autonomic, affective, cognitive, or motor) b. ) Signs may be subtle or even absent, c. ) Progression between initial signs of central oxygen toxicity and seizures may be rapid.
 Partial pressures as low as 0.")
Free Radicals and The Lungs When? 1. ) Partial pressures as low as 0. 5 ATA Symptoms a. ) Substernal burning, b. ) Chest tightness, c. ) Cough, and dyspnea, d. ) Likely reversible with the cessation of hyperbaric oxygen therapy. e. ) IF not stopped = adult respiratory distress syndrome. (Kobzik, 1999). Cases of irreversible pulmonary dysfunction have NOT followed single-treatment hyperbaric oxygen protocols such as those deployed by the United States Navy.
 Secondary to lenticular")
Free Radicals and Ocular complications. Diabetic and Elderly patients. 1. ) Secondary to lenticular changes, 2. ) Progressive myopia: a. ) Partial pressures of oxygen between 2. 0 and 2. 4 ATA b. ) Recurrent treatments lasting at least 90 minutes. c. ) 20 - 40% will experience visual changes. The condition is reversible, typically resolving during six treatment-free weeks.

Cardiac Arrest This condition is a rarity in the chamber, Most arrythmias usually improve within HBO Incidence < 0. 2% ( Kindwall) Case Report 1. ) Individual suffered 30 cardiac arrests during the 48 hours he was treated during a research study. 2. ) 28 of his 30 cardiac arrests occurred at the surface The protocol Ø Multiplace > CPR can be immediatley initiated. Ø Monoplace >The patient must be removed from the chamber in order to initiate cardiopulmonary resuscitation.

Pneumothorax > This condition is a life threatening event > If patien is decompressed it will increase as # ATA’s increase. Signs of a pneumothorax Ø SOB Ø Chest pain, Ø Tracheal deviation to the side of the collapsed lung Ø Absence of breath sounds on the affected side. Pathognomonic Test Ø If the patients respiratory distress worsens on decompression and improves immediately on recompression one can diagnose a pneumothorax. Treatment: Ø The patient shoould be held at pressure until a management team can be assembled, ( surgeon, anesthesiologist etc). Ø The patient is then brought quickly to the surface Ø A needle is place into the affected side to relieve pressure.
 Patients may be fitted with clear plastic hoods. 2. ) Audio/visual")
Claustrophobia 1. ) Patients may be fitted with clear plastic hoods. 2. ) Audio/visual entertainment systems may be incorporated to add comforting distractions. 3. ) Often fabricated from clear materials 4. ) Afford visual contact between the patient and the external Environment
 HBO therapy follows Physiological Principles and the Laws of physics 2.")
Conclusions 1. ) HBO therapy follows Physiological Principles and the Laws of physics 2. ) HBO is Currently indicated for 13 diseases and supported by the literature 3. ) Various “Fringe Therapy” based off of HBO 4. ) Evidence includes testimonial and case reports 5. ) THBO is a misnomer, that does not follow basic tenets of certain physiological principles and laws 6. ) THBO, is a therapy that physicians should be aware of and not utilize

References 1. Chambon P, Weill J, Dory J, Stosser M, and Mandel P. “The formation of a novel adenylic compound by enzymatic extracts of liver nuclei”. Biochemical and Biophysical Research communications 1966; vol 25: 638, from, Gimbel M, and Hunt T. “Wound Healing and Hyperbaric Oxygenation”. In: Whelan, H. T. , Kindwall, E. P. , Hyperbaric Medcine Practice, 1999, pg. 175. 2. Chambon P, Weill J, and Mandel P. “Nicotinamide mononucleotide activation of a new Dna dependant polyadenylic acid synthesizing nuclear enzyme”. Biochemical and biophysical research Communication 1963; 11: 38 -43, from, Gimbel M, and Hunt T. “Wound Healing and Hyperbaric Oxygenation”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 175. 3. lark RA, Stone RD, Leung DY, Silver I, Honhn Dc, and Hunt Tk. “Role of macrophages in wound healing”. Surgical forum 1976; 269: 804 -6, from, Gimbel M, and Hunt T. “Wound Healing and Hyperbaric Oxygenation”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 181 4. Cotran RS, and Mitchell RN. (1999). “Hemodynamic disorders, Thrombosis and Shock”. In: Cotran, RS, Kumar V, and Collins T. (eds), Robbins Pathologic basis of Disease, W. B. Saunders Company. Chapter 5, pg. 119 -120. 5. Constant J, Suh DY, Hussain Mz, and Hunt TK. “Wound Healing angiogenesis: The metabolic basis of repair”. In: M. E. Marargoudokis and North Atlantic Treaty Organization. Scientific affairs Division, eds. Molecular, cellular and clinical aspects of angiogenesis. New York: Plenum Press, 1966: ix, 298, from, Gimbel M, and Hunt T. “Wound Healing and Hyperbaric Oxygenation”. In: Whelan HT, and Kindwall EP, Hyperbaric Medcine Practice, 1999, pg. 183. 6. Chang and Mathers SJ. “Comparison of the effect of bacterial inoculations in musculocutaneous and random-pattern flaps”. Plast Reconstr Surg 1982; 70: 1 -10, from, Gimbel M, and Hunt T. “Wound Healing and Hyperbaric Oxygenation”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 187 -188. 7. Dorlands, pocket medical dictionary, 25 th edition pg. 428. Feng Lj, Berger BE, Lysz TW, and Shaw WW. “Vasoactive prostoglandins in the impending no-reflow state: Evidence for a primary disturbance in microvascular tone”. Plast Reconstruction Surgery. 1988; 81: 755, from, Zamboni W. “The Microcirculation and Ischemia-reperfusion: Basic Mechanisms of Hyperbaric Oxygen”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 171, 172, 186. 9. Feng J, Ghani Q, Ledger G, Barkhordar R, Hunt T, and Hussain M. “Modulation of vascular endothelial growth factor angiogenic activity by ADP-riboxylation”. In: M. E. Maragoudakis and NATO, scientific affairs division. , eds. Molecular, cellular and clinical spects of angiogensis. Vol 298. New York: Plenum Press, 1998: ix, 298. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 183. 10. Ghani Q, Hussain MZ, Zhang J, And Hunt TK. “Control of procollagen gene transcription and prolyl hydroxylase activity by poly(ADP-ribose)”. In: G. G. Poirier and P. Moreau, eds. ADP-ribosylation reactions. New York: Springer. Verlag, 1992: XXXVI, 410, from, Gimbel M, and Hunt T. “Wound Healing and Hyperbaric Oxygenation”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 187. 11. Gottrop F, Firmin R, Hunt Tk, and Mathes SJ. “The dynamic properties of tissue oxygen in healing flaps”. Surgery 1984; 95: 527 -36, from, Gimbel M, and Hunt T. “Wound Healing and Hyperbaric Oxygenation”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 187 -188. 12. Gimbel M, and Hunt T. “Wound Healing and Hyperbaric Oxygenation”. In: Whelan H, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 174, 178, 183. 13. Heng MCY, and Kloss SG. “Endothelial cell toxicity in Leg Ulcers Treated with Topical Hyperbaric Oxygen”. Am. J. Dermatopath 8(5): 403 -410, 1986. 14. Hill GB, and Osterhout S. “Experimental effects of hyperbaric oxygen on selested Clostridial species”. In vitro studies. J Infect Dis. 1972; 125: 17 -25, from, Park M. “ Effects of Hyperbaric Oxygen in Infectious Diseases: Basic mechanisms. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 208. 15. Hunt TK, Linsey M, Grislis H, Sonne M, and Jawetz E. “The effect of differing ambient oxygen tensions on wound infection”. Annals of surgery 1975; 181: 35 -9, from, Hunt T, and Gimbel M. “Wound healing and Hyperbaric oxygenation”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 172. 16. Hohn DC, Mackay RD, Halliday B, and Hunt TK. “Effect of O 2 tension microbial functions of leukocytes in wounds and in vitro”. Surgical forum 1976; 27: 18 -20, from, Hunt T, and Gimbel M. “Wound healing and Hyperbaric oxygenation”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 172. 17. Hunt TK, and Van winkle E jr. “ Normal repair”, in Hunt, Tk Dunphy. JE (eds): Fundamentals of wound management, NY. Appleton-Century-Crofts, 1979, 85, from, Gimbel M, and Hunt T. “Wound Healing and Hyperbaric Oxygenation”. In: Whelan HT, and Kindwall EP, Hyperbaric Medcine Practice, 1999, pg. 187. 18. Hunt TK. “The physiology of wound healing”. Ann Emerg Med 1988; 17: 1265 -73, from, Hunt T, and Gimbel M. “Wound healing and Hyperbaric oxygenation”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 171. 19. Hunt TK, and Minnesota Minning Manufacturing Co. “Wound healing and wound infection: theory and surgical practice”. New york: appleton Century-Crofts, 1980: xii, pg 303, from, Hunt T, and Gimbel M. “Wound healing and Hyperbaric oxygenation”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 172. 20. Hunt TK, and Pai MP. “The effect of varying ambient oxygen tensions on wound metabolism and collagen synthesis”. Surgery, Gynecology and Obstetrics 1972; 135: 561 -7, from, Gimbel M, and Hunt T. “Wound Healing and Hyperbaric Oxygenation”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 178. 21. Hunt TK, Twomey P, and Zederfeldt B. “Respiratory gas tensions in healing wounds”. American Journal of Surgery 1967; 114: 302 -7, from, Gimbel, M. and Hunt, T. , “Wound Healing and Hyperbaric Oxygenation”. In: Whelan, H. T. , Kindwall, E. P. , Hyperbaric Medcine Practice, 1999, pg. 179. 22. )Abstract). 1992; 19, from, Zamboni WA. “The microcirculation and ischemia-reperfusion: Basic mechanisms of hyperbaric oxygen”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 788.

30. Korn HN, Wheeler ES, and Miller TA. “Effect of hyperbaric oxygen on second degree burn wound healing”. Arch Surg. 1977; 122: 732 -737. Zamboni, “The microcirculation and ischemiareperfusion: Basic mechanisms of hyperbaric oxygen”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999. Pg. 779 -791. 31. Krasener D, and Sibbald GR. “Wound Management: Best Chronic Wound Care Practices For The Hyperbaric Practioner”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 418 -428. 32. Nemet K, Fekete G, Schuler D, Kiss E, Meszner Z, Kirvan G, Kardos G, Galanti I, Poder G, Kalamar A, Boer M, and Roos D. “Chronic granulomatoous disease: dysfunction of the phagocyte NADPH-Oxydase enzyme”. Orvosi Hetilap 1997; 138: 397 -401, from, Hunt T, and Gimbel M. “Wound healing and Hyperbaric oxygenation”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 172. 33. Leslie CA, Sapico FL, Ginuas VJ, and Adkins RH. “Randomized Control trial of topical Hyperbaric Oxygen for Treatment of Diabetic Foot Ulcers”. Diabetes care 11: 111 -115, 1988. 34. Neubauer RA, and Morton W. Dpm, Hyperbaric Oxygen Therapy. Penguin Putnam Inc. , New York, NY, 1998. Pg. 10 -11. 35. Oldart RM. “Effects of hyperbaric oxygenation and antibiotics on aerobic microorganims”. In: brown Jr IW, Cox BG, Eds. Proceedings of the Third International Conference on Hyperbaric Medicine. Washington, DC: n. Natl Acad Sci, 1966; 565 -671, from, Park M. “Effects of Hyperbaric Oxygen in Infectious Diseases: Basic mechanisms”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 208. 36. Park M. “ffects of Hyperbaric Oxygen in Infectious Diseases: Basic mechanisms”. In: Whelan, H. T. , Kindwall, E. P. , Hyperbaric Medcine Practice, 1999, pg. 206. 37. Park MK, Muvich KH, Myers RAM, and Marzella L. “Hyperoxia prolongs the aminoglycoside induced post antibiotic effect in Pseudomonas aeruginosa”, from, Park, M. “ Effects of Hyperbaric Oxygen in Infectious Diseases: Basic mechanisms”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 209. 38. Park M. “ Effects of Hyperbaric Oxygen in Infectious Diseases: Basic mechanisms”. In: Whelan HT and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 209. 39. Park M. “ Effects of Hyperbaric Oxygen in Infectious Diseases: Basic mechanisms”. In: Whelan HT, Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 218 40. Polverini PJ, Cotran PS, Gimbrone MA, Jr. and Unanue ER. “Activated macrophages induce vascular proliferation”. Nature 1977; 269: 804 -6 , from, Gimbel M, and Hunt T. “Wound Healing and Hyperbaric Oxygenation”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 181 41. Owen M, and Steward M. (2000). “Antigen Recognition”. In: Riott, Brostoff and Male. (eds), Immunology 5 th Edition , Mosby International, chapter 9, pg. 115. 42. ) Ritzenthaler JD, goldstein RH, Fine A, and Smith BD. “Regulation of the alpha 1(I) collagen promoter via a transfoming growth factor-beta activation element”. Journal of Biological chemistry 1993; 268: 13625 -31, 43. ) Skover GR. “Celllular and biochemical dynamics of wound repair: wound environment in collagen regeneration”. Clinics in Podiatric Medicine and Surgery, 1991; 8: 723 -56, from, Gimbel M, and Hunt T. “Wound Healing and Hyperbaric Oxygenation”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 178. 44. Whelan H, and Clark J. “Oxygen Toxicity”. In: Whelan HT, and Kindwall EP. Hyperbaric Medcine Practice, 1999, pg. 70 -76. 45. Venkatachalam MA. (1999). “Cellular Pathology: Cell Injury and cell Death”. In: Cotran RS, Kumar V, and Collins T. (eds), Robbins Pathologic basis of Disease, W. B. Saunders Company, chapter 1, pg. 11 -12. 46. Young. B, and Heath JW. Functional Histology a text and colour atlas. Church Livingstone, 2000, pg. 50. 47. Zamboni WA. “The microcirculation and ischemia-reperfusion: Basic mechanisms of hyperbaric oxygen”. In: Whelan HT, and Kindwall EP. Hyperbaric. Medcine Practice, 1999, pg. 779 -791 48. Zamboni WA, Roth AC, Bergman BA, Russell RC, Stephenson LL, and Suchy H. “Experimental evaluation of oxygen in the treatment of ischemic muscle. ” Undersea Biomedical

Whereas the systematic review of the International Working Group that considered HBO accepted that there was some evidence to support its use, it is clear that more data are required from larger controlled trials not only to confirm efficacy but also to clarify which wounds might best benefit from this expensive treatment Hinchliffe RJ , Valk GD , Apelqvist J , Armstrong DG , Bakker K , Game FL , et al. A systematic review of the effectiveness of interventions to enhance the healing of chronic ulcers of the foot in diabetes. Diabet Metab Res Rev 2008 ; 24 ( Suppl 1): 119 – 144.

Negative Pressure wound therapy

Bollero D, et al. THE ROLE OF NEGATIVE PRESSURE WOUND THERAPY IN THE SPECTRUM OF WOUND HEALING. Ostomy Wound Management. 2010; 56(5 Suppl): 1– 18.

Bollero D, et al. THE ROLE OF NEGATIVE PRESSURE WOUND THERAPY IN THE SPECTRUM OF WOUND HEALING. Ostomy Wound Management. 2010; 56(5 Suppl): 1– 18.

Bollero D, et al. THE ROLE OF NEGATIVE PRESSURE WOUND THERAPY IN THE SPECTRUM OF WOUND HEALING. Ostomy Wound Management. 2010; 56(5 Suppl): 1– 18.

Bollero D, et al. THE ROLE OF NEGATIVE PRESSURE WOUND THERAPY IN THE SPECTRUM OF WOUND HEALING. Ostomy Wound Management. 2010; 56(5 Suppl): 1– 18.

Bollero D, et al. THE ROLE OF NEGATIVE PRESSURE WOUND THERAPY IN THE SPECTRUM OF WOUND HEALING. Ostomy Wound Management. 2010; 56(5 Suppl): 1– 18.

Bollero D, et al. THE ROLE OF NEGATIVE PRESSURE WOUND THERAPY IN THE SPECTRUM OF WOUND HEALING. Ostomy Wound Management. 2010; 56(5 Suppl): 1– 18.

Bollero D, et al. THE ROLE OF NEGATIVE PRESSURE WOUND THERAPY IN THE SPECTRUM OF WOUND HEALING. Ostomy Wound Management. 2010; 56(5 Suppl): 1– 18.

Growth factors A number of growth factors and other agents designed to modify abnormalities of the biochemistry of the wound bed or surrounding tissues have been described, but there is still no consensus as their place in day - to - day clinical practice. One example is platelet - derived growth factor (PDGF) which is available for clinical use in a number of countries. Jeffcoate WJ , Lipsky BA , Berendt AR , Cavanagh PR , Bus SA , Peters EJ , et al. Unresolved issues in the management of ulcers of the foot in diabetes. Diabet Med 2008 ; 25 : 1380 – 1389.

Growth factors Whereas there is some support for their use for randomized clinical studies, their expense together with the fact that most neuropathic ulcers can be healed with appropriate offloading, have limited their use. Unfortunately, PDGF together with other topically applied agents such as epidermal growth factor do not have sufficient robust data to support their day - to - day use in routine clinical practice. Wieman TJ , Smiell JM , Yachin S . Efficacy and safety of a topical gel formulation of recombinant human platelet - derived growth factor - BB (Becaplermin) in patients with chronic neuropathic diabetic foot ulcers. Diabetes Care 1998 ; 21 : 822 – 827.

Bioengineered skin substitutes Similar to other treatments in this group of adjunctive therapies although there is some evidence to support the use of bioengineered skin substitutes in non - infected neuropathic ulcers, its use of somewhat restricted by cost. A systematic review on this topic concluded that the trials assessed were of questionable quality and until high quality studies were performed, recommendations for the use of these skin substitutes could not be Made. Blozik E , Scherer M. Skin replacement therapies for diabetic foot ulcers: systematic review and meta - analysis. Diabetes Care 2008; 31 : 693 – 694.

Diabetic Foot Ulcer 27 HBO Treatments / 6 ½ Weeks

Diabetes & Osteomyelitis Infected Calcaneous s/p ORIF then external fixation Options: BKA vs HBO 25 yo Diabetic, Standing on two Feet changing oil.

COMPROMISED SURGICAL FLAP Dehisced TMA s/p 30 HBOT’s

Preparation for a Flap or Grafting in a Compromised Patient

WE SAVE LIMBS AND CHANGE LIVES
- Slides: 106