Neurosurgeries Dr Nishan Silva MBBS Head Injuries mechanism
")
Neurosurgeries Dr. Nishan Silva (MBBS)

Head Injuries mechanism morphology severity

MECHANISM • BLUNT INJURY High Velocity Low Velocity • PENETRATING INJURY Gunshot Sharp instruments

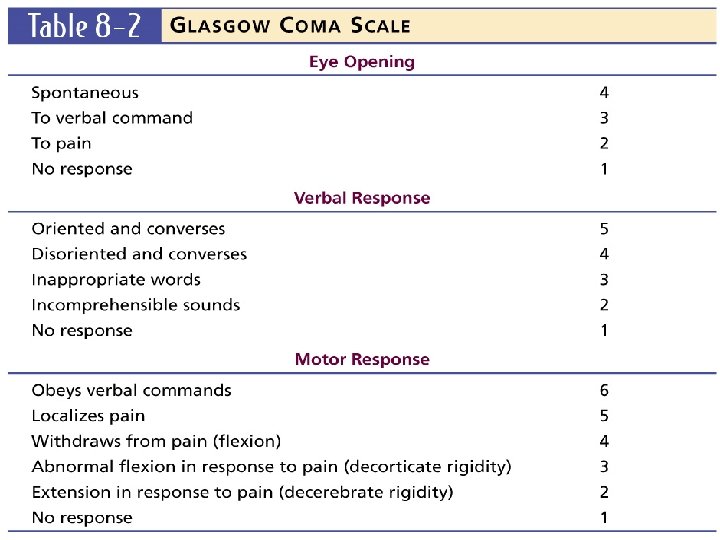
Severity -GLASGOW COMA SCALE ASSESSMENT AREAS SCORE Eye opening 4 Best Motor Response 6 Verbal Response 5 Total Mild Moderate Severe - 15 GCS GCS 13 - 15 9 - 12 3 -8

Intracranial pressure

MORPHOLOGY • SCALP INJURY Cephal Hematoma Subgaleal Hematoma

• SKULL FRACTURES • Vault : linear/stellate depressed/non depressed open/closed

Basilar : with/with out CSF leak with/with out seventh-nerve palsy Battle sign Raccoon eyes CSF rhinorrhea

INTRACRANIAL LESIONS • Focal : epidural hematoma subdural hematoma intracerebral hematoma

Epidural haematoma • Collection of blood & clot b/n dura matter and bones of the skull • Source Middle Meningeal Artery Dural Venous Sinuses • C/F Brief loss of consciousness, headache, drowsiness, dizzy, nausea, vomitting • Rapid clinical deterioration • Talk & die
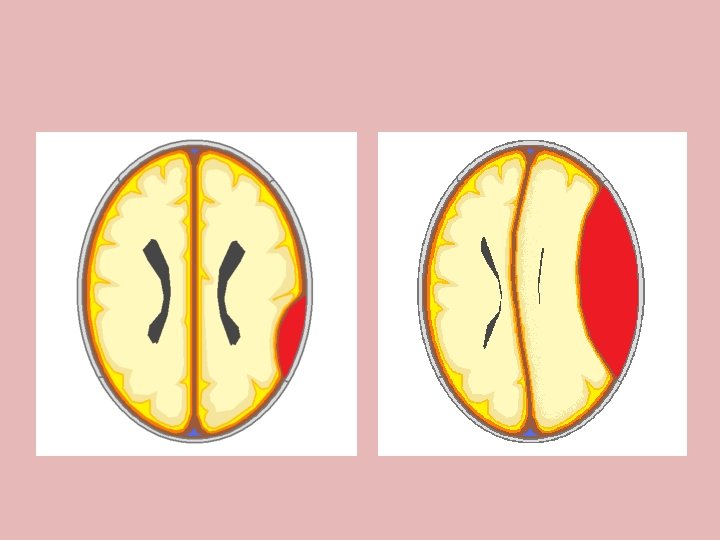

EDH

SDH • Subdural hematomas • Most frequently from tearing of a bridging vein between the cerebral cortex and a draining venous sinus. • - acute - <24 hrs - subacute – 24 hrs-2 wks - chronic - >2 wks Shape. Crescent

Intra Cerebral Heamatoma • Formed within brain tissue & caused by shearing or tensile forces that mechanically stretch and tear deep small caliber arterioles • Most common in temporal and frontal regions • C/F depend on site involved

INTRACRANIAL LESIONS Diffuse : concussion multiple contusion hypoxic/ischemic injury

Concussion • Temporary & brief interruption of neurological function after minor head injury • Due to shearing / stretching of white matter fibres at the time of impact or temporary neuronal dysfunction • C/o headache, confusion, amnesia • CT/MRI cannot detect

DAI • Shearing forces disrupt the axonal fibres in the white matter • Shaken baby syndrome • Blunt trauma • Rapid rise in ICT. • Prolonged or permanent.

APPROACH TO A PATIENT WITH HEAD INJURY • History • Initial Assessment Primary Survey Secondary Survey

PRIMARY SURVEY Airway maintenance with cervical spine protection

Intubation with Cervical inline stabilization • Breathing and ventilation : Intubation precautions Pre-medicate with Lidocaine, 1 mg/kg IV 2 minutes attempt • Laryngoscopy produces an ICP Spike prior to

Circulation • Maintain MAP >90 mmhg- adequate • Hematocrit >30% • Cushing reflex

• Isolated intracranial injuries do not cause hypotension • LOOK FOR THE CAUSE OF HYPOTENSION

Disability • Pupil size Pupillary Changes Irregular shaped Equality? Constricted? Dilated? Vision Problems? • GCS

Early Evaluation Pupillary reactivity and size

SECONDARY SURVEY • AMPLE history • Examination of Head to toe • Glasgow Coma Scale • Detailed Neurological Examination

IMAGING STUDIES ONLY AFTER HEMODYNAMIC STABILIZATION
 • History • General Examination • Limited")
MANAGEMENT OF MILD HEAD INJURY(GCS 13 -15) • History • General Examination • Limited Neurologic Examination • C-spine and other X-rays as indicated • CT scan

CRITERIA FOR ADMISSION • • • No CT scanner available Abnormal CT scan findings All penetrating head injuries Skull fractures CSF leak Deteriorating level of consciousness Moderate to severe headache Significant alcohol / drug intoxication Significant associated injuries

Brain specific monitoring • Brain specific monitoring, including * ICP monitoring * cerebral blood flow (CBF) * Cerebral oxygenation (using either a jugular venous bulb catheter or an oxygen sensitive electrode) * Electroencephalographic (EEG) monitoring can be helpful in postoperative patients in the neuro-ICU.

Brain specific monitoring • Monitoring of ICP is indicated in * Trauma patients with severe brain injury (GCS score < 8), *Abnormalities on the initial CT scan *further in patients with a normal admission CT scan if two or more of the following features are present: Age greater than 40 years, Unilateral or bilateral motor posturing, Systolic blood pressure less than 90 mm Hg. • Routine ICP monitoring is not generally indicated in patients with mild or moderate head injury but may be considered • • • When other severe extracranial injuries are present, Necessitating anesthesia for surgery, When the initial CT scan shows traumatic lesions with space-occupying effects. • ICP monitoring is further indicated in poor grade patients with subarachnoid aneurysmal hemorrhage.

CEREBRAL BLOOD FLOW AND OXYGENATION • Intermittent measurements of CBF can be obtained with stable Xenon CT scanning or positron emission tomography studies. Transcranial Doppler echography provides a noninvasive assessment of blood flow velocity through the basal cerebral arteries. • Global cerebral oxygenation can be assessed using jugular oximetry. • A decrease in jugular venous saturation of oxygen (Sjvo, ) indicates that the brain is extracting more oxygen, suggesting that the J oxygen supply is not adequate for metabolic demands. • Interpretation of results of jugular oximetry require that systemic • information, • such as hemoglobin concentration and arterial saturation, and intracranial data, such as CPP

ELECTRICAL MONITORING • Continuous EEG monitoring has the potential for detecting nonconvulsive status epilepticus in ICU patients. • The value of this monitoring has been shown most often in the setting of stroke and TBI. • As primary monitor of brain function, continuous EEG can be used to titrate continuous infusion of sedative agents, and the technique can further alert the physician to development of focal or global ischemia

TREATMENT OF CEREBRAL HERNIATION AND ELEVATED ICP • Ventricular cerebrospinal fluid drainage (if access is available) • Administration of mannitol, 1 g/kg body weight • Rapid sequence intubation with a neuroprotective strategy ****Lumbar cerebrospinal fluid drainage should never attempted, as this may increase herniation. • Emergency head CT scan should be performed to detect the cause of raised ICP and permit targeted treatment,

INDICATIONS FOR CT SCAN • Skull fracture • Deteriorating GCS • Neurologic deficit • Amnesia, headache • Seizure
 • Initial Examination - Same as for")
MANAGEMENT OF MODERATE HEAD INJURY(GCS 9 -12) • Initial Examination - Same as for mild head injury - CT scan brain – obtained in all cases - Admission for observation • After Admission Frequent Neurologic Checks Improved • Discharge • Follow up Deteriorates (10%) • Repeat CT scan • Manage as per severe head injury protocol
 • Primary Survey and Resuscitation •")
MANAGEMENT OF SEVERE HEAD INJURY(3 - 8 ) • Primary Survey and Resuscitation • Secondary Survey and ‘AMPLE’ history • Admit to facility – neurosurgical care • Neurologic Re-evaluation – Eye opening – Motor response – Verbal response – Pupillary reaction

• • CT scan only after hemodynamic stabilization Medical therapy for raised ICP Immediate neurosurgeon opinion If needed surgical management

MEDICAL THERAPIES FOR HEAD INJURY Head end elevation – 30 deg Intravenous fluids: Maintain normovolemia Hypotonic/glucose containing fluids should not be used • Serum sodium levels monitored daily • •

Conservative therapy of raised ICP • Sedation, analgesia, and mild to moderate hyperventilation (Paco 2 [30 -40 mm Hg]) • Osmotic therapy: preferably mannitol given repeatedly in bolus infusions (dose: 0. 25 -0. 5 glkg body weight, or as indicated by monitoring). Serum osmolarity should be maintained at less than 315 m. Osm/L. If osmotherapy has insufficient effect, furosemide (Lasix) can also be administered. • Cerebrospinal fluid drainage • Volume expansion and inotropes or vasopressors when arterial blood pressure is insufficient to maintain CPP and CBF in a normovolemic patient

Mannitol • • • 0. 25 -1 g/kg Osmotic agent- dec ICP, maintains CBF, CPP and brain metabolism Dec ICP within 6 hrs. Expands volume, O 2 carrying capacity. Diuretic effect- net intravascular volume is reduced.

Furosemide • To reduce ICT in conjunction with mannitol • Dose 0. 3 to 0. 5 mg/kg • Never use in Hypovolemia

HYPERVENTILATION • • • No role as prophylaxis in 24 hrs. Reducing Pa. CO 2 cerebral vasoconstriction Maintain Pa. Co 2 25 – 35 mmhg Last resort for reducing ICP TEMPORARY MEASURE ONLY.

Barbiturates • Effective in reducing ICP – refactory to other measures • Not used in presence of hypotension/hypovolemia

• Anticonvulsants Phenytoin. Loading dose - 18 – 20 mg/kg Maintenance dose - 100 mg q 8 hrly

Surgical management • • Scalp wounds cleaning & debridemant Elevation of depressed Fractures Craniotomy & evacuation of Haematoma Cranial decompression for reduction of ICT

Burr hole evacuation

Brain Surgery • Brain Tumors

Brain Surgery • Brain Tumors – Intraoperative

Brain Surgery

Brain Surgery -Intraoperative

Brain Surgery -Postoperative

Brain Surgery • Aneurysm

Brain Surgery • Aneurysm

Brain Surgery • Aneurysm

Brain Surgery • Traumatic Brain Injury

Brain Surgery • Traumatic Brain Injury

Brain Surgery • Traumatic Brain Injury

Brain Surgery

Brain Surgery • Parkinson’s disease – Deep brain stimulation

Lets see the video examples…

- Slides: 63