Neurosarcoidosis Betsy D Hughes BS J Ned Pruitt

Neurosarcoidosis Betsy D. Hughes, BS, J. Ned Pruitt II, MD, and John R. Vender, MD Contemporary Neurosurgery Vol. 29, Num. 3, Feb. 15, 2007 R石孟申/VS高定憲

Sarcoidosis Inflammatory multisystem disorder n Noncaseating granulomas n Lung: most common n Skin, eyes, liver, lymph nodes n CNS: less common but severe n Isolated CNS lesions: mimic brain and spinal neoplasm. n

Prevalence Age: 20 to 40 y/o n 10 to 40 cases per 100, 000 population in the United States and Europe n African-Americans : Caucasians n – 10: 1 to 17: 1 n Nervous system involvement – 5% to 15%: patients with sarcoidosis – 25%: Postmortem studies

Pathophysiology Non caseaing granuloma: epithelioid macrophages, lymphocytes, monocytes, fibroblasts n Exaggerated cellular immune response n Activation of the Th 1 T lymphocyte cell line. n – By IL-4 and CD 28 – Release INF-r: macrophages

Clinical Manifestations Cranial Neuropathies n Hydrocephalus n Meningeal Disease n Intracranial Parenchymal Disease n Spinal Cord Lesions n Peripheral Neuropathies n Skeletal Muscle Involvement n

Cranial Neuropathies Most common presentation of neurosarcoidosis n Heerfordt syndrome: Acute neurosarcoidosis n – Facial nerve palsy – Parotid gland enlargement – Anterior uveitis – Fever

Hydrocephalus Meningeal involvement n Infiltration of the ependyma or choroid plexus n Intrinsic obstruction of the ventricular system n Communicating or noncommunicating n
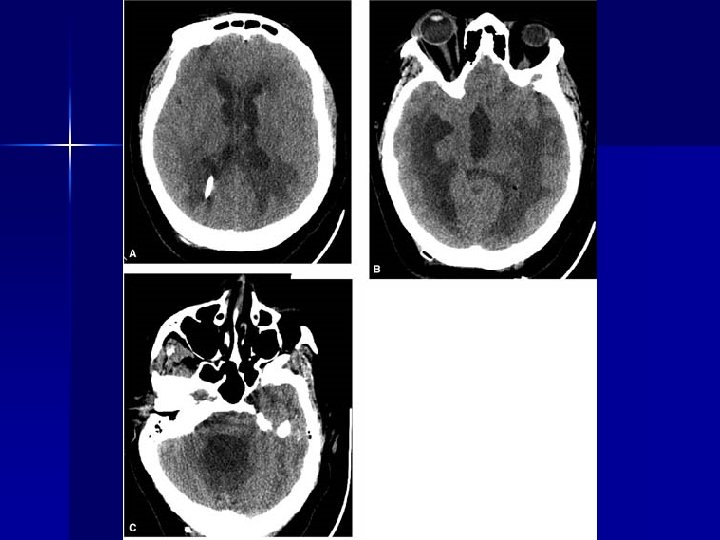

Meningeal Disease n Present like aseptic meningitis or a mass lesion – Pleocytosis: 70% of patients – Elevated Protein: 80% – Reduced glucose: 10% n Thickened, chronic meningitis

Intracranial Parenchymal Disease n Sarcoid encephalopathy – seizures – mood disturbances – cognitive impairment – psychosis – personality changes

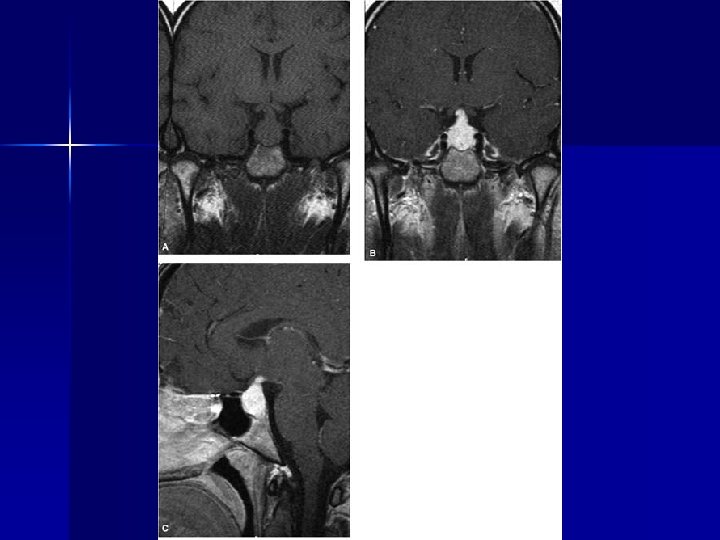
Intracranial Parenchymal Disease n Hypothalamus, infundibulum, and posterior lobe of the pituitary – direct tissue involvement – changes related to adjacent basal meningeal disease n Enhanced MRI can show the enlargement of these structures; – mimic a pituitary tumor or a glioma

Spinal Cord Lesions Cervical and thoracic intramedullary lesions are the most common. n mimic spinal cord neoplasms both clinically and radiologically. n Imaging studies n – Enhancement of the lesions – enlargement of the cord – surrounding edema.

Peripheral Neuropathies Paresthesias and radiculopathy n Sensorimotor, Motor, Sensory n Small or Large n Autonomic n NCV n

Skeletal Muscle Involvement Extremely common and usually asymptomatic n Weakness, pain, and tenderness n Firm, palpable nodules and cramps, with atrophy and contractures n EMG + Muscle biopsy n

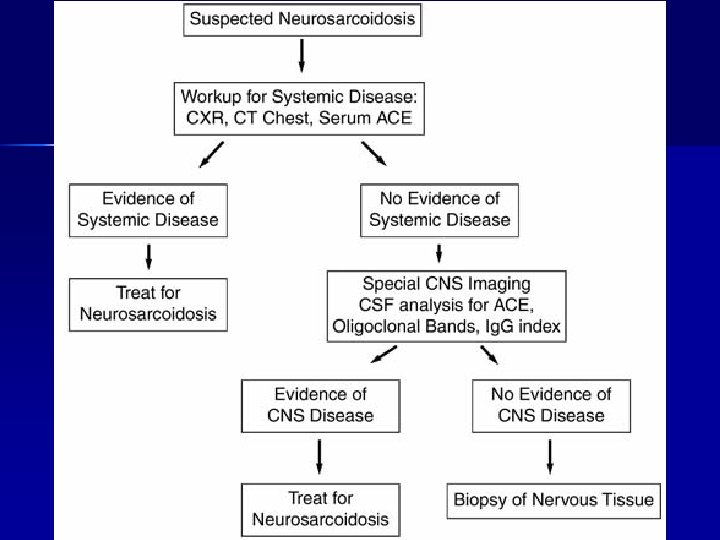
Diagnosis n Zajicek et al. proposed diagnostic criteria for three categories of neurosarcoidosis – Certain neurosarcoidosis – Probable neurosarcoidosis – Possible neurosarcoidosis

Certain Neurosarcoidosis n Biopsy of nervous tissue – noncaseating granulomas n Other possible diagnoses are excluded.

Probable Neurosarcoidosis Clinical presentation n Laboratory evidence demonstrates signs of CNS inflammation n Systemic sarcoidosis. n Other diagnoses are excluded n

Possible Neurosarcoidosis n Clinical presentation n Other diagnoses are excluded

Diagnosis CXR, Chest CT, gallium-67 scan, bronchoalveolar lavage n PFT, Ophthalmologic n Serum ACE (Angiotensin-converting enzyme) n MRI of the muscles, PET, 24 -hr urine calcium, VEP, NCV, EMG n

CNS inflammation Elevation of ACE n Normal to low glucose n Elevated immunoglobulin G n Oligoclonal bands n Elevation of lysozyme and β 2 microglobulin n

Brain MRI n n Most sensitive imaging study for neurosarcoidosis. Irregular leptomeningeal thickening and enhancement – the base of the brain, pituitary and infundibulum. n Periventricular abnormalities, white matter lesions, hydrocephalus, and cranial nerve enhancement.

Treatment n Goal of therapy: – Decrease fibrosis and ischemia of the tissue First-line: corticosteroids n Methotrexate, n infliximab n

Corticosteroids n n n Facial palsy: 1 week of prednisone followed by a 1 -week taper. Parenchymal disease: high-dose prednisone for 2 to 4 weeks, followed by a taper. Severe acute neurological symptoms : IV methylprednisolone for 3 days, followed by 2 to 4 weeks of prednisone with taper.

Surgery n Indications: – Hydrocephalus – Life-threatening mass lesions causing IICP n VP shunt: – Stereotactic guidance – Multiple shunts and revision procedures – Endoscopic fenestration of intraventricular adhesions and septae – Increased infection rate

Conclusion n n Biopsy: after extensive medical and laboratory testing Corticosteroids usually provides a favorable outcome. Aggressive surgical intervention rarely is indicated V-P shunt: appropriate with hydrocephalus secondary to neurosarcoidosis.
- Slides: 27