NEUROPSYCHOLOGICAL EVALUATIONS OF CHILDREN AND ADULTS IN CHILD


 • Differences in focus of: Neuropsychological, Neurological, Psychiatric and Psychological")




 – THE “CULPRIT” IN ALL FORMS OF ADHD •")
 • • (One")
 • Chronic Alcohol/Substance")

 • Review of CBHA")


- Slides: 15
NEUROPSYCHOLOGICAL EVALUATIONS OF CHILDREN AND ADULTS IN CHILD WELFARE CASES Presenter: James E. Lewis, Ph. D. , Clinical Neuropsychologist Florida Children’s Medical Services Suncoast/Pinellas County Child Protection Team A Continuing Education presentation for: Multidisciplinary Dependency Court Professionals Sixth Judicial Circuit of Florida 10 a. m. to 12 Noon Friday, August 14, 2015
OVERVIEW OF SEMINAR • “Let neuroscience help to inform your decisions” -- The “Whole Child” evaluation model • Focus of seminar is on the most frequently occurring neuropsychological disorders in the child welfare system (children and adults) • The Neuroscience Model of evaluation vs. “traditional” mental health assessments • Head injury (TBI) and asphyxia/hypoxia are the leading causes of death and disability in child abuse and neglect statewide and nationwide • High frequency of injuries to children already known to the system – a primary goal is to prevent reabuse
OVERVIEW OF SEMINAR (Continued) • Differences in focus of: Neuropsychological, Neurological, Psychiatric and Psychological Evaluations • Concussion and more severe brain injury, including Shaken Baby cases • Neurotoxicity from Alcohol/Substance Abuse: Adults and Children • Cerebral Hypoxia from Abuse and Neglect – Choking Incidents (Abuse) and near-fatal drowning (supervision neglect) • Components of the neuropsychological evaluation • Risk factors to identify need for Neuropsychological Evaluations
“OLDER” VS. RECENT DEFINITIONS OF CONCUSSION AND “SUBCONCUSSIVE” INJURIES • Lessons from Sports Medicine: so-called “Mild Concussions” not taken seriously until past 5 -10 yrs. • Eliciting concussion history: how not to ask about possible head trauma • Concussion effects are cumulative – multiple “mild” concussive injuries can produce severe and lasting consequences • Most affected functions: Attention (“Acquired” ADHD), Memory, Frontal lobe executive functions • #1 “treatment” – Prevention of reinjury
HYPOXIA/ASPHYXIA IN CHILD ABUSE AND NEGLECT • Definitions: disruption in oxygenated cerebral blood flow • Choking/strangling incidents of adults and children: external pressure on trachea AND pressure on carotid arteries (San Diego study) • Similar neuropsychological sequelae as concussion • Hypoxia from drowning (supervision neglect) vs. inflicted injury (holding child’s head under water) • Neurological studies (EEG, CT, MRI) often show no structural CNS findings but pt. can have major neuropsychological deficits
ALCOHOL AND SUBSTANCE ABUSE – EFFECTS WITH ADULTS • Typical treatment models necessarily focus on addiction and recovery; however, • Underlying neurotoxicity (brain impairment) esp. frontal lobe dysfunction overlooked • Crucial “Differential Diagnosis” issues: • Substance Induced Disorders (drugs or alcohol) “mimic” Bipolar and other Mood Disorders
ALCOHOL AND SUBSTANCE ABUSE – EFFECTS WITH CHILDREN AND ADOLESCENTS • “Older” concept of Fetal Alcohol Syndrome vs. Fetal Alcohol, Drug and Polydrug Exposure • How not to elicit reliable history of Fetal Exposure • Neurodevelopmental and neurobehavioral consequences of Fetal Exposure (Teratogenic Effects) • Dramatic increased risk for Learning and Attention Disorders, Frontal Lobe Executive Function Disorders and Neurobehavioral Disorders • Adolescent Chemical Abuse: the physiological immature brain
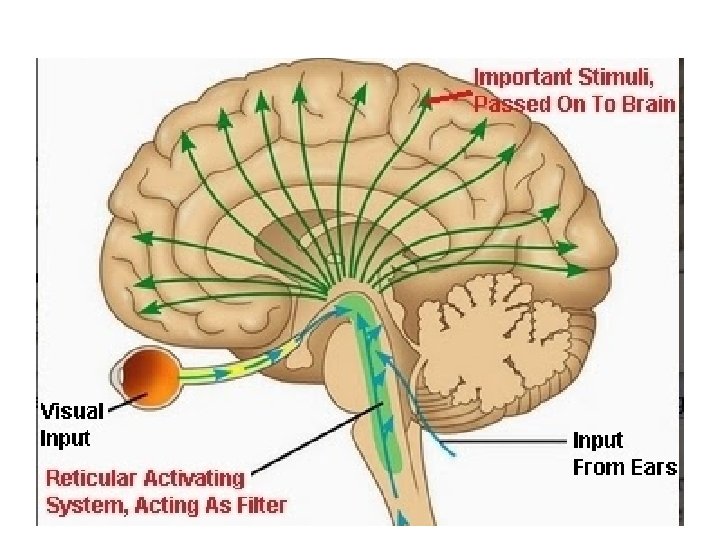
THE RETICULAR ACTIVATING SYSTEM (RAS) – THE “CULPRIT” IN ALL FORMS OF ADHD • Connections between ADHD and increased risk for child abuse • The “vicious cycle” – Fetal Drug and Alcohol Exposure increases risk for ADHD – then increased risk for abuse • The “Two Epidemics” – nationwide extremes of overmedicating some children (example of danger of relying on Parent and Teacher ADHD rating scales) • Opposite extreme of underdiagnosis of the nonhyperactive ADHD Predominantly Inattentive pt. • Brief overview of the four classes of ADHD meds (amphetamine, methylphenidate, Strattera, antihypertensives)
RISK FACTORS TO IDENTIFY NEUROPSYCHOLOGICAL EVALUATION AS A “BEST PRACTICE” (CHILDREN) • • (One or several of these factors present; use best judgment and do careful staffing for best allocation of resources – this is not an all-inclusive listing, just most common) History of a Severe Traumatic Brain Injury (TBI), e. g. motor vehicle/pedestrian accident; sports injury, OR Suspected or confirmed history of repeated “lesser” concussions or choking (hypoxia/asphyxia) in Domestic Violence (“smacks, ” punches or blows to the head or striking the head onto a hard surface) – can have no outright loss of consciousness History of suspected or confirmed Fetal Drug, Polydrug or Alcohol Exposure History of persistent or severe Developmental Delays, e. g. , Intellectual Disability/MR; Severe Learning Disabilities, severe forms of ADHD are causing the “special needs” or “difficult child” to be at increased risk of abuse or neglect; questions of IEP misclassification or IEP inadequacies History of early Failure to Thrive or Shaken Baby brain injury Known diagnosis of neurologic disorder (esp. Epilepsy/Seizure Disorder, congenital brain defects, e. g. recent example of Chiari Defect) History of multiple “traditional” psychological and/or psychiatric evaluations but child/adolescent still has unexplained emotional, behavioral, learning problems
RISK FACTORS TO IDENTIFY NEUROPSYCHOLOGICAL EVALUATION AS A “BEST PRACTICE” (ADULTS) • Chronic Alcohol/Substance Abuse Disorder with concurrent evidence of abuse/neglect of a child • History of TBI, Severe Learning Disabilities, Adult ADHD (TBI may be present in the “Battered Partner/Spouse”) • Suspected or “visible and obvious” cognitive limitations, impaired processing of information, pt. complaints of memory deficits • Previous/known diagnosis of neurologic disorder that can be interfering with safe and appropriate parenting (e. g. Multiple Sclerosis, Epilepsy/Seizure Disorder) • Suspected or confirmed “Co-Occurring Disorder” with treatment noncompliance (Mental Disorder and Alcohol/Substance Disorder) • Caregiver has repeated involvement in child protective services; either chronically noncompliant with services or supports and services “not working, ” past “traditional” psychological and psychiatric evaluations have had limited effectiveness in developing effective treatment
NEUROLOGICAL, PSYCHIATRIC, PSCYHOLOGICAL AND NEUROPSYCHOLOGICAL EVALUATIONS • Neurological evaluations: Physician conducts office examination and laboratory studies (e. g. Brain MRI, Brain CT, EEG. ) Focuses on structural brain damage, disease, defect. Need for neurological examination identified in the neuropsychological evaluation. • Psychiatric Evaluation (M. D. ) – Evaluation for medication, hospitalization, “suitability” for restrictive Residential Treatment Center. Multiple psychiatric evaluations can yield numerous even conflicting/contradictory DSM-5 diagnoses. • “Traditional” Psychological Evaluation of Child or Adult – case history review, cognitive testing, possible academic testing and significant emphasis on personality testing.
THE NEUROPSYCHOLOGICAL EVALUATION IN CHILD WELFARE CASES (CHILDREN AND ADULTS) • Review of CBHA and other case records and reports • Administration of the full core age-appropriate Wechsler Scales (does not use Wechsler Abbreviated Scales), e. g. WAIS-IV for ages 16 to adult; WISC-IV of WISC-V for ages 6 -15; WPPSI-III (Wechsler Preschool and Primary Scales of Intelligence) for ages 3 to 5 years, 11 months • Academic/psychoeducational screening for Learning Disorders with Reading, Written Language and Math subtests of the Woodcock. Johnson Tests of Achievement (WJ-III) • Halstead-Reitan Neuropsychological Testing with the Lateral Dominance Examination, Aphasia Examination, Reitan-Klove Sensory Perceptual Examination and measures of frontal lobe Executive Functioning • Includes Adaptive Functioning Testing for child and adult patients who may be eligible for services with the Florida Agency for Persons with Disabilities • Diagnostic/Clinical Interview and Trauma Assessment
Presenter Contact Information and Additional Sources • Dr. Jim Lewis – cell: 301 -769 -4180 • Email: docjimlewis@gmail. com
BRIEF BIO OF PRESENTER Dr. Jim Lewis is an expert in Child and Adult Clinical Neuropsychology with over 35 years of experience as an evaluator in the child welfare system in Maryland, Washington, D. C. and Florida. In 2002, Dr. Lewis was named “Mid-Atlantic Region Child Welfare Advocate of the Year” by the Child Welfare League of America, the national accreditation organization for public and private Social and Family Services Agencies. While conducting over 8, 000 neuropsychological evaluations of children and adults through private and public agency referrals in clinical private practice, Dr. Lewis has also been a frequent local and national presenter of Continuing Professional Education seminars for the National Model Family Court Program, the Judicial Institute of Maryland, the Florida Statewide Child Protection Team annual conference, the National Drug Endangered Children Conference and television broadcasts on biomechanical force mechanisms and prevention of the Shaken/Impact Baby Syndrome. Dr. Lewis is a Consultant Neuropsychologist Examiner for the Suncoast Center Child Protection Team through Florida Children’s Medical Services and for the Eckerd Community Alternatives programs. Primarily conducting evaluations for Pinellas and Pasco Counties and some evaluations for Manatee County, Dr. Lewis has been qualified before the Florida Sixth Judicial Circuit Court as an Expert in Adult and Child Clinical Neuropsychology and as a Neuropsychologist Expert in Intellectual and Developmental Disabilities.