Neuropharmacologic Interventions in Stroke and Brain Injury Rehabilitation

Neuropharmacologic Interventions in Stroke and Brain Injury Rehabilitation Alan M. Harben, MD, Ph. D Medical Director North Fulton Hospital Rehabilitation Services Restore Neurobehavioral Program

Neuropharmacologic Interventions in Stroke and Brain Injury Rehabilitation None are FDA Approved!

Management of Cognition/Behaviors/ Emotions/Hypertonia/Pain n n Identify problematic cognitive/behavioral/ emotional/motor/tone/pain areas Prioritize problematic areas with respect to functional impact Consider nonpharmacologic solutions such as cognitive testing/remediation, behavioral strategies, and/or psychotherapy Finally, develop a pharmacologic approach considering the effects on all other areas

Cognitive/Behavioral/Emotional/ Tone/Pain Problems n n n Cognition: Hypoarousal, Inattention, Hemineglect, Aphasia, Amnesia Behavior: Agitation, Aggression, Low Frustration Tolerance, Irritability Mood: Depression, Anxiety, Adjustment D/O, PTSD, etc. Hypertonia: Spasticity, Rigidity, Dystonia Pain: local vs. generalized, somatic vs. neuropathic

Neuropharmacologic Management of Cognitive Disorders: Hypoarousal, Inattention, Slow Processing, Hemineglect, Aphasia, Amnesia

Metabolic Encephalopathies Infections: UTI, PNA, Sepsis n Electrolyte Abnls: hypo/hypernatremia n Fluid Abnls: dehydration, A/C renal insufficiency, DM hyperosmolarity n Renal Dysfxn: uremia n Hepatic Dysfxn: hyperammonemia ↓’s DA n Endocrine Dysfxns: DM, hypocortisolism, hypothryoidism n

Iatrogenic Hypoarousal n ALL potentially sedating medications should be evaluated for discontinuation – – – Anticonvulsants: PB, VA, DPH, etc. Antipsychotics: Haldol, Seroquel, etc. Antianxiety Agents: Ativan, Xanax, etc. Antidepressants: TCA, Paxil, etc. Other Medications: Benadryl, etc.
 Produces and maintains general arousal n Originates in midbrain and")
Reticular Activating System (RAS) Produces and maintains general arousal n Originates in midbrain and projects via long axons to the cortex n Coma may be seen with brainstem and/or widespread hemispheric lesions n
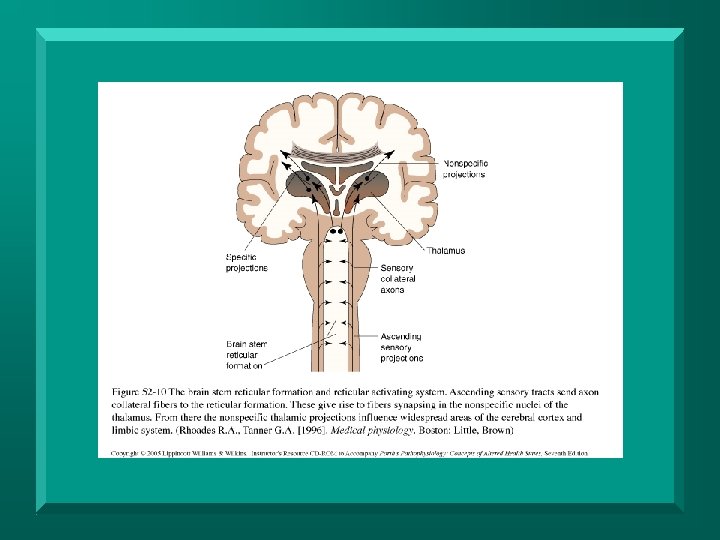

RAS Transmitters n n Dopamine – arousal, attention, hemi-attention, language, memory, perception Norepinephrine – arousal, attention, mood Serotonin – mood, sleep Acetylcholine – memory

Neuropharmacologic Trials Identify target symptoms: cognitive deficits, behaviors, mood d/o’s, hypertonia, and/or pain n Recognize each medication use as a trial n Titrate to effect, monitoring for SE’s n Monitor responses in therapies n Monitor for and minimize drug interactions n

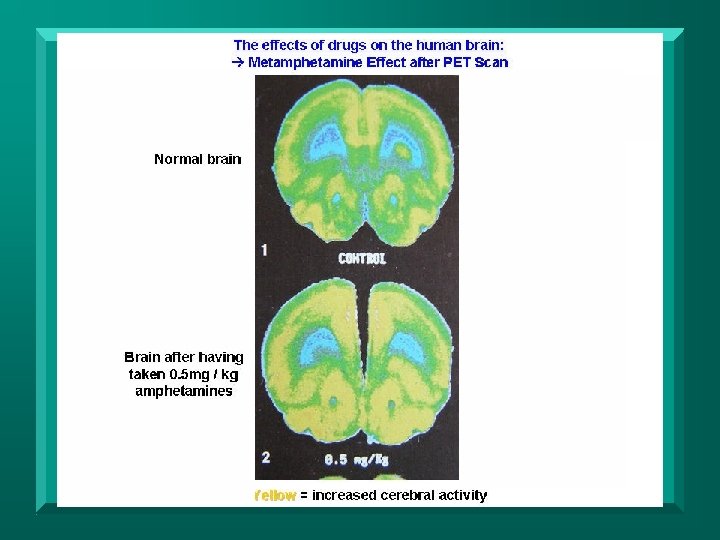
Stimulant Medications n Classic Stimulants – Indicated in ADHD, Narcolepsy – Increase dopamine levels – Increase norepinephrine levels – Improve arousal and attention – Amphetamine (Adderall, Dexedrine) – Methylphenidate (Concerta, Ritalin) • MP structure similar to Cocaine:
 Blocks DA and NE DAT reuptake n Indicated in ADHD, Narcolepsy")
Methylphenidate (Ritalin, etc) Blocks DA and NE DAT reuptake n Indicated in ADHD, Narcolepsy n Too little DA: boredom/distraction n Too much DA: overstimulation/agitation n Right DA: attention/reward/pleasure n SE’s: nervousness, insomnia, CNS overstimulation, anorexia, tachycardia, hypertension n
 Improves arousal via RAS n Improves attention via frontostriatal pathway n")
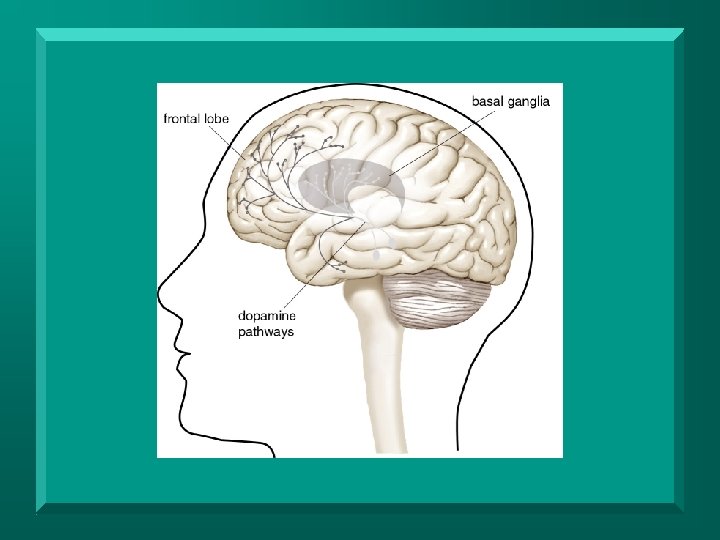
Methylphenidate (Ritalin, etc) Improves arousal via RAS n Improves attention via frontostriatal pathway n Improves processing speed n Improves working (ST) memory via ↑frontal lobe activity n

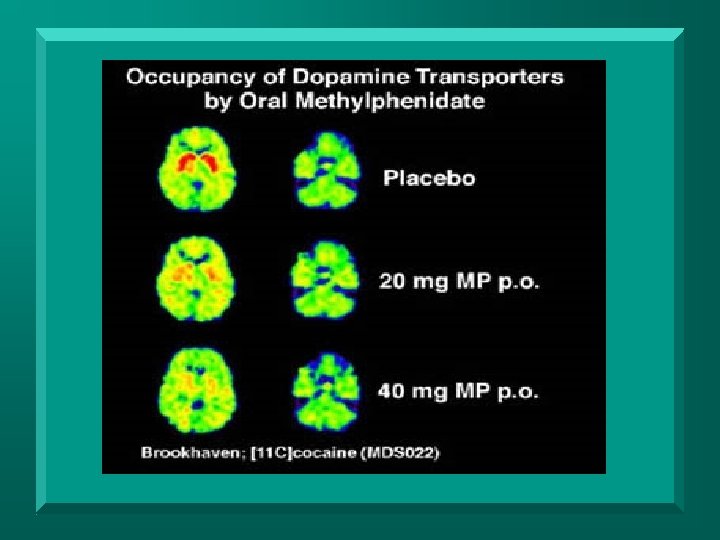
Methylphenidate PET Scan n n Increased DA activity in striatum →
 Blocks DA and NE DAT reuptake n Indicated in ADHD n")
Amphetamine (Adderall, etc) Blocks DA and NE DAT reuptake n Indicated in ADHD n SE’s: nervousness, insomnia, lability, CNS overstimulation, anorexia, tachycardia, hypertension n
 Improves arousal via RAS n Improves language production* n Improves short")
Amphetamine (Adderall, etc) Improves arousal via RAS n Improves language production* n Improves short term working memory, i. e. digit span/manipulation n

DA Stimulant Medications n Dopaminergic Agents – – – Increase or mimic dopamine Indicated in Parkinson’s Disease May improve arousal, attention, hemiattention, and language L-dopa/carbidopa (Sinemet) • dopamine precursor Amantadine (Symmetrel) • – – DA/NE releaser/agonist Bromocriptine (Parlodel) - agonist Ropinirole (Requip) - agonist
 Converted into dopamine n Repletes deficient intracellular DA n – Deficient")
L Dopa (Sinemet) Converted into dopamine n Repletes deficient intracellular DA n – Deficient after CVA, TBI, CNS infections Indicated in Parkinson’s Dz n SE’s: nausea, vomiting, hypotension, confusion, hallucinations n Potentially augments classic stimulants n Consider with bradykinesia n
 DA releaser/agonist in frontal lobes n NMDA glutamatergic receptor antagonist n Indications:")
Amantidine (Symmetrel) DA releaser/agonist in frontal lobes n NMDA glutamatergic receptor antagonist n Indications: Parkinson’s Dz n SE’s: NMS and/or seizures with abrupt withdrawal, nervousness, anxiety, agitation, insomnia, difficulty concentrating n
 Improves arousal n Improves recovery from post-traumatic disorders of consciousness n Improves")
Amantidine (Symmetrel) Improves arousal n Improves recovery from post-traumatic disorders of consciousness n Improves attention n Improves verbal fluency* n Improves general cognition (MMSE) n Decreases agitation* n
 DA agonist at post synaptic D 2 receptors n Not dependent upon")
Bromocriptine (Parlodel) DA agonist at post synaptic D 2 receptors n Not dependent upon pre-synaptic DA n – Lost due to neuronal damage Indications: Parkinson’s Dz, Pituitary D/O’s n SE’s: nausea, vomiting, orthostatic hypotension, and headaches n
 May improve arousal in low level TBI n May improve or worsen")
Bromocriptine (Parlodel) May improve arousal in low level TBI n May improve or worsen hemi-neglect * n May improve fluency and decrease pauses in select aphasia cases * n May improve motivation in frontal lobe injury* n
 • Increases histamine release in the")
Stimulant Medications n Newer Agents – Modafinil (Pro/Nuvigil) • Increases histamine release in the hypothalamic sleep-wake rhythm center • May have DAT blocking activity • Indicated in Narcolepsy, OSA, Sleep D/O’s • SE’s: insomnia, nervousness, HA, rash • Promotes wakefulness • Lower abuse potential

Modafinil PET Scan Increased DA Activity n Placebo Modafinil

Caffeine n Adenosine – an inhibitory neurotransmitter – – – n suppresses CNS activity and arousal promotes sleep levels increasing levels while awake Caffeine - an adenosine receptor antagonist – increases acetylcholine, epinephrine, dopamine, serotonin, norepinephrine and glutamate activity – a reversible acetylcholinesterase inhibitor – acts as a stimulant, improving arousal, attention, concentration

Caffeine n n n Onset within 1 hour, lasts 3 - 5 hours Tolerance develops rapidly as well as clinically significant physical and mental dependence Caffeine abuse, caffeinism, >250 mg/day – anxiousness, irritability, restlessness, insomnia, headaches, and heart palpitations n Withdrawal symptoms – headache, irritability, inattention, drowsiness, and/or insomnia

Caffeine n Pre/Post Caffeine Metabolism

Aphasias May respond to dopaminergic agents n Amantidine n – May increase fluency and word finding* – ~ 30% n Bromocriptine – May increase word finding and decrease pauses*

Hemi-Neglect Right parietal/TP jxn lesions → left neglect n May respond to dopaminergic agents: n – L dopa, amantidine, bromocriptine – Increased left sided awareness* – Improved midline orientation – May worsen via contralateral overstimulation

Post-Traumatic Amnesia n Hippocampal, thalamic, temporal and other cortical lesions – due to trauma and/or anoxia n Deficiency in acetylcholine levels
")
Acetylcholinesterase Inhibitors AI’s block breakdown of acetylcholine to Ach synaptic levels n Donepezil (Aricept) n Rivastigmine (Exelon) n – also butrylcholinesterase inhibitor to ACh n Galantamine (Razadyne) – also acts on nicotinic receptors to release acetylcholine n SE’s: nausea, vomiting, diarrhea, anorexia, abdominal pain, bradycardia

Acetylcholinesterase Inhibitors Indications: Alzheimer’s Dementia n Alzheimer’s Dementia: increased attention, memory, language, and reasoning; decreased confusion → ↑basic ADL’s, better behavior n – Slows progression of dementia by 6 -12 months n Vascular Dementia: similar effects

Acetylcholinesterase Inhibitors TBI: increased attention and concentration → improved general cognition* n TBI: improved immediate and delayed memory n
 n n n NMDA glutamatergic receptor antagonist regulates glutamate in the brain,")
Memantine (Namenda) n n n NMDA glutamatergic receptor antagonist regulates glutamate in the brain, decreasing abnormal activity D 2 DA receptor agonist Indications: Alzheimer’s Dementia SE’s: confusion, dizziness, headache, insomnia, agitation, and/or hallucinations Improves information processing, and clears thinking → ↑basic ADL’s
 n Mild TBI: improved attention, fluency, memory, and processing speed")
Memantine (Namenda) n Mild TBI: improved attention, fluency, memory, and processing speed

Neuropharmacologic Management of Behavioral Disorders: Agitation, Aggression, Irritability, Frustration

Agitation n Definitions – Delirium: syndrome including fluctuating arousal, inattention, and cognitive impairments – PT Agitation: delirium with PTA and behaviors including aggression, restlessness, disinhibition, and/or emotional lability – Psychosis: disorder including perceptual impairments (hallucinations) and/or fixed false beliefs (delusions)

Agitation: Incidence • 40% in acute severe TBI • transient • less common in chronic TBI, < 5% • more disabling

Agitation: Neuropathology No precise localization n Frontal and temporal lobe lesions n Disinhibition and emotional lability: orbitofrontal injury n

Agitation: Neurotransmitters n Catecholamines: dopamine and norepinephrine – affect arousal and attention – decreased levels in agitated patients n Serotonin – regulates mood and behavior – decreased CSF metabolite levels are related to aggressive behavior – decreased levels in CSF of TBI patients n Acetylcholine: affects memory – adrenergic/cholinergic/serotoninergic balance affects mood

Agitation: Behavioral Treatment n Behavioral Interventions – Controlled environmental stimulation • Structure sensory input – Behavioral modifications • Based on learning consequences of behaviors • Manipulation of events either pre- or post - behavior – Restraint - only when patient and/or staff at risk for injury
 GABA receptors, agonist –")
Agitation: Pharmacologic Interventions n Benzodiazepines – increase affinity of (inhibitory) GABA receptors, agonist – indications • • • anxiety agitation with anxiety violent agitation – adverse effects • • • sedation frontal lobe disinhibition, may worsen behavior seizures with abrupt withdrawal
 – D 2 dopamine receptor blockers, newer")
Agitation: Pharmacologic Interventions n Antipsychotics (Major Tranquilizers) – D 2 dopamine receptor blockers, newer agents are serotonin blockers – Indications: psychosis, violent agitation/aggression, mood stabilization, depression

Agitation: Pharmacologic Interventions n Antipsychotic Adverse Effects – sedation – extrapyramidal signs - dopamine deficiency – tardive dyskinesia - dopamine hypersensitivity – Neuroleptic Malignant Syndrome (NMS) • hyperadrenergic state (autonomic arousal), HTN, tachycardia, fever, sweating, rigidity, CPK
 • motor effects, weight gain,")
Agitation: Pharmacologic Interventions n Atypical Antipsychotics – Risperidone (Risperdal) • motor effects, weight gain, sedation – Olanzapine (Zyprexa) • weight gain, diabetes, fewer motor effects, sedation – Quetiapine (Seroquel) • less weight gain, fewer motor effects, sedation – Ziprasidone (Geodon) • no weight gain, fewer motor effects, sedation – Aripiprazole (Abilify) • no weight gain, fewer motor effects ? , no sedation

Agitation: Pharmacologic Interventions n n Agitation with hypoarousal and/or inattention Dopaminergic Agents – L-dopa (Sinemet), Amantadine (Symmetrel) releaser/agonist – Adverse reactions • nausea and vomiting, dizziness, insomnia, irritability, psychosis n Classic Catecholamine Stimulants – Methylphenidate (Concerta, Ritalin), Amphetamine (Adderall, Dexedrine) – Adverse effects • insomnia, irritability, agitation, psychosis
 – No controlled studies")
Agitation: Pharmacologic Interventions n Anticonvulsants – Mood stabilizers (bipolar treatment) – No controlled studies in PT agitation – Indications • agitation, impulse control disorders, bipolar disorder, mania, epilepsy, headache
, Oxcarbazepine (Trileptal) – Adverse effects: cognitive impairment, sedation, drug metabolism")
Anticonvulsants n Carbamazepine (Tegretol), Oxcarbazepine (Trileptal) – Adverse effects: cognitive impairment, sedation, drug metabolism interactions, leukopenia (rare), rash (15%), Stevens-Johnson Syndrome (<1%), dizziness, hyponatemia n Valproic Acid (Depakote) – Increases GABA levels, agonist – Adverse effects: hepatotoxicity, pancreatitis (children), weight gain n Lamotrigine (Lamictal) – Adverse effects: rash, dizziness n Topiramate (Topamax) – Adverse effects: weight loss, glaucoma, cognitive impairment n Levetiracetam (Keppra) – Adverse effects: sedation, dizziness

Agitation: Pharmacologic Interventions n n n SSRI’s - Zoloft, Lexapro, Prozac, Paxil, etc. SNRI’s – Effexor, Cymbalta Indications – agitation – depression, anxiety, PTSD n Adverse effects – overstimulation, insomnia, anxiety, sedation, impotence, tremor, GI upset, HTN, drug metabolism interactions

Acute Agitation Decision Tree Behavioral Interventions Short Term IM Pharmacologic Interventions Short Acting Benzodiazepine IM-Ativan Antipsychotics Geodon IM Zydis SL Behavioral Interventions Longer Term Pharmacologic Interventions Cognitive Agents SSRI's, Mood Stabilizers Atypical Antipsychotics A. Harben, MD, Ph. D

Chronic Agitation Decision Tree A. Harben, MD, Ph. D

Summary n n Identify problematic cognitive/behavioral/ emotional/motor/pain areas Prioritize problematic areas with respect to functional impact Consider nonpharmacologic solutions such as cognitive testing/remediation, behavioral strategies, and/or psychotherapy Finally, develop a pharmacologic approach considering the effects on all other areas

Summary Recognize each medication use as a trial n Titrate to effect, monitoring for SE’s n Monitor responses in therapies n Monitor for and minimize drug interactions n
- Slides: 58