Neuroophthalmology Abdulrahman AlMuammar College of Medicine King Saud

Neuro-ophthalmology Abdulrahman Al-Muammar College of Medicine King Saud University

Neuro-ophthalmology Objectives: • Recognize and interpret the common signs and symptoms of neuro-ophthalmic disorders Obtain appropriate history Measure visual acuity Examine pupillary reaction Test the function of the extraocular muscles Evaluate the visual fields Inspect the optic nerve head

Neuro-ophthalmology Pupil Ocular motor system Visual fields Common neuro-ophthalmic disorders

Pupillary size is determined by number of factors including Age Level of alertness Level of retinal illumination Accommodative effort

Pupil Anatomy of pupillary pathway Afferent limb Efferent limb • Parasympathetic pathway • Sympathetic pathway Near response

Pupil

Pathway of pupillary reaction to light

Sympathetic pathway
")
Afferent pupillary defect (APD)
")
Afferent pupillary defect (APD)

Causes of APD Optic nerve disease Significant retinal disease Amblyopia

Efferent pupillary defect

Anisocoria

Anisocoria
 (small pupil)")
Anisocoria Pupillary inequality greatest In bright light In dim light (large pupil) (small pupil) 3 rd nerve palsy Ptosis Trauma Horner syndrome Tumor Physiological Temporal lobe herniation Aneurysm No 3 rd nerve palsy Drug induced Adie’s pupil Iris damage (trauma/surgery/laser) Basal meningitis

Anisocoria

Horner syndrome

Ocular motor system

Ocular motor system

Ocular motor system

3 rd nerve palsy + ve pupillary involvement An incomplete III palsy which progress Other neurological signs No resolution in 3 months Aberrant regeneration appears Emergency Do MRI, MRA If negative do catheter angiography To r/o compressive lesion: aneurysm, tumor Other possible causes : vasculopathy, trauma, inflammatory, demyelination, infectious, MG, congenital

Ocular motor system

4 th nerve palsy Most frequent cause is trauma If no trauma, isolated 4 th nerve palsy then most likely vasculopathic ( Do BP, BS) +ve trauma, any other neurological signs, normal BP/BS or palsy lasting > 3 months then MRI is needed.

Ocular motor system

6 th nerve palsy Isolated 6 th nerve palsy most likely vasculopathic ( do BP/BS) Normal BP/BS, other neurological signs, trauma, or palsy > 3 months then do MRI

Visual system

Visual system

Visual system

Visual fields defect

Visual fields defect

Visual fields defect

Visual fields defect

Visual fields defect

Visual fields defect

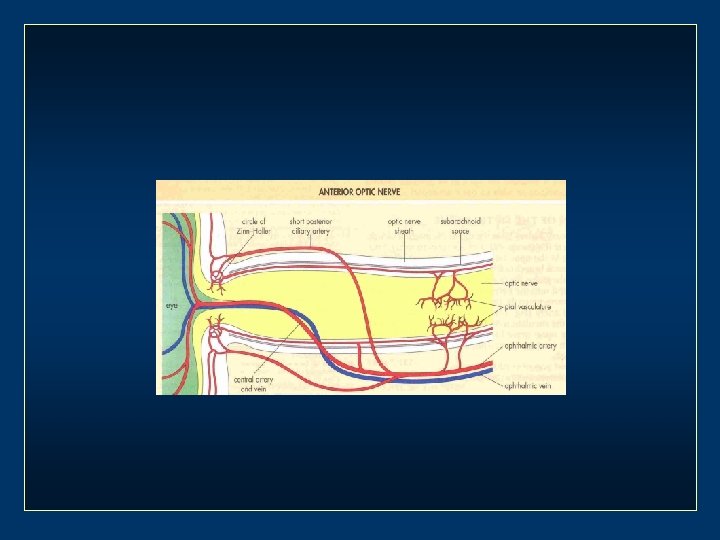
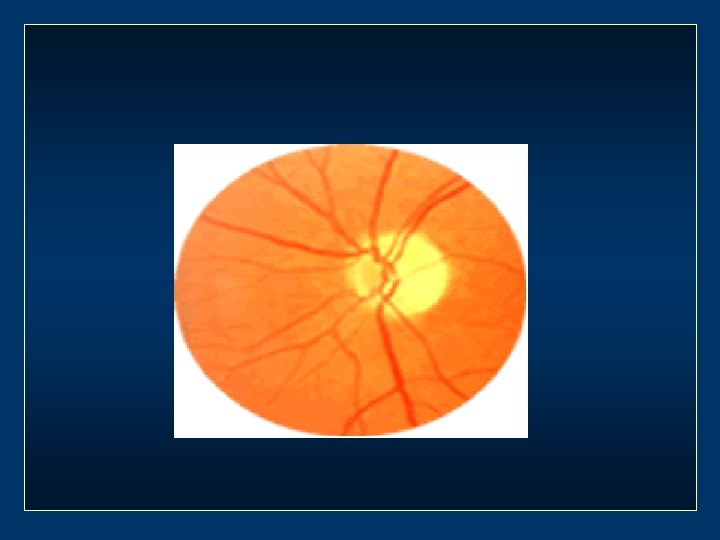
Optic disc


Disc swelling Mechanical signs Elevation Blurred margins Peripapillary edema Choroid folds Vascular signs Hyperemia Venous dilation Disc hemorrhage NFL infarcts Exudates

Causes of disc swelling Increased intracranial pressure Ischemic optic neuropathy Optic neuritis Central retinal vein occlusion Nutritional optic neuropathy Toxic optic neuropathy ETOH-ethanol-Digitalis. Ethambutol -Chloramphenicol. INH Tumor Infiltrative Orbital Pseudotumor Thyroid orbitopathy

Amaurosis Fugax Transient monocular visual loss or dimming May last from 2 -3 minutes to 30 minutes or more Due to decrease blood flow to the eye Causes: • Carotid atheroma • Cardiac valvular disease • Atrial myxoma • Retinal migraine • Giant cell arteritis • Hyperviscousity syndromes
 Chronic auto-immune disorder characterized by presence of antibodies which block the")
Myasthenia Gravis (MG) Chronic auto-immune disorder characterized by presence of antibodies which block the ACH receptor sites It can affect any muscle Eye signs are the presenting signs in 50% of the patients • • Ptosis Any ocular motility disturbances INO Variability is the hallmoark
 Diagnosis • • Clinically Pharmacologically (Tensilon test) Serologically Sleep test Ice-pack")
Myasthenia Gravis (MG) Diagnosis • • Clinically Pharmacologically (Tensilon test) Serologically Sleep test Ice-pack test CT chest Thyroid function test ANA Treatment • • • Acetylcholinesterase inhibitors Steroid Immunosuppressant Plasmapheresis Thymectomy
 frequently have visual complaints Cerebellar dysfunction Motor")
Multiple sclerosis Patients with multiple sclerosis (MS) frequently have visual complaints Cerebellar dysfunction Motor symptoms Sensory symptoms Mental changes Sphincter disturbances

Multiple sclerosis Ocular complications: Optic neuritis Chiasmal and retro chiasmal abnormalities Ocular motility disturbances Treatment Steroid Interferon

Thank you
- Slides: 46