Neuromuscular Blocking Agents Harold Griffith Depolarizing succinylcholine activate

Neuromuscular Blocking Agents

Harold Griffith
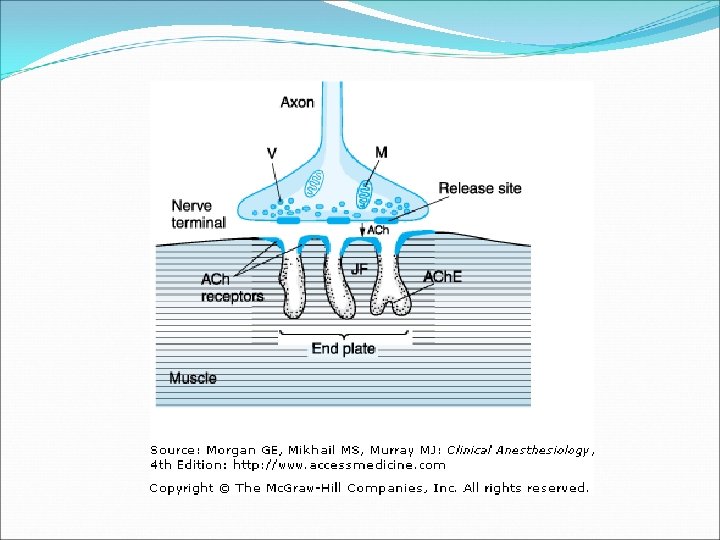

�Depolarizing: -succinylcholine - activate Ac. H receptors - resemble acetylcholine -continuous stimulation -diffuse from NMJ -rapidly hydrolyzed -pseudocholinesterase
 �Short half-life-duration 6 -10 min")
Succinyholine �Emergency setting �Rapid onset (45 -60 sec) �Short half-life-duration 6 -10 min

Contraindications �Personal/family h/o malignant hyperthermia �Risk of sever hyperkalemia: rhabdomyolysis Ach receptor upregulation -denervating injury -denervating disease -inherited myopathies -burns after 72 h -severe infections with exotoxin production -prolonged total body immobilization
 �Fasciculation �Bradycardia �Increased intraocular pressure")
Complications �Trismus (0. 001 -0. 1%) �Fasciculation �Bradycardia �Increased intraocular pressure

Rapid Sequence Intubation 1971 Rosen, Canada

Mallampati classification of oral opening Grading of laryngeal view

RSI. �Retrospective, 1996 -2006 � 1, 24 h after arrival to ER �RSI+direct laryngoscopy – standard approach � 1 st h-6088 patients – 21(0. 3%) surgical airway �Fisrt 24 h – 32. 000 patients – 31(0. 1%) surgical airway The Success of Emergency Endotracheal Intubation in Trauma Experience at a Major Adult Trauma Referral center. Baltimore. Anesthesia and Analgesia. 109. 2009

RSI � Prospective observational, multicenter � 2 years � Compare anesthesiologist vs. ER physician � 439 trauma patients – 233 RSI – 3 attempts – 100% success � No significant difference in complication rates for RSI : -esophageal intubation -endobronchial intubation -aspiration -critical desaturation -hypotensive episode Rapid Sequence Intubation of Trauma Patients in Scotland. J. Trauma 2004, p 1123 -26

RSI �Observational study � 1995 -1996 � 610 patients � 515 RSI, 99. 2% intubations - successful �ED physicians Airway management in the emergency department: a one-year study of 610 tracheal intubations. Annals of Emergency Medicine-Vol 31, Issue 3, March 1998 University of California

Non-depolarizing NMBAs in RSI �Malignant hyperthermia �Neuromuscular disease �Muscular dystrophy �Stroke over 72 hours old �Rhabdomyolysis �Burn over 72 hours old �Significant hyperkalemia

� Rocuronium versus succinylcholine for rapid sequence intubation of anesthesia and endotracheal intubation: prospective, randomized trial in emergent cases. Anesthesia and Analgesia, 2005 � Non-blinded, randomized, controlled trial � 180 randomized patients � Intubating conditions were assessed by anesthesiologist � Numerical scale 9 points � Priority for Sch � Time intubation-median time � Sch-95 sec � Rocuronium 130 sec Rocuronium vs. succinylcholine in the emergency department: a critical appraisal. William K. Mallon… The Journal of Emergency Medicine. Vol 37, 2009
 for use during rapid sequence induction anesthesia. Anaesthesia")
� Comparison of rocuronium and suxamethonium(Sch) for use during rapid sequence induction anesthesia. Anaesthesia , 1998 � Randomized, double-blinded, controlled trial � 314 patients � Excellent, good, poor � Emergent or elective surgery � Rocuronium 1. 0 mg/kg better then 0. 6 mg/kg � Intubating conditions rocuronium=Sch but � Execllent grade Sch Rocuronium vs. succinylcholine in the emergency department: a critical appraisal. William K. Mallon… The Journal of Emergency Medicine. Vol 37, 2009

�A comparison of succinylcholine and rocuronium for rapid sequence intubation of emergency department patients. Academic emergency Medicine, 2000 �Prospective cohort study � 520 patinets in ED �Three 10 -point numerical scales: -body movement- Sch less body movement -vocal cord movements - the same -physician’s satisfaction - Sch better �Sch faster Rocuronium vs. succinylcholine in the emergency department: a critical appraisal. William K. Mallon… The Journal of Emergency Medicine. Vol 37, 2009

� Rocuronium versus succinylcholine for rapid sequence induction untubation. Cohrane Database of Systematic Reviews, 2008 (10) � Systematic review, August 20, 2007 � 37 studies for analysis, n=2690 � Randomized controlled clinical trials � Controlled clinical trials � No statistical difference in intubation conditions � Sch is clinically superior – shorter duration of action � Propofol+Sch better intubation conditions then Propofol+Rocuronium vs. succinylcholine in the emergency department: a critical appraisal. William K. Mallon… The Journal of Emergency Medicine. Vol 37, 2009

Conclusion �Sch-the drug of choice for ED RSI �Unless - contraindicated Rocuronium vs. succinylcholine in the emergency department: a critical appraisal. William K. Mallon… The Journal of Emergency Medicine. Vol 37, 2009
 programs (directors) � 98. 9%-RSI protocol � 90% - use Sch")
�Responded 89 (182) programs (directors) � 98. 9%-RSI protocol � 90% - use Sch � 70% - use long-acting NMB � 77%-mandatory in-flight sedation � 13% - maintenance in-flight paralytics �GCS-3 - 97% long-acting NMB for even short transportation Emergency airway management in critically injured patients: a survey of U. S. aero-medical transport programs. Resuscitation 80 (2009)

Nondepolarizing neuromuscular blocking agents in ICU �Decreased-20 years �Last resort �To facilitate mechanical ventilation �Trained ICU staff

Nondepolarizing neuromuscular blocking agents � Nondepolarizing: -competitive antagonist Ac. H -prevents depolarization -no side effects of depolarizing agents � Aminosteroidal compounds : -pancuroium -pipecuroinium -vecuronium -rocuronium � Benzylisoquinolinium compounds: -D-Tubocurarine - 1 st – not in use -atracurium -cisatracurium -doxacurium -mivacurium Critical practice guidelines for sustained neuromuscular blockade in the adult critically ill patient. Critical Care Medicine 2002 Vol. 30 No. 1

Indications for long-term administrations � Facilitations of mechanical ventilations No study comparing NMB’s to placebo � Control ICP in TBI No control study � Ablation of muscle spasm in tetanus Case studies � Decreasing oxygen consumption � No direct effect on seizures-facilitation of ventilation only Critical practice guidelines for sustained neuromuscular blockade in the adult critically ill patient. Critical Care Medicine 2002 Vol. 30 No. 1

Need for NMBAs? • Mechanical ventilation • Tetanus • High ICP Yes Is the patient adequately sedated? No Yes Still need for NMBAs Yes Contraindication to vagolytic drug? No Optimize sedatives and analgesics No Continue sedatives and analgesics Yes Hepatic or renal dysfunction? Avoid pancuronium if hepatic or renal dysfunction use atracrium or cistracurium Yes No Pancuronium bolus/infusion? Ciatracurium/atracurium bolus/infusion Critical practice guidelines for sustained neuromuscular blockade in the adult critically ill patient. Critical Care Medicine 2002 Vol. 30 No. 1

Recommendation � Adult in ICU � Manage ventilation � Manage patients with increased ICP � Treat muscle spasm � Manage decreased oxygen consumption � When all other means –no success � Grade of recommendations = C Critical practice guidelines for sustained neuromuscular blockade in the adult critically ill patient. Critical Care Medicine 2002 Vol. 30 No. 1
-not pancuronium=C �")
Recommendations � Pancuronium = B � Contraindication to vagolysis (heart dis. )-not pancuronium=C � Significant hepatic and renal diseases-cisatrcurium, atrcurium=B � Monitoring clinical/TOF-1 -2 twitches=C � Prior to NMB sedation, analgesia=C � NMB and steroids- stop ASAP=C � Drug holidays decreases AQMS=C � Prophylactic eye care/DVT proph. =B � Tachyphilaxis to one NBM, try another=C Critical practice guidelines for sustained neuromuscular blockade in the adult critically ill patient. Critical Care Medicine 2002 Vol. 30 No. 1
: -pancuronium 3 -hydroxypancuronium")
Prolong weakness �Accumulation of NMB agent or active metabolite (renal/hepatic dysfunction): -pancuronium 3 -hydroxypancuronium -vecuronium - 3 -desacetylvecuronium �Myopathy: -acute paresis -myonecrosis -EMG: denervation Role of analgesics, sedatives, neuromuscular blockers and delirium. Critical Care Medicine, Oct 2009. Jesse B. Hall…

�Last decade –decreased the use of NMB’s-ICUAW �Facilitation of Intubation �Patient ventilator asynchrony-targets of ventilation �Cisatracurium Role of analgesics, sedatives, neuromuscular blockers and delirium. Critical Care Medicine, Oct 2009. Jesse B. Hall…

� Persistent paralysis in critically ill patients after long-term administartion of vecuronium. NEJM, 1992, 327, University of California � 8 men, 8 women � Vecuronium for at least 2 days to facilitate mechanical ventilation � Clinical factors, plasma concentration of vecuronium and 3 -desacetylvecuronium � 7 patients - 6 h -7 days paralysis � Higher plasma magnesium � Lower p. H � Higher 3 -desacetylvecuronium � Higher frequency of renal failure Intensive care unit-acquired weakness: Risk factors and prevention. Crit Care Med 2009, vol 37(10)

� A retrospective cohort study, 2 hospitals � 1985 -1995, 86 patients, 94 episodes of asthma � Asthma required mechanical ventilation � NMBAs – in patients admissions � Muscle paralysis 3. 1± 2. 3 days � 9 (30%)patient significant myopathy -EMG � Multiple logistic regression model-long NMBAs use=myopathy Myopathy Following Mechanical Ventilation for Acute Severe Asthma. The role of Muscle Relaxants and Steroids. Chest 1999; 115. Vancouver Hospital, St. Paul’s Hospital, Canada

ICU-Aquired Weakness. William D. Schweickert. Chest, 2007, 131

Prospective, multicenter, international cohort � 20 countries, 361 ICU � 5, 183 patients-mechanical ventilated >12 H � 3, 540 – sedated � Mechanical ventilation >12 h Median – 3 days ( 2 -6 days ) � More sedation-more ventilation days � More weaning days � Longer ICU stay � 686 (13%) – NMB’s for at least 1 day � Median – 2 days (1 -4), 8% days of mechanical ventilation Use of Sedatives and Neuromuscular Blockers in a Cohort of Patients Receiving Mechanical Ventilation. Chest 2005, 128 University of Texas Health Science Center at San Antonio

� Factors independently related to use of NMBs: -age<50 -male -normal previous functional status -reasone: ARDS more -less likely in coma, neuromusc diseases, postop, resp. failure -full ventilatory support -permissive hypercapnia -prone position -high PEEP -high airway pressure � The use of NMB’s: -longer MV median 7 days vs. 3 -weaning time 1 -6 vs. 1 -3 -ICU stay 10 vs 7 -higher mortality-50%-independently related to mortality in ICU Use of Sedatives and Neuromuscular Blockers in a Cohort of Patients Receiving Mechanical Ventilation. Chest 2005, 128 University of Texas Health Science Center at San Antonio

�MOF �Muscle immobilization �Hyperglycemia �Corticosteroids �NMBAs Intensive care unit-acquired weakness: Risk factors and prevention. Crit Care Med 2009, vol 37(10)

�NMBAs: Direct muscular toxicity Increase susceptibility to corticosteroids �Recent changes: -intermittent blouses -use NMBA independent from renal/liver metabolism -monitoring Intensive care unit-acquired weakness: Risk factors and prevention. Crit Care Med 2009, vol 37(10)

NMB monitoring-national surveys �UK-62% physicians never used peripheral nerve stimulator �<10%-used on a routine base �Routine monitoring: -Denmark-43% -Germany-28% -Mexico-2% Neuromuscular monitoring: Old issues, new controversies. Aaron F. Kopman. Journal of Critical Care, 2009, Vol. 24

Clinical tests � 1949 - ” 5 seconds head lift”, animal studies � 1961 -64, 89 human studies � 1970, 1988 “HL” test criticized-insensitive � � 1952 -maximal expiratory flow � 1959 -maximal negative inspiratory force Neuromuscular monitoring: Old issues, new controversies. Aaron F. Kopman. Journal of Critical Care, 2009, Vol. 24

Evoked mechanical responses � 1958. The St. Thomas’s hospital nerve stimulator in the diagnosis of prolonged apnea. Lancet 1958. London �Twitch-3/sec or tetanus 50/sec.

TOF � 1970, 1971 -1 st description � 1973 for the 1 st time TOF-0. 7 � 8 healthy persons �VC, Inspiratory force decrease significantly – 0. 6 and 0. 7 The effect of d-tubocurarnie on indirectly elicited train-of four muscle responses and respiratory measurements in humans. Ali…Br J Anaesth 1973

• Peripheral nerve stimulator • A current variable frequency/amplitude • A pair of electrodes • Ulnar nerve-adductor pollicis contraction • Facial nerve-orbicularis oculi contraction Train-of-four • 4 successive 200μs stimuli in 2 s (2 Hz) • Ratio 1 st to 4 th decreases as relaxation increases • Absent of : 4 th twitch – 75%block 3 rd 80% 2 nd 90% • TOF>0. 9 -clinical recovery (past >0. 7)
-50 Hz/5 sec-3 sec-1 Hz �Tetany at 50 -100 Hz-sustained contraction for")
�Post-tetanic count (PTC)-50 Hz/5 sec-3 sec-1 Hz �Tetany at 50 -100 Hz-sustained contraction for 5 secreversal NMB �Double-burst stimulation: -DBS 3, 3 -3 - 200μs stimuli separated by 20 -ms intervals -pause 750 ms - 3 - 200μs stimuli separated by 20 -ms intervals �DBS 3, 2

Use in ICU � Trained ICU staff � Airway control � Mechanical ventilatory support � Adequate sedation � Adequate analgesia � Monitoring � Protect eyes � Protect pressure points � DVT prophylaxis

The Ideal NMBA �Early, tytratable paralysis �Rapid offset of action �No adverse physiologic effect �Elimination independent of hepatic/renal �Inactive metabolites �No accumulation �Modest cost

�Paralyze skeletal muscle �No: -sedative amnestic analgesic prevent muscle contracting �In ICU: improve patient-ventilator synchrony �Enhance gas exchange �Diminish the risk of barotrauma

� Table 1 The effect of d-tubocurarine on respiratory � mechanics at several TOF ratios in human volunteers [23] � TOF � ratio � Vital � capacity a � Negative � inspiratory force a � Peak expiratory � flow rate a � 0. 60 91. 2 70. 3 95 � 0. 70 96. 5 81. 6 92. 2 � 0. 80 99. 9 87. 9 94. 1 � 0. 90 99. 5 90. 9 94. 5 � 1. 00 99. 7 96. 6 99. 2

Suggamadex � 1 st Selective relaxant binding agent-for reversal of NMB by rocuronium and other steroidal NDNMB � 18 RCTs- 1321 patients �Adverse effect <1%, the same for placebo, neostigmine �Conclusion-Sugg. Is effective in reversing rocuronium-induced NMB Sugammadex, a selective reversal medication for preventing postoperative residual neuromuscular blockade. Cochrane Database Syst Rev 2009 Oct 7
- Slides: 45