Neurology Update Paul Hart Neurologist l Epsom St








































- Slides: 42
Neurology Update Paul Hart Neurologist l. Epsom + St Helier l. AMNU @ St George’s l. Royal Marsden Hospital
Neurology Update l Diseases l l l l Parkinsons disease Multiple Sclerosis Epilepsy Stroke Dementia Headache ……. .
Neurology Update l Diseases l l l l Parkinsons disease Multiple Sclerosis Epilepsy Stroke Dementia Headache ……. . Germline mosaicism of MPZ gene in Dejerine-Sottas syndrome (HMSN III) associated with hereditary stomatocytosis Neuromuscul Disord. 1999 Jun; 9(4): 232 -8
Neurology Update l Diseases l l l l Parkinsons disease Multiple Sclerosis Epilepsy Stroke Dementia Headache ……. . Germline mosaicism of MPZ gene in Dejerine-Sottas syndrome (HMSN III) associated with hereditary stomatocytosis Neuromuscul Disord. 1999 Jun; 9(4): 232 -8 l Neurology Top 10 Tips l Services l l TWRs Direct access investigations Local provision How to get the most out of your neurologist
Update - Parkinsons disease l l l Suspected PD Unsuspected PD – making the penny drop PD review Common Increasing prevalence l l Predicted to treble over the next 50 years Age 50 – 10: 100, 000 Age 80 – 200: 100, 000 < 80% confirmed at post-mortem !?
Classification of Movement Disorders l Akinetic l l Idiopathic Parkinsons Disease Parkinsons plus l l l MSA PSP DLB CBD Secondary Parkinsonism l Hyperkinetic l l l Chorea Ballism Tremors Myoclonus Wilsons disease Dystonia Tics + Tourettes Sleep related movement disorders Ataxia Dyskinesias Psychogenic
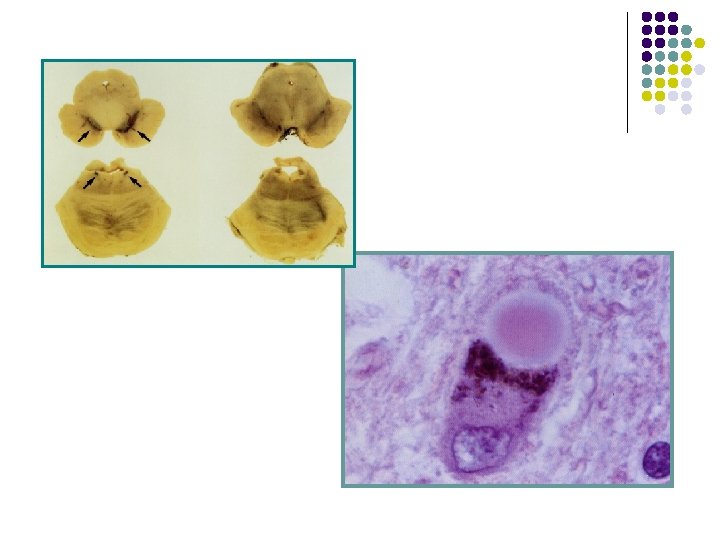
Definition of idiopathic PD l Pathological diagnosis l depigmentation + neuronal loss in substantia nigra l Intraneuronal inclusions- Lewy bodies
Clinical Features l Tremor l l UL>LL Asymmetric Rest tremor Tongue lips chin l Non-motor manifestations l l l Rigidity l l l Akinesia l Postural instability l l Gait micrographia Facial Hypomimia Speech l l Constipation EDS Anosmia REM behaviour disorder Depression Dementia Pain Postural stability Skin Autonomic ….
Sleep l l l l 75 -90% PD sleep dysfunction Insomnia Sleep fragmentation Sleep akinesia Nocturnal panic attacks RLS Excesssive daytime somnolence Neuropsychiatric problems l l Drug induced psychosis 10 -30% reduce parkinson meds monitor response neuroleptic trial quetiapine / clozapine / olanzapine Depression and Dementia l l Mirtazapine RIvastigmine
A Clinical Diagnosis Investigations: Exclude Wilsons -young with tremor MRI Da. T scan Research SPECT PET
PD - Is it something else ? l Essential Tremor l l l Kinetic +/- postural tremor 4 -12 Hz UL, head, voice, LL, trunk, tongue >90% undiagnosed 73% report significant disability Treatment: medical, botox, surgical l Drug induced Parkinsonism l 12% of 328 patients referred to secondary care l l l Parkinsons plus l l MSA PSP LBD CBD l l l Prochloperazine 32% Typical antipsychotics 42% atypical antipsychotics 18% Metoclopramide 11% Amiodarone 8% Lithium 8% Antihistamines 8% § l Promethazine and cinnarazine Valproate 5%
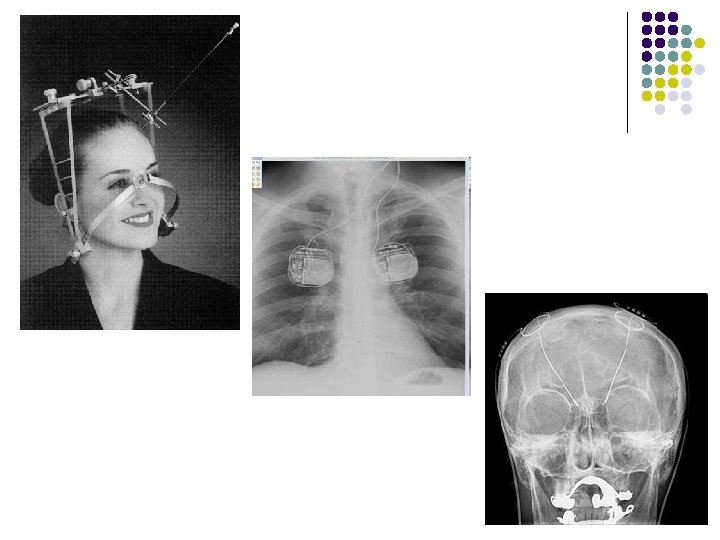
PD Treatment – what when and how? 1817 James Parkinson Blood letting Iatrogenic pus formation 2011 Dopaminergic Non dopaminergic Symptomatic Neuroprotective Surgery – Ablation – DBS – Brain Grafting Preventative
Levo Dopa l l Pros: effective Cons: side effects l l l Early side effects – N+V, HR, BP Late SE motor fluctuations dyskinesias neuropsychiatric (DATATOP trial n=352; F/U 20 months +/- 9) l Wearing off 50% Dyskinesias 33% Severe on-off 10% l Hedonistic homeostatic dysregulation l l Symptoms unresponsive to L-Dopa l l l l l postural instability freezing phenomena speech sialorrhoea depression and dementia ANS - sweating, urinary frequency, constipation sensory symptoms + pain Tremor REM sleep behaviour disorder
Levodopa therapeutic manoeuvres l On with dyskinesia vs Off without dyskinesia l l l CR preparations Hyperfractionate dosing schedule COMT inhibitors - entacapone, tolcapone l Stalevo § l l l Levodopa carbidopa entacapone § 50 / 12. 5 / 200 § Stalevo “ 50” “ 75” “ 100” “ 125” “ 150” “ 200” MAO inhibitors - selegeline, rasagiline Amantadine Dopamine Agonists Duo-dopa Apomorphine pump
Agonists l l l No dyskinesia potentially neuroprotective delays use of levodopa longer half life no absorption delay/dietary effects no metabolic conversion l Apomorphine Pergolide Cabergoline Pramipexole Ropinirole Rotigitone l Side effects l l l l Ankle oedema Gambling Sexual appetite
PD – whats new l Genetics l Drugs l NSAIDs l l l Ibuprofen protective but not other NSIADs N=136, 474 Stem cells
PD – whats new - Genetics l l 15% PD patients have an affected 1 st degree relative 5% due to mutation in one of several specific genes l l l l l In most cases, people with these mutations will develop PD. All rare except LRRK 2 l l Complex late onset sporadic degenerative 15 confirmed genes Mutations in genes including SNCA, LRRK 2 and glucocerebrosidase (GBA) have been found to be risk factors for sporadic PD. l l 10% familial PD 3% sporadic PD Genome wide association studies l l alpha-synuclein (SNCA) ubiquitin carboxy-terminal hydrolase L 1 (UCH-L 1) parkin (PRKN) leucine-rich repeat kinase 2 (LRRK 2 or dardarin) PTEN-induced putative kinase 1 (PINK 1) DJ-1 ATP 13 A 2 Mutations in GBA are known to cause Gaucher's disease All identified risks account for 2. 5 -3 x risk
Update – Multiple Sclerosis
Update – Multiple Sclerosis l Disease modifying therapies l CCSVI l Lifestyle effects l Sativex l NMO antibodies
Update – Multiple Sclerosis l Refresher l l Demyelination Inflammation Clinically isolated syndrome l Optic neuritis l Transverse myelitis l Brain stem l motor l Sensory Mc. Donald criteria 2001 2005 2010
Mc. Donald criteria Clinical presentation l Two or more attacks objective clinical evidence of two or more lesions l l Two or more attacks objective clinical evidence of one lesion One attack objective clinical evidence of two or more lesions One attack objective clinical evidence of one lesion (known as 'clinically isolated syndrome') Insidious neurological progression suggestive of multiple sclerosis (typical for primary progressive MS) Additional data needed for MS diagnosis None Dissemination in space shown on MRI or Up to two MRI detected lesions typical of MS plus positive CSF* or Await a further relapse suggestive of dissemination in space (ie affecting another part of the body) Dissemination in time demonstrated by MRI or Second clinical attack (relapse) Dissemination in space demonstrated by MRI or Up to two MRI detected lesions typical of MS plus positive CSF AND dissemination in time demonstrated by MRI or Dissemination in time demonstrated by MRI (ie new lesion seen on MRI at least 3 months after the original scan) or Second clinical attack (relapse) Positive cerebrospinal fluid* AND dissemination in space, shown on MRI or Abnormal visual evoked potential plus abnormal MRI AND dissemination in time demonstrated by MRI or Continued progression for one year (determined retrospectively or by ongoing observation)
Update – Multiple Sclerosis l Treatment of MS l Relapses l Treatment § l Prevention § l DMTs Treatment of symptoms l l l Oral methyprednisilone 500 mg od - 5 days Fatigue l Amantadine l Modafinil Depression Spasticity l Baclofen l Tizanidine l Sativex Bladder Etc…. Multi-disciplinary care
Update – Multiple Sclerosis - DMTs l a group of compounds which alter the progression of MS reduce the frequency and severity of relapses and slow the development of disability in some people. l Beta interferon l 1 a 1 b AVONEX REBIF BETAFERON im sc sc po COPAXONE sc Fingolimod l Glatiramer acetate l l Natalizumab TYSABRI l l Different mechanism, similar effect A recombinant humanised monoclonal antibody produced in murine myeloma cells. The specific mechanism(s) not fully defined. However, inhibition of leucocyte transmigration out of the vascular space. Progressive Multifocal Leukoencephalopathy*(PML) is an opportunistic infection caused by the JC virus that typically occurs in patients that are immunocomprimised. Mitoxantrone l Cardiac toxicity
Update – Multiple Sclerosis - DMTs l CCSVI l Zamboni l Stem cells l Lifestyle effects l Vitamin D l tobacco l diet l NMO antibodies l Neuromyelitis optica (Devic’s disease) l Aquaporin antibodies
Update – Multiple Sclerosis - DMTs l CCSVI l Zamboni Other neurological antibodies • MUSK l Stem cells l Lifestyle effects l Vitamin D l tobacco l diet l NMO antibodies l Neuromyelitis optica (Devic’s disease) l Aquaporin antibodies • VGKC • NMDA
Update – Epilepsy l More New AEDs l Enhance slow activation of Na channels l l l Ca channel lockers + carbonic anhydrase inhibitor l l Lacosamide Rufinamide Zonisamide Sudden unexplained death in epilepsy l Epilepsy SMR 1. 6 -9. 3 l l Underlying disorder / status / accidents / suicide / Rx related death / SUDEP 8 -17% of deaths l Memory l Psychosocial
Update – Stroke l Risk of stroke after TIA l Thrombolysis l PFO
Update – ……
Overview 1. Neurology - there’s a lot of it about
Overview 1. 2. Neurology - there’s a lot of it about Guidelines, QOFs, and more guidelines
Overview 1. 2. 3. Neurology - there’s a lot of it about Guidelines, QOFs, and more guidelines Do you suffer from Neurophobia ?
Overview • There’s a lot of it about • Guidelines, QOFs, and more guidelines • Neurophobia widespread
1. Neurological disorders are common l WHO “Neurological disorders – a public health challenge” “one of the greatest threats to public health” l Mortality vs DALYs l Neurological disease accounts for 20% of admissions to general hospitals l More diagnoses than the rest of medicine put together
2. l l l l Guidelines, QOFs, etc…. . NICE – PD NICE – epilepsy SIGN – epilepsy QOF – epilepsy Stroke and TIA Headache MS And all the others….
3. l Do you suffer from Neurophobia ? A fear of neurosciences and clinical neurology l Jozefowicz 1994 l Schon Hart et al 2002
3. Do you suffer from Neurophobia ? l A fear of neurosciences and clinical neurology l Jozefowicz 1994 l Schon Hart et al 2002 l Seeds Sown at medical school ?
4. l We can cure it for you ! The Epsom and St Helier neurology Service l ~100% patients seen by Consultant grade l 4 Consultant Neurologists l 2 Consultant Neurophysiologists l 4 specialist nurses l Neuro PT, OT etc… l State of the art imaging facilities, EEG, EMG, PIU l 52 clinics per month l 94% of ward referrals seen on day of referral, 99% within 48 hrs
Neurology – top ten tips l l l l l TIAs never cause isolated loss of consciousness Numb tingling hands are rarely due to neck pathology Beware of medication overuse headache Essential hypertension, sinusitis and “eye strain do not cause chronic daily headache Vertigo usually originates from the vestibular apparatus not the brain Diplopia – monocular = ophthalmology, binocular = neurology Know which headaches are worth worrying about Beware of misdiagnosing tremor Radiological imaging is rarely helpful in illuminating headache or back pain The neurological examination is hugely overvalued in non-neurologists
l Our ethos ? l Referral guidelines ? l Communication l l Tel 0208 296 3355 Fax 0208 296 3356
Neurology Update Paul Hart Neurologist l. Epsom l. AMNU + St Helier @ St George’s l. Royal Marsden Hospital t 0208 296 3355 f 0208 296 3356