Neuroendocrine Tumour of Small Bowel KaiHong Yue Ivan

Neuroendocrine Tumour of Small Bowel Kai-Hong Yue, Ivan Kwong Wah Hospital

Outline Neuroendocrine tumour Distribution and Classification Morphology Presentation and Diagnosis Treatment and survival Take home message

Neuroendocrine Tumour Oberndorfer, 1907: used Karzinoide to represent the carcinoma-like appearance and the relative indolent nature Neuroendocrine cells throughout the entire GI tract, bronchopulmonary systems, and urogenital tract Secrets vasoactive substances Controversies about terminology and staging WHO 2010 classification 1. Lubarsch O. Uber den pimaeren krebs des ileum nebst Bemerkungen ueber das gleichzeitige Vorkommen von krebs und Tuberculos. Virchows Arch 1888; 11: 280– 317. 2. Oberndorfer S. Karzinoide tumoren des dunndarms. Frankf Z Pathol 1907; 1: 425– 429.
 Extragastrointestinal (Lung, ovary, uterus) ~30 Oesophagus <1 Stomach 4 -8")
Distribution Site Occurrence (%) Extragastrointestinal (Lung, ovary, uterus) ~30 Oesophagus <1 Stomach 4 -8 Duodenum/ pancreas < 2 Small intestine 25 -30 Appendix 6 Colon 10 Rectum 15 Kenneth J. . Current management of gastrointestinal carcinoid tumors. Journal of Gastroint Surgery. 2004, Volume 8, Issue 6, pp 742 -756

WHO 1980 WHO 2000 WHO 2010 Carcinoid Highly differentiated neuroendocrine tumor Neuroendocrine tumor Grade 1 (carcinoid) Highly differentiated neuroendocrine carcinoma Mucocarcinoid mixed carcinoidadenocarcinoma Grade 2 Poorly differentiated (small-cell) neuroendocrine carcinoma Neuroendocrine carcinoma Grade 3 (Small- or large-cell) Mixed endocrineexocrine carcinoma Mixed adenoneuroendocrine carcinoma Bosman FT, et al. WHO Classification of Tumours of the Digestive System. Lyon, France: IARC Press; 2010.

Small Bowel Neuroendocrine Tumours Midgut/ Jejuno-ileal NETs “classical” midgut carcinoids serotonin (5 -hydroxytryptamine [5 -HT]) immunoreactivity 30% of NETs 25% of small-bowel neoplasms Average of diagnosis: 65 year-old Slight male predominance Modlin, I. M. , Kidd, M. , Latich, I. , et al. Current status of gastrointestinal carcino Gastroenterology 2005; 128: 1717 -1751.
, flat and fibrotic submucosal")
Morphological Features Most common: terminal ileum Small (usually <1 cm), flat and fibrotic submucosal tumour, central navelling Mesenteric metastases Typically conspicuously larger than primary tumour Incidence: 70 -90% in patient subjected to surgery Marked desmoplastic reaction with fibrosis Conglomerate of mesenteric lymph gland metastases Surgical treatment of midgut carcinoid tumours. World J Surg 1990; 14: 377 -385

Evers BM, Townsend CM Jr, Thompson JC. Small intestine. In Schwartz SI, ed. Principles of Surgery. New York: Mc. Graw-Hill, 1999, pp 1217– 1263. http: //www. webpathology. com/image. asp? case=209&n=2

Mesenteric metastases Partial or complete small-intestinal obstruction by kinking and fibrotic entrapment Fibrosis may tether the mesenteric root to the retroperitoneum/ duodenum Mesenteric vessels encased or occluded Venous stasis/ congestion, or arterial deficiency Vascular elastosis: specific angiopathy marked thickening of mesenteric vessel walls due to elastic tissue proliferation in the adventitia Surgical treatment of midgut carcinoid tumours. World J Surg 1990; 14: 377 -385

Distant Metastases Most common: liver Bilateral, diffusely spread; 10% dominant lesion Carcinoid syndrome Skeleton (spine, orbital framing) Lungs, CNS, peripheral lymphnodes, ovaries, breast, skin Surgical treatment of midgut carcinoid tumours. World J Surg 1990; 14: 377 -385

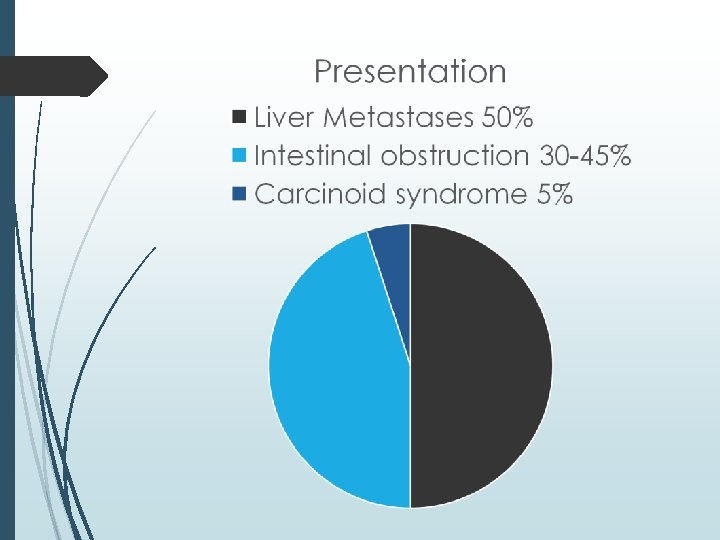
Clinical Presentation Slow growing tumour Long periods of prodromal symptoms Episodic abdominal pain; features of carcinoid syndrome Intestinal bleeding: rare, late Moderate size, submucosal location Mesenteric metastases invasion Venous stasis Modlin, I. M. , Kidd, M. , Latich, I. , et al. Current status of gastrointestinal carcino Gastroenterology 2005; 128: 1717 -1751.

Carcinoid Syndrome 20% of patient with jejuno-ileal NETs Release of vasoactive peptides: Serotonin, bradykinin, tachykinins (substance P, neuropeptide K), prostaglandins and growth factors, e. g. platelet-derived growth factor (PDGF), noradrenaline Implication: Hepatic metastasis Impaired monoamine oxidase activity for detoxification Symptoms: Secretory Diarrhoea, Cutaneous Flushing, Heart valve fibrosis, Bronchial constriction Modlin, I. M. , Kidd, M. , Latich, I. , et al. Current status of gastrointestinal carcino Gastroenterology 2005; 128: 1717 -1751.

Diagnosis Biochemistry Radiology Histology

Biochemistry Serotonin metabolite: (5 - Chromogranin A Sensitive, reflect tumour load, as indicator of treatment hydroxyindoleacetic response, non specific acid ) 5 -HIAA 24 -hour urine sample Plasma Specific Sensitive advanced disease, liver metastases Reflect tumour load, Indicator of treatment response, non specific

Radiology Contrast CT Sensitivity 50 -100% “circumscribed mesenteric mass with radiating densities” Somatostatin receptor scintigraphy - Octreo. Scan Sensitivity 43%– 86% indium-111. Somatostain receptors type 2 and 5 PET Sensitivity 90% - 97% fluorine 18 (18 F) FDG is less useful. Low proliferative rate Gallium; 68 Ga DOTA octreotate Midgut Neuroendocrine Tumors: Imaging Assessment for Surgical Resection Woodbridge et al. Radio. Graphics 2014 34: 2, 413 -426

Woolbridge et al. Midgut Neuroendocrine Tumors: Imaging Assessment for Surgical Resection. Radio. Graphics 2014 34: 2, 413 -426

Histology Insular, glandular, mixed growth pattern Immunocytochemistry staining Chromogranin A Synaptophysin Ki 67 antibody: proliferation rate grade 1 < 3%, grade 2 = 3– 20%, and grade 3 > 20%

Treatment Surgery Primary tumour and mesenteric metastases Resection Medical treatment and prophylaxis against carcinoid crisis

Primary tumour Surgical resection Active strategy with early prophylactic locoregional tumor removal to prevent or delay abdominal complications from the growth of the mesenteric tumor disease Resection of the primary tumor reduces symptoms and improves survival, even though inoperable mesenteric lymph node and liver metastases are present Inoperable Involvement of origins of proximal jejunal arteries, median colic artery or extending retroperitoneally

Hellman et al. Effect of Surgery on the Outcome of Midgut Carcinoid Disease with Lymph Node and Liver Metastases. World J. Surg. 26, 991– 997, 2002

Medical Treatment Palliation of symptoms Somatostatin analogues Octreotide, lanreotide Binding to somatostatin receptors types 2 and 5 Reduce the release of bioactive peptides Inhibit tumour growth, induce apoptosis Long-acting formulations (Monthly) Octreotide-LAR, lanreotide-PR Interferon-α (IFN - α) Reduces hormone secretion and stimulates natural killer cells

Prophylaxis Against Carcinoid Crisis Carcinoid crisis Hyperthermia, shock, arrhythmia, excessive flush or bronchial obstruction Octreotide 500 microgram in 500 ml NS, 50 microgram/hr infusion for prophylaxis 100 microgram/ hr infusion for carcinoid crisis ENETS Consensus guidelines for the standards of care in neuroendocrine tumors pre- and perioperative therapy in patients with neuroendocrine tumors. Neuroendocrinology 2009; 90: 203 -208.

Survival Age-adjusted overall 5 -year survival: 67% Median survival 8. 4 year Inoperable liver metastases: 50% 5 -year survival Inoperable liver and mesenteric lymph node metastases: 42% 5 -year survival Long-Term Results of Surgery for Small Intestinal Neuroendocrine Tumors at a Tertiary Referral Center. World J Surg (2012) 36: 1419– 1431

Take Home Message Rare, Slow growing tumour, long periods of prodromal symptoms Intestinal obstruction Carcinoid syndrome uncommon Locoregional resection improves survival even in presence of liver metastases Medical treatment improves symptoms
- Slides: 25