NEUROANATOMY REVIEW David Jho CEREBRAL CTX BRODMANNS AREAS

NEUROANATOMY REVIEW David Jho

CEREBRAL CTX

BRODMANN’S AREAS 6 4 3, 1, 2 5, 7 8 9 40 10 45, 4428 41, 42 34 11 12 22 39 19 18 17

BRODMANN’S AREAS 8 = Frontal Eye Field 6 = SMA & Premotor ctx 5, 7 = PPC (apraxia, dom. side) 4 3, 1, 2 6 4 = Primary motor ctx 3, 1, 2 = Primary somatosensory ctx 5, 7 9 41, 42 = Primary 8 auditory ctx (Transverse gyrus of Heschl) 40 45, 44 = Broca’s speech area (Inf Frontal Lobe; 10 39 expressive dysprosody) 22 45, 44 22 = Wernicke’s speech area (arcuate 41, 42 28 34 fasciculus connect to Broca’s; 11 receptive dysprosody) 12 40 = Supramarginal gyrus (Rt/Lt confusion, dyscalculia, understanding speech) 39 = Angular gyrus (dyslexia & dysgraphia) 19 18 17
 on dominant side a)")
BRODMANN’S AREAS 39, 40 = Inf parietal lobe (Gerstmann’s syndrome) on dominant side a) Rt/Lt confusion b) dyscalculia c) finger agnosia 6 4 3, 1, 2 d) dyslexia & dysgraphia 5, 7 8 9 e) lower quadrantanopia (visual radiations to cuneus) 40 Parietal lobe, non-dominant hemisphere (Sup or Inf parietal lobes) a) contralateral sensory neglect & astereognosis 39 10 b) construction apraxia 45, 44 41, 42 22 c) lower quadrantanopia (visual radiations to cuneus) 28 11 34 9, 10, 11, 12 = Prefrontal ctx 12 Post part of orbital gyrus = smell Uncus = serves as part of primary olfactory ctx (medial temporal lobe) 34 = Primary olfactory ctx (medial temporal lobe—seizures can have smell aura) 19 18 17

LIMBIC SYSTEM
 HIPP Fornix Mamillary body Septal area Hypothal VAFP/VAPP Stria terminalis")
PAPEZ CIRCUIT (Limbic System) HIPP Fornix Mamillary body Septal area Hypothal VAFP/VAPP Stria terminalis Ventral Amygdalo. Fugal Pathway Ventral Amygdalo. Petal Pathway Amygdala Mamillothalamic tract Olfactory, Sensory, Autonomic Ant nuc of thalamus Ant limb of internal capsule Cingulate gyrus Perforant pathway Cingulum Entorhinal ctx Wernicke’s Encephalopathy (Thiamine/Vit B 1 defic) 1) Nystagmus 2) Ataxia 3) Mental status change Korsakoff’s confabulatory syn 1) Mem loss & confabulation
 Orbitofrontal ctx (associated with HIPP)")
Mediodorsal nuc of the thalamus (associated with Ant nuc) Orbitofrontal ctx (associated with HIPP) Ansa lenticularis = VA Fugal Pathway
 a) Docility b) Hypersexuality")
Klüver-Bucy Syndrome (bilateral ablation of ant temporal lobes including amygdala) a) Docility b) Hypersexuality c) Hyperphagia d) Visual agnosia AMYGDALA—coordinates behavioral & emotional responses to complex sensory input by integrating somatosensory and viscerosensory information. Output via Stria Terminalis posteriorly by tail of caudate and arches over thalamus to anterior hypothalamus. Output via Ventral Amygdalofugal pathway (VAFP) to Caudate/Septal Area.
 Homeostasis (autonomic, endocrine, & limbic systems) b) Half of hypothalamus is enough")
HYPOTHALAMUS a) Homeostasis (autonomic, endocrine, & limbic systems) b) Half of hypothalamus is enough
 (sexually dimorphic, regulates gonadotropic hormones) Suprachiasmatic nuc (direct retinal")
Preoptic area (Medial Preoptic Nuc) (sexually dimorphic, regulates gonadotropic hormones) Suprachiasmatic nuc (direct retinal input, circadian rhythms) Lat Nuc (appetite center, stim induces eating, destruction causes starvation) Ventromedial Nuc (satiety center, stim stops eating, destruction causes obesity & savage behavior) Ant Hypothal Nuc (dissipates heat, parasympathetic) Post Hypothal Nuc (conserves heat, sympathetic) Parvocellular PVN & SON (produce oxytocin & ADH/vasopression, destruction causes DI) SUPRAOPTICODorsomedial Nuc HYPOPHYSIAL (stim causes obesity & savage TRACT behavior) Magnocellular PVN Arcuate Nuc (DOPA-ergic neurons inhib prolactin release) TUBEROINFUNDIBULAR TRACT

HYPOTHALAMIC FIBER SYSTEMS Fornix From HIPP to mamillary nuclei (then Mamillothalamic tract to Ant Thal Nuc) Medial Forebrain Bundle (MFB) a) in lat hypothalamus, lat to fornix; can be damaged in hypothal injury b) unmyelinated, major connection b/n cerebral ctx & BS c) no synaptic relay through thalamus d) has monoaminergic neurons from the locus coeruleus (NE), raphe nuclei (5 -HT), and ventral tegmental area (DA). Hypothalamo-spinal tract Descending autonomic fibers for sympathetic neurons (thoracic intermediolateral horn) and parasympathetic neurons (sacral lateral horn) Lesion or interruption above T 1 can cause Horner’s syndrome (miosis, ptosis, anhidrosis, & apparent enophthalmos)

HYPOTHALAMIC FIBER SYSTEMS Stria terminalis is the major pathway of Amygdala to hypothalamus & septal area. STRIA = STRANDS (Sup to fornix & divides caudate from thalamus) Lamina terminalis (from optic chiasm to rostral 3 rd ventricle; closure of ant neuropore) LAMINA = LAYER Stria medullaris thalami (hypothalamus & septal area in roof of 3 rd ventricle inf to fornix to thalamus & epithalamic habenular nuclei; relay from limbic forebrain to midbrain reticular formation) MEDULLARIS is also in the MEDULLA Stria medullaris of 4 th ventricle (central sulcus to Inf Cereb Ped; arcuate nuc of pyramids) Sulcus Limitans (divides Alar & Basal plates) SULCUS = GROOVE
")
HYPOTHALAMIC FIBER SYSTEMS (strands)
 Ant neuropore (anencephaly) vs Post neuropore (spina bifida)")
HYPOTHALAMIC FIBER SYSTEMS Lamina terminalis (layer) Ant neuropore (anencephaly) vs Post neuropore (spina bifida)
")
HYPOTHALAMIC FIBER SYSTEMS (medial & also in medulla)

HYPOTHALAMIC FIBER SYSTEMS
 Neural Crest (PNS including DRG, postgang ANS)")
EMBRYOLOGIC DEVELOPMENT Neural Tube (CNS, pregang ANS) Neural Crest (PNS including DRG, postgang ANS) Sulcus Limitans (divides Alar & Basal plates) Alar plate (sensory), Basal plate (motor) Rhombencephalic lip (in roof of 4 th ventricle becomes Cerebellum)
 Diencephalon (3")
EMBRYOLOGIC DEVELOPMENT PRIMARY VESICLES Prosencephalon Mesencephalon Rhombencephalon SECONDARY VESICLES Telencephalon (lateral ventricles) Diencephalon (3 rd ventricle) Mesencephalon (cerebral aqueduct) Metencephalon (upper 4 th ventricle) Myelencephalon (lower 4 th ventricle, central canal)
 2. PCOM (ant circulation) 3. Ant Choroidal")
THALAMUS BLOOD SUPPLY 1. PCA (post circulation) 2. PCOM (ant circulation) 3. Ant Choroidal a (ICA)
 = ANT-LAT (EPS) = POST (sensory) = NON-SPECIFIC (relay)")
= ANT-MED (limbic) = ANT-LAT (EPS) = POST (sensory) = NON-SPECIFIC (relay)
 Ant+MD (Papez) VPL (sensory--body) VPM (sensory--head) LGN (vision) MGN (hearing) Pulvinar (visual")
VA/VL (GP+SN) Ant+MD (Papez) VPL (sensory--body) VPM (sensory--head) LGN (vision) MGN (hearing) Pulvinar (visual sensory association) = ANT-MED (limbic) = ANT-LAT (EPS) = POST (sensory) Intralaminar CM (very diffuse to cerebral ctx, ends in layer I for cortical excitability) Reticular (GABA-ergic to thal) = NON-SPECIFIC (relay)

Mamillary bodies Cingulate gyrus Prefrontal ctx
 Area 6 Area 4 GP, SN, cerebellum (EPS + dentatothalamic tract)")
GP, SN (EPS) Area 6 Area 4 GP, SN, cerebellum (EPS + dentatothalamic tract) Area 4 + EPS

Integration of somesthetic, visual, & auditory Areas 18, 19 Areas 3, 1, 2 Areas 41, 42 Sensory--body Hearing Sensory--face Vision Area 17
 LD or DL LP Ant VA (VL) Ant Interthalamic adhesion")
Caudate Fornix VA (VL) LD or DL LP Ant VA (VL) Ant Interthalamic adhesion Cerebral peduncle Mamillary bodies Ant VL CM MD Ant MD CM VL Pulvinar Pineal gland MD Pulvinar Sup colliculus VPL VPM LGN VPL MGN Midbrain Zona Incerta STN Pons MGN LGN
 a) Dentate gyrus—HIPP input & output")
HIPPOCAMPUS HIPPOCAMPAL FORMATION (3 -layered archicortex; declarative mem) a) Dentate gyrus—HIPP input & output to HIPP pyramidal cells b) Hippocampus proper or Cornu Ammonis (CA)—to fornix then septal area c) Subiculum—to fornix then mamillary nuc Alzheimer’s Disease affects neurons in Nuc Basalis of Meynert (ACh), Locus Coeruleus (NE), Entrorhinal ctx, and CA 1/Subiculum of HIPP.
 Fimbria of Fornix Alveus 6 -layer")
HIPPOCAMPUS Mammillary bodies Postcommissural Fornix (connects bilateral CA) Fimbria of Fornix Alveus 6 -layer 3 -layer vs NEOCORTEX ARCHICORTEX Schaeff e CA 3 Entorhinal ctx (with pyriform ctx are paleoctx) th for r e P Alvear path rals CA 1 CA 4 DENTATE GYRUS r collate pa t n a SUBICULUM

Dentate gyrus has afferents entirely within HIPP formation. CA 1 projects to Subiculum and precommissural fornix. CA 3 projects to CA 1 and precommissural fornix. CA 4 (hilus of dentate gyrus) receive afferents from dentate and project to bilateral dentate (hippocampal commissure). Subiculum provides main efferents to POST-COMMISSURAL FORNIX (to thalamus and hypothalamus).

EPS SYSTEM
 UMN lesion 1. 2. 3. 4. 5. Weakness Spasticity Inc")
Pyr system (CS tract) UMN lesion 1. 2. 3. 4. 5. Weakness Spasticity Inc tone No atrophy Babinski LMN lesion 1. 2. 3. 4. 5. EPS (Basal Ganglia) 1. Chorea (Huntington’s, Syndenham’s) Weakness Dec DTR Dec tone Atrophy Downgoing toes Cerebellum 1. Intention tremor 2. Ataxia (fall towards lesion, 2. Athetosis (choreoathetosis in HD, gait & trunk dystaxia, Tardive dyskinesia when dysrhythmokinesia, antipsychotics block DA receptors & dysdiadochokinesia, make super-sensitive) dysmetria) 3. Hemiballismus (stroke) 3. Nystagmus 4. Parkinson’s vs Diffuse Lewy Body Dz 4. Dec DTR/tone ipsilaterally (resting tremor, bradykinesia, truncal instability, dementia)

Glutamate Lenticular nuc = Put + GP Striatum/Neostriatum = Put + Caud Corpus striatum = Put + Caud + GP GABA (Glycine in SC) Input from Ctx--Net excitation Input from D 1 recep—Net excitation DIRECT PATHWAY Ctx Striatum Parkinson’s GPi/SNr VA/VL thalamus Ctx D 1 recep SNc INDIRECT PATHWAY Ctx Striatum Parkinson’s D 2 recep SNc GPe STN Input from Ctx—Net inhibition Input from D 2 recep—Net excitation GPi/SNr VA/VL thalamus Ctx
 have both D 1 recep (Gs; contain excitatory Substance P) and")
Striatum (GABAergic neurons) have both D 1 recep (Gs; contain excitatory Substance P) and D 2 recep (Gi; contain inhibitory Enkephalin). Net LOSS of excitation in Parkinson’s Dz. Pallidotomy destroys segments of GPi to reduce inhibition of thalamus (interrupts direct & indirect pathways). GPi and GPe are usually always on. Input from Ctx--Net excitation Input from D 1 recep—Net excitation DIRECT PATHWAY Ctx Striatum Parkinson’s GPi/SNr VA/VL thalamus Ctx D 1 recep SNc INDIRECT PATHWAY Ctx Striatum Parkinson’s D 2 recep SNc GPe STN Input from Ctx—Net inhibition Input from D 2 recep—net excitation GPi/SNr VA/VL thalamus Ctx

GPe is constantly on. In Huntington’s chorea, the striatum (ACh & GABAergic medium spiny neurons) are destroyed so GPe overstimulates Ctx. Damage to STN results in Hemiballismus due to decreased stim of thalamic inhibition to Ctx. Input from Ctx--Net excitation Input from D 1 recep—Net excitation DIRECT PATHWAY Ctx Striatum Parkinson’s GPi/SNr VA/VL thalamus Ctx D 1 recep SNc INDIRECT PATHWAY Ctx Striatum Parkinson’s D 2 recep SNc GPe STN Input from Ctx—Net inhibition Input from D 2 recep—net excitation GPi/SNr VA/VL thalamus Ctx

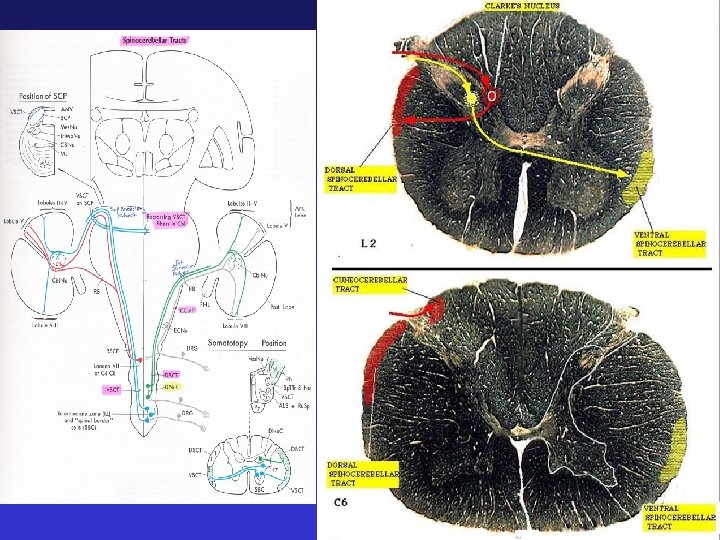
CEREBELLUM Functional vs Anatomical Divisions

Cerebellar Synonyms 1. FLOCCULONODULAR LOBE = Vestibulocerebellum. 2. VERMIS = Medial zone or part of Spinocerebellum. 3. PARAVERMIS = Intermediate zone or part of Spinocerebellum. 4. CEREBELLAR HEMISPHERES = Lateral zone or Cerebrocerebellum or Pontocerebellum.

Cerebellar Function 1. FLOCCULONODULAR LOBE = balance & eye movement. 2. VERMIS = balance & axial motor functions. 3. PARAVERMIS = distal motor execution. 4. CEREBELLAR HEMISPHERES = motor planning.
 2. Middle Cerebellar Ped (pontocerebellar")
Cerebellar Peduncles 1. Sup Cerebellar Ped (dentatothalamic tract, VSCT) 2. Middle Cerebellar Ped (pontocerebellar fibers) 3. Inf Cerebellar Ped (Olivo. CT, Dorsal Spino. CT, CCT, vestibulocerebellar tract) - Spine to cerebellum
 MOLECULAR Stellate LAYER Purkinje PARALLEL FIBERS GOLGI LAYER")
Motor Ctx (corticopontine & CS tracts) MOLECULAR Stellate LAYER Purkinje PARALLEL FIBERS GOLGI LAYER CLIMBING FIBERS PURKINJE LAYER Basket Corticopontine fibers Pontine nuc Dentatothalamic tract (Sup Cereb Ped) Pontocerebellar tract (contralat) MOSSY FIBERS Golgi VL (thalamus) Red Nuclei (rubrospinal tract) Cereb Deep Nuc Dentate Emboliform Fastigial Globose Spinocerebellar Pontocerebellar Vestibulocerebellar (cerebellar & vestibular nuc) Granule ION Olivocerebellar tract to CLIMBING FIBERS Vestibulospinal tract

4 Cerebellar Deep Nuclei 5 Types of. Cerebellar Cells (know if excit or inhib; know if projects out of cerebellum or not)

Cerebellar Deep Nuclei receive excitatory afferents from Climbing fibers and Mossy fibers (collaterals on their way to the Granule layer). Purkinje cell (only ones that project out of ctx) inhibitory fibers from Cerebellar Ctx to Cerebellar Deep Nuclei. Climbing fibers from Inf Olivary Nuc via Inf Cerebellar Ped. Pontocerebellar fibers via Middle Cerebellar Ped. Granule cell (only excitatory) endings (Parallel Fibers) go to Molecular layer but not out of Cerebellar Ctx. Stellate, Basket, & Golgi cells (inhibitory) do not project out of Cerebellar Ctx either.

Flocculo-nodular lobe projects to Medial and Lateral Vestibular Nuclei. Medial Vestibular Nuclei assist coordinating eye movement with body. Lateral Vestibular Nuclei assist postural control. Be careful not to confuse Dentate nuclei (cerebellum) and Dentate gyri (HIPP).
 & crosses immed in midbrain. Rt cerebellum")
Rubrospinal tracts (gross mvmts unlike CS tracts) & crosses immed in midbrain. Rt cerebellum to Lt Red Nucleus to Rubrospinal tracts crossing left-to-right to innervate Rt arm & leg. Cerebellar tests = finger-to-nose (dysmetria & intention tremor), foot tap/heel shin, pronator drift with poor adjustment, dysdiadochokinesia, nystagmus on extreme gaze. Romberg test = vision, vestibular, DC-ML. (not SC tract, which is unconsc proprio).

BV’s & CN’s
 asymptomatic unless large or rupture (possible death) rupture—SAH,")
Berry aneurysms (ACOM, MCA, PCOM, basilar) asymptomatic unless large or rupture (possible death) rupture—SAH, hemorr stroke (seizures, HCP) worst HA of life (10/10) ADPKD, Ehlers-Danlos, Marfan’s Pituitary adenoma Acoustic neuroma (Schwannoma) at CPA Uncus = where Amygdala is located

ICA-MCA aneurysm can put pressure on side of optic chiasm. Basilar tip aneurysm can put pressure on CN 3’s. Lat striate or Lenticulostriate aa of cerebral hemorrhage (internal capsule). Occlusion of PCA distal to PCOM can result in Ant choroidal to Post choroidal aa. Labyrinthine a from AICA or Basilar a. Post Spinal a from PICA or Vertebral a.
. Pupillary light")
Autoregulation allows constant blood flow over wide bp range (local metabolite control). Pupillary light reflex is CN 2 afferent and CN 3 efferent. CN 2 lesion preserves a consensual reflex. CN 3 lesion causes blown-pupil, down-and-out eye, droopy eyelid, & efferent loss. Corneal blink reflex is CN 5 (V 1) afferent and CN 7 efferent. Ankle jerk Knee ext Brachiorad Biceps Triceps = = = Abdominal = Babinski = S 1 L 2, 3, 4 C 5 C 6 C 7 T 8 -T 12 L 5 -S 1
 + MCA (lateral")
Internal Capsule BLOOD SUPPLY ANT LIMB = ACA (medial striate aa) + MCA (lateral striate aa) GENU = ICA (Ant Choroidal a) POST LIMB = ICA (Ant Choroidal a) + MCA (lateral striate aa)
 block cerebral aqueduct")
Scalp infections down through valveless emissary vv. Pineal tumors (Perinaud’s syn) block cerebral aqueduct and/or impose on sup colliculus Epidural lens, Subdural falx, Subarachnoid (ventricles), Intraparenchymal bleeds
 HCP ex-vacuo (big ventricles, no inc ICP) Pseudotumor cerebri")
Communicating vs Non-communicating Hydrocephalus (HCP) HCP ex-vacuo (big ventricles, no inc ICP) Pseudotumor cerebri (nml or slit ventricles, inc ICP) Above or below 4 th ventricle Choroid plexus Creates CSF, Arachnoid villi/granulations Absorb CSF

HERNIATION SYNDROMES Subfalcine Transtentorial Foraminal

VISUAL SYSTEM

TEMPORAL NASAL TEMPORAL Ipsilateral blindness Nasal hemianopia Contralateral hemianopia with macular sparing Bitemporal hemianopia Contralateral hemianopia to LGN, optic radiations, then occipital lobe

LGN Crossed fibers to layers 1, 4, 6 Uncrossed fibers to layers 2, 3, 5 to LGN, optic radiations, then occipital lobe

LGN Crossed fibers to layers 1, 4, 6 Uncrossed fibers to layers 2, 3, 5 to LGN, optic radiations, then occipital lobe

LGN to OCCIPITAL LOBE Parietal lobe visual radiations to cuneate gyrus Contralateral lower quadrantanopia Calcarine fissure Temporal lobe visual radiations (Meyer’s loop) to lingual gyrus Contralateral upper quadrantanopia to LGN, optic radiations, then occipital lobe
 Central scotoma (optic neuritis in MS) Lower altitudinal hemianopia (bilateral cuneate")
Constricted field (glaucoma) Central scotoma (optic neuritis in MS) Lower altitudinal hemianopia (bilateral cuneate gyri) Upper altitudinal hemianopia (bilateral lingual gyri) to LGN, optic radiations, then occipital lobe

Sup Colliculus Vertical gaze MLF Coordinates CN 3 & CN 6 (internuclear ophthalmoplegia in MS) a) carries info from pontine Horizontal Gaze Centers to oculomotor complex in midbrain. b) Inc activity during mvmt c) Helps during turning of head (conjugate gaze)

Left? Right? to LGN, optic radiations, then occipital lobe

Right? Left? True Diplopia CN 3 = accommodation, many mvmts CN 4 = down-and-out CN 6 = lateral to LGN, optic radiations, then occipital lobe
 Rt Pontine Paramedian Reticular Formation (PPRF; lat")
Voluntary Conjugate Gaze Lt Area 8 (FEF) Rt Pontine Paramedian Reticular Formation (PPRF; lat gaze center) Rt CN 6 Lt Medial Longitudinal Fasciculus (MLF) Lt CN 3 [Rt Gaze] Internuclear Ophthalmoplegia Pupillary Light Reflex Optic Sup Colliculi Ciliary LGB n/chiasm/ (pretectal ganglia tract area) (CN 3) (CN 2) Argyll-Robertson’s pupils (syphilis) Accommodation Optic n/chiasm/ tract (CN 2) LGB Optic radiation Visual ctx Sup Colliculi (pretectal area) Ciliary ganglia (CN 3)
 Rt Pontine Paramedian Reticular Formation (PPRF; lat")
Voluntary Conjugate Gaze Lt Area 8 (FEF) Rt Pontine Paramedian Reticular Formation (PPRF; lat gaze center) Rt CN 6 Lt Medial Longitudinal Fasciculus (MLF) Lt CN 3 [Rt Gaze] One-and-a-half Syndrome Pupillary Light Reflex Optic Sup Colliculi Ciliary LGB n/chiasm/ (pretectal ganglia tract area) (CN 3) (CN 2) Argyll-Robertson’s pupils (syphilis) Accommodation Optic n/chiasm/ tract (CN 2) LGB Optic radiation Visual ctx Sup Colliculi (pretectal area) Ciliary ganglia (CN 3)
 is 1 st place with binaural processing. 2.")
HEARING 1. Medial Superior Olive (SON) is 1 st place with binaural processing. 2. Lesion above cochlear nuclei (Lateral leminscus and up) will decrease hearing bilateral (more in contralateral ear). 3. Inner hair cells transduce sound, and Outer hair cells modify sound (olivocochlear efferents). Scala media (endolymph). 4. Lateral Superior Olive (SON) has intensity differences for horizontal position orientation. 5. High freq is closest to Oval window/Stapes (scala vestibule and NOT round window at the end of the scala tympani) for tonotopic organization, and high freq is dorsomedial in cochlear nuclei.

HEALING 1. ANTEROGRADE degeneration is Wallerian degeneration—axons & myelin sheaths disappear. (e. g. , Mid-thoracic crush of spine and Pt dies. Cervical stain shows Wallerian degeneration of fasciculus gracilis. ) 2. RETROGRADE degeneration is Chromatolysis—loss of Nissl substance (RER & free polyribosomes at cell body and dendrites are lost) 3. In the CNS, glial scars formed by astrocytes inhibit healing (reactive astrogliosis). 4. For successful axonal repair, macrophages must clean debris. 5. Axonal elongation is 2 -4 mm/d in the CNS (oligodendrocytes) or PNS (Schwann cells).
 tropic (differentiation; turning toward")
HEALING 1. Target-derived neurotrophic factor = Nerve Growth Factor (NGF) tropic (differentiation; turning toward stim) & trophic (growth & survival) peptide for DRG and sympa in PNS and basal forebrain ACh neurons in CNS. 3. Neurotrophins (NGF, BDNF, NT 3) + IGF 1 + FGF + GDNF + CNTF 4. BDNF is synthesized in cell body & transported anterogradely down the axons (unlike NGF or GDNF).
 Special")
Neurohistology Sensory neurons = Pseudounipolar, myelinated (DRG and CN 5, 7, 9, 10) Special senses = Bipolar (smell is unmyelinated-slow, hearing is myelinated-fast) (CN 1, 2, 8) Motor neurons = Multipolar, myelinated (a. MN, ANS)
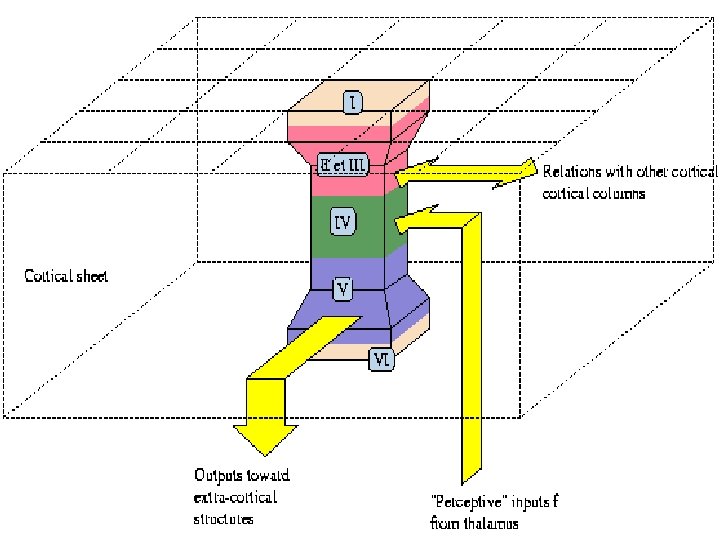
 Layer II (External Granular) Layer III (External Pyramidal)—cortico-cortical")
6 -Layered Neocortex Layer I (Molecular) Layer II (External Granular) Layer III (External Pyramidal)—cortico-cortical fibers Layer IV (Internal Granular)—thalamocortical fibers (VPL, VPM, LGN) Layer V (Internal Pyramidal)—CS, CB, & corticostriatal fibers (Betz giant pyramidal cells) Layer VI (Multiform)—corticothalamic projection & association fibers AFFERENT EFFERENT (Layer IV is big in Brodmann Area 3, 1, 2) (Layer V is big in Brodmann Area 4)

SENSORY & MOTOR HOMUNCULI Lots to lips, tongue, hand, & index finger Paracentral lobule = feet/legs

RABIES Rabies is caused by a Rhabdovirus that enters a peripheral nerve and travels retrograde up the nerve to the DRG. From there, it replicates and infects the CNS, resulting in encephalitis with a variety of neurologic symptoms leading to coma and respiratory or cardiac arrest.

THE END
- Slides: 72