Nephrotic Syndrome Dr Carol Inward Consultant Paediatric Nephrologist




























- Slides: 38
Nephrotic Syndrome Dr Carol Inward Consultant Paediatric Nephrologist NPPG Conference Bristol 2011
What Is Nephrotic Syndrome?
Causes • Primary • Secondary • Minimal Change Disease • Focal Segmental Glomerulosclerosis • Mesangioproliferative glomerulonephritis • Ig. A Nephropathy • • Henoch Schonlein Pupura SLE Hepatitis B&C HIV • Genetic • Mutations in genes coding for podocyte proteins
Epidemiology • Incidence 2 -7 per 100 000 population <16 yrs • Most commonly presents in pre-school children • MCNS 75% of cases overall & 93% who respond to steroids ( but only 20 -30% of adolescents) • >60% will have a relapsing course • 44% will be relapse free 1 year from diagnosis • 69% relapse free after 5 years • 84% relapse free after 10 years
Georgia 2001 1 st presentation with NS age 3 yrs Prednisolone 60 mg/m 2 for 4 weeks 40 mg/m 2 alt days for 4 weeks Relapses on withdrawal of steroid & then on low dose alternate day prednisolone Referred for specialist opinion
Georgia – 2 nd line • Cyclophoshamide 3 mg/kg over 8 weeks • Weekly monitoring of FBC • Continued relapses→ high dose oral prednisolone
Georgia – 3 rd line • Feb 2002 Cyclosporin → seizures • IV antibiotics, ganciclovir & phenobarbitone
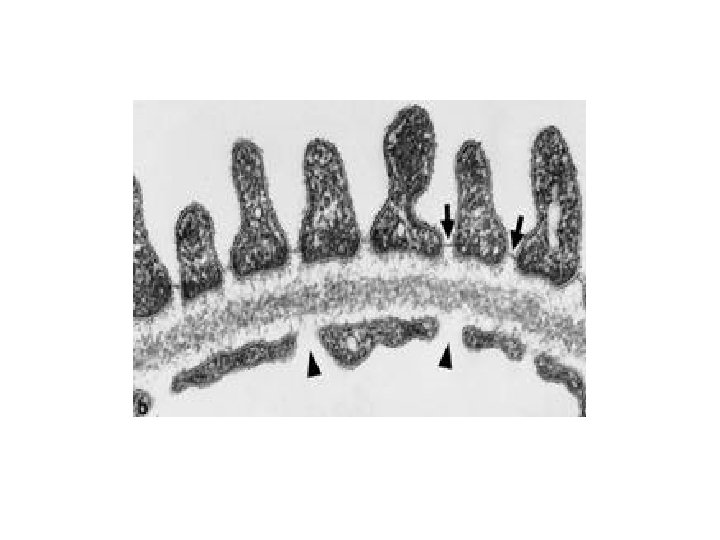
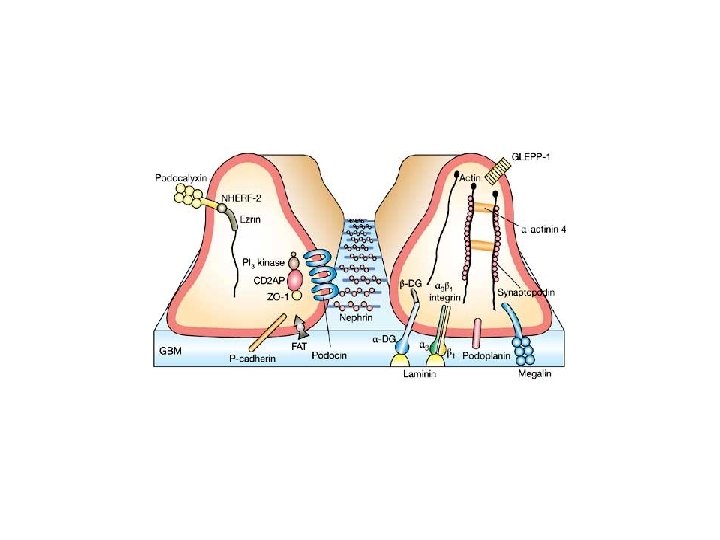
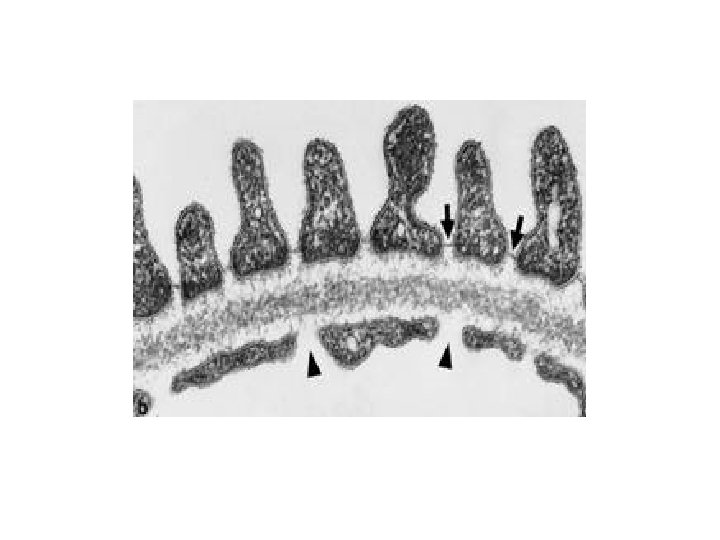
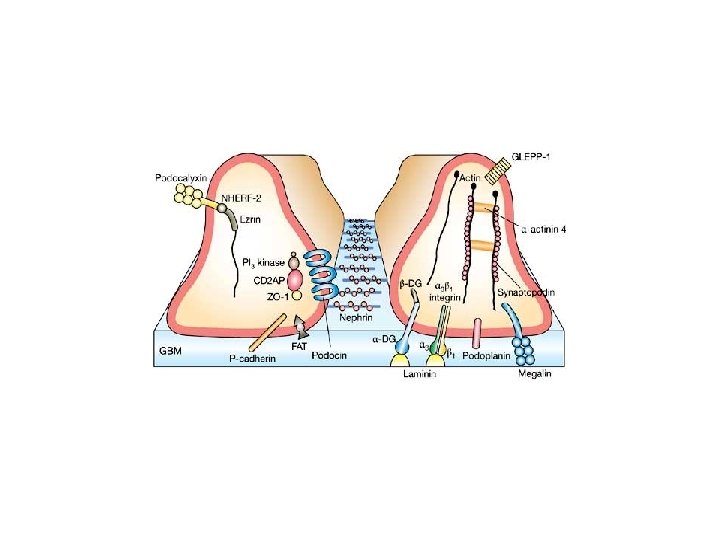
What are we treating? • Minimal Change Disease
Further Strategies • Low dose alternate day prednisolone and levamisole • Chlorambucil • Mycofenolate
Progress • Prolonged remission allowing withdrawal of prednisolone • Mycophenolate withdrawn in 2009 • Has had one relapse since then • Discharged from hospital follow up this year as relapse free off treatment for 12 months
What causes Minimal Change Nephrotic Syndrome? • • • Disorder of the immune system? Response to immunosuppressives Remission during infection with measles virus Response to plasma exchange Experimental induction of nephrotic syndrome in animals by infusion of plasma from patients in relapse.
Why use all these toxic medicines? • Uncontrolled oedema→ respiratory compromise, skin breakdown, cellulitis • Circulatory compromise → AKI • Prothrombotic state → risk of thromboembolism • Loss of immune mediators →sepsis • Untreated mortality 50% - treated 2 -5%
Summary • Minimal Change Nephrotic Syndrome • Good prognosis but potentially life threatening • Immunosuppressive strategies are effective but may lead to significant complications
Welcome to Bristol
Nephrotic Syndrome Dr Carol Inward Consultant Paediatric Nephrologist NPPG Conference Bristol 2011
What Is Nephrotic Syndrome?
Causes • Primary • Secondary • Minimal Change Disease • Focal Segmental Glomerulosclerosis • Mesangioproliferative glomerulonephritis • Ig. A Nephropathy • • Henoch Schonlein Pupura SLE Hepatitis B&C HIV • Genetic • Mutations in genes coding for podocyte proteins
Epidemiology • Incidence 2 -7 per 100 000 population <16 yrs • Most commonly presents in pre-school children • MCNS 75% of cases overall & 93% who respond to steroids ( but only 20 -30% of adolescents) • >60% will have a relapsing course • 44% will be relapse free 1 year from diagnosis • 69% relapse free after 5 years • 84% relapse free after 10 years
Georgia 2001 1 st presentation with NS age 3 yrs Prednisolone 60 mg/m 2 for 4 weeks 40 mg/m 2 alt days for 4 weeks Relapses on withdrawal of steroid & then on low dose alternate day prednisolone Referred for specialist opinion
Georgia – 2 nd line • Cyclophoshamide 3 mg/kg over 8 weeks • Weekly monitoring of FBC • Continued relapses→ high dose oral prednisolone
Georgia – 3 rd line • Feb 2002 Cyclosporin → seizures • IV antibiotics, ganciclovir & phenobarbitone
What are we treating? • Minimal Change Disease
Further Strategies • Low dose alternate day prednisolone and levamisole • Chlorambucil • Mycofenolate
Progress • Prolonged remission allowing withdrawal of prednisolone • Mycophenolate withdrawn in 2009 • Has had one relapse since then • Discharged from hospital follow up this year as relapse free off treatment for 12 months
What causes Minimal Change Nephrotic Syndrome? • • • Disorder of the immune system? Response to immunosuppressives Remission during infection with measles virus Response to plasma exchange Experimental induction of nephrotic syndrome in animals by infusion of plasma from patients in relapse.
Why use all these toxic medicines? • Uncontrolled oedema→ respiratory compromise, skin breakdown, cellulitis • Circulatory compromise → AKI • Prothrombotic state → risk of thromboembolism • Loss of immune mediators →sepsis • Untreated mortality 50% - treated 2 -5%
Summary • Minimal Change Nephrotic Syndrome • Good prognosis but potentially life threatening • Immunosuppressive strategies are effective but may lead to significant complications
Welcome to Bristol