Nephrology and Hypertension An Update in 2017 Johan







30057 -0)")
30057 -0)")



 91, 982 -988")












 Average e. GFR 20 - 29 116 ml/min/1. 73")

 of CV morbidity 40 30 p <")

















: 10 patients with resistant hypertension")



. Julian F. R. Paton et al.")

 is antihypertensive, lowers respiratory rate (transiently) and")
. Julian")
. Julian F.")

 • ACCORD did look specifically at diabetics t 2 •")


")
")
 • Lifestyle advice is recommended for all patients. GRADE: Strong; LEVEL: •")





 65 64%*")




 Majority of patients achieved BP")





")








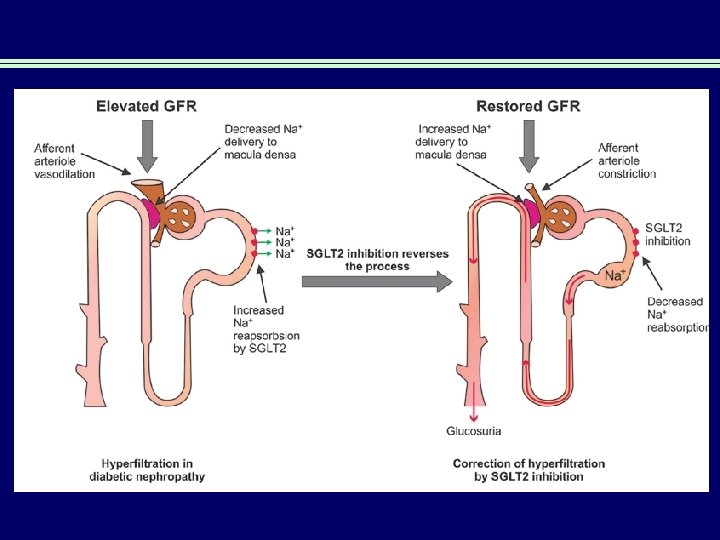
 inhibitors Induce prox tubular glycosuria Benefits: • reduce Hb.")
, Placebo & CKD: ↓wt, BP, GFR & u. ACR Wt")














 Please do not get obsessed with")
- Slides: 120
Nephrology and Hypertension: An Update in 2017 Johan Rosman, nephrologist FRACP Foundation Professor of Medicine Curtin University Medical School Royal Perth Hospital Private Practices in Nedlands and Cannington www. perthkidneys. com. au Healthlink EDI ptkidney
What is new in Nephrology and Hypertension • Nothing • Thank you for your attention • Are there any questions ? • This presentation will be uploaded to my website: – www. perthkidneys. com. au
Identity ? ? ? ?
Is prehydration useful for renal patients receiving Xray contrast ?
Lancet 2017; 389: 1312
AMACING study setup • Parallel group, open-label, no inferiority trial of patient at risk for CIN • High risk patients used: e. GFR 30 -59 ml/min, >18 years old, undergoing elective procedure requiring iodinated contrast • Randomly allocated, receiving pre-hydration with 0. 9% Na. Cl or not • Primary outcome: incidence of CIN, defined as increase in creatinine>25%, or 44 umol/L, within 2 -6 days of exposure, and cost -effectiveness of no prophylaxis vs pre-hydration to prevent CIN • Creatinines dones before, after 2 -6 days and after 26 -35 days • Between 2014 and 2016: 332 patients no prophylaxis, 328 with Na. Cl
Fluid protocol • 0. 9% Na. Cl 3 -4 ml/kg per hour during 4 and during 4 hours after contrast, but in cardiac compromised patients: ” 0. 9% Na. Cl 1 ml/kg per hour 12 hours before and 12 hours after • Control group patients free drinking as they felt • For medical reasons clinicians could deviate from this protocol
Figure 2 The Lancet 2017 389, 1312 -1322 DOI: (10. 1016/S 0140 -6736(17)30057 -0) Copyright © 2017 Elsevier L
Figure 3 The Lancet 2017 389, 1312 -1322 DOI: (10. 1016/S 0140 -6736(17)30057 -0) Copyright © 2017 Elsevier Ltd Terms and Conditions
Prophylaxis of contrast nephropathy • AMACING trial • No difference in rate of contrast nephropathy between group given 0. 9% saline or no i. v. fluids before contrast administration • Adverse effects: heart failure, hyponatremia, arrhythmia more common in the iv fluid group • Criticised: low power, low overall rate opf contrast nephropathy, suggesting patients were not at significant risk
Telehealth • In many disciplines already well established method of efficient communication with remote locations • In renal lagging behind as resistance in renal community • Most telehealth in renal is in private practice, like in my practice where I serve from Kununurra to Esperance and Augusta • Encrypted systems like Goto. Meeting very comfortable for patients and high quality multi-user platforms can easily include GP as the third person in the conference (MBS item) • Although major push is being made, renal medicine keeps resisting • The future will require Tele. Health to become a top player to save money and increase patient comfort
Is there proof that intensive follow up of diabetes patients make a difference for outcome ?
Kidney Int (2017) 91, 982 -988
Trial design • • Short term studies supported some benefit to renal outcome of intensive follow up, and early referral to nephrology Recent meta-analysis showed early vs late use of ACE/ARB had up to 4 years delay of ESRD (Schievink et al, Diebetes Obes Metab, 2016) Post hoc analysis of impact of intensified, multifactorial treatment on renal outcomes in patients with type 2 diabetes and microalbuminuria Patients were part of the large cohort of the STENO-2 study STENO study recently published sign reduction in cardiovascular disease and – mortality after 21 year follow up with intensive treatment 160 patients recruited with type 2 diabetes plus microalbuminuria and assigned to conventional or intensified treatment targeting multiple risk factors Mean duration of intervention 7. 8 years, after which all patients were offered intensified treatment over 21 years, focusing on albuminuria, GFR, ESRD and mortality Intensive=aggressive reduction targeting behaviour: smoking, exercise, diet, glycaemic control, blood pressure and dyslipidaemia
Multifactorial Rx in T 2 DM & legacy effect Trial: intensive vs conventional Post-trial: all intensive 80 Hazard ratio = 0. 47 (95% CI, 0. 24– 0. 73; p = 0. 008) 70 Conventional therapy 60 Cumulative 50 incidence of any CV 40 event (%) 30 53% reduction in CVD Intensive therapy 20 10 0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Years N=160 T 2 DM microalbuminuria STENO 2 TRIAL N Engl J Med 2008; 358: 580– 591.
Figure 1 Kidney International 2017 91, 982 -988 DOI: (10. 1016/j. kint. 2016. 11. 023) Copyright © 2017 International Society of Nephrology
Figure 2 Kidney International 2017 91, 982 -988 DOI: (10. 1016/j. kint. 2016. 11. 023) Copyright © 2017 International Society of Nephrology
Figure 3 Kidney International 2017 91, 982 -988 DOI: (10. 1016/j. kint. 2016. 11. 023) Copyright © 2017 International Society of Nephrology
Figure 4 Kidney International 2017 91, 982 -988 DOI: (10. 1016/j. kint. 2016. 11. 023) Copyright © 2017 International Society of Nephrology DOC= Death of other causes DCVD= Death of cardiovascular disease ESRD= End Stage Renal disease
Kaplan-Meier of combined renal endpoint to progression of GFR<45, ESRD or death Figure 5 Kidney International 2017 91, 982 -988 DOI: (10. 1016/j. kint. 2016. 11. 023) Copyright © 2017 International Society of Nephrology Solid line: intensive therapy Dashed line: conventional therapy
My passion Interface primary and secondary care
Why is there this wall between primary and secondary care ?
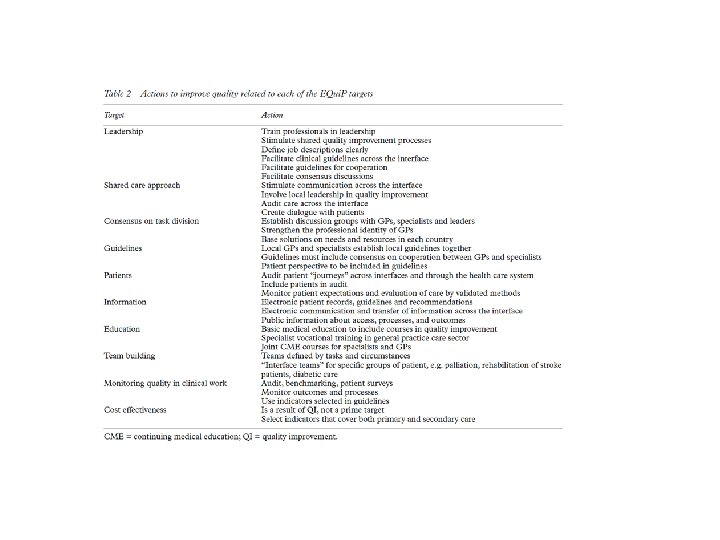
Quality in Healthcare 2001; 10: 33 -39
Monthly meeting GP’s and Hospital Doctors in Westeinde Hospital, The Hague
When to refer to a nephrologist
“Normal” GFR by Age (years) Average e. GFR 20 - 29 116 ml/min/1. 73 m 2 BSA 30 - 39 107 ml/min/1. 73 m 2 BSA 40 - 49 99 ml/min/1. 73 m 2 BSA 50 - 59 93 ml/min/1. 73 m 2 BSA 60 - 69 85 ml/min/1. 73 m 2 BSA > 70 years 75 ml/min/1. 73 m 2 BSA
Factors causing progression of CRF n Cont activity of primary disease n Systemic hypertension n Intraglomerular hypertension n Proteinuria n Nephrocalcinosis (dystr and metast) n Dyslipidaemia n Imbalance renal energy demands and supply
Cardiovascular Morbidity and Proteinuria Cumulative incidence (%) of CV morbidity 40 30 p < 0. 001 20 No Proteinuria 10 0 0 1 2 3 4 5 Years Adapted from Samuelsson et al. J Hypertens 1985; 3: 72 6 7 8 9 RPLM Hoogma 10
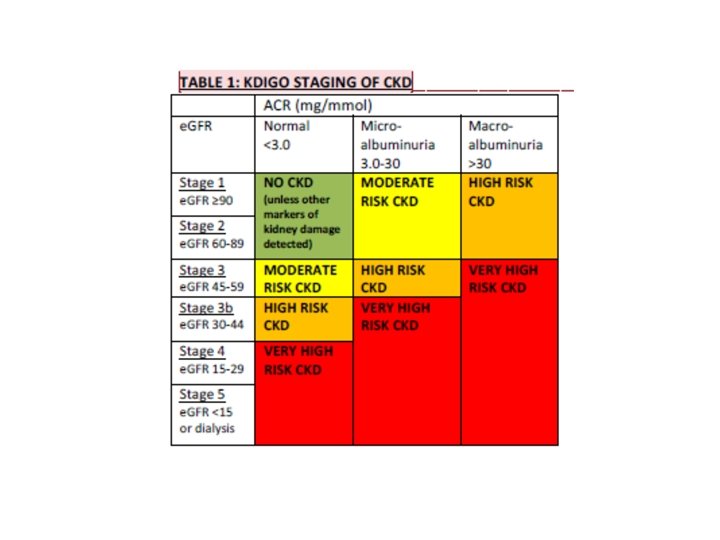
When to refer to renal physician? n e. GFR < 30 ml/min/1. 73 m 2 BSA n <45 in diabetics; anaemia (Hb < 100 g/L) n Proteinuria: persistent abnormal ACR and/or PCR n Glomerular haematuria n Difficult to control hypertension n Rapidly declining GFR n >15% in 3 months (Australia) n Electrolytes, vascular disease, etc. But: you can always call 0416 961 611
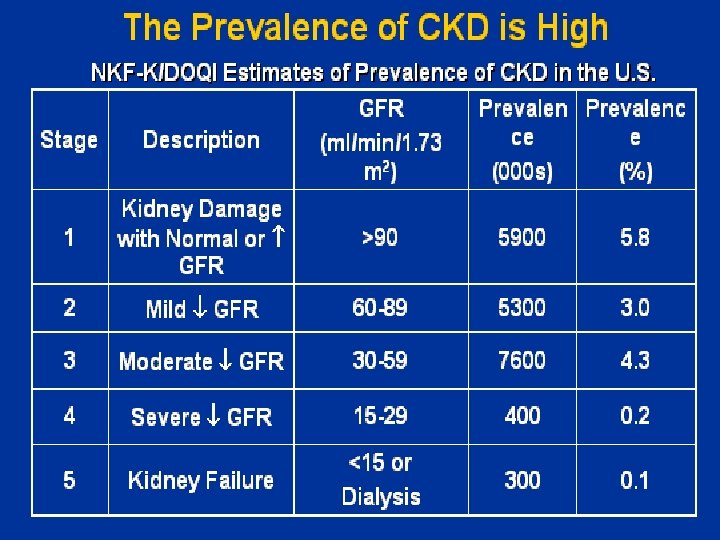
Early detection is paramount n CKD n Preventable ? ? ? n Growing @ 6%pa n Delayed progression n Renal abnormality is prevalent! n 16% of Australians (Aus. DIAB) n 15% NZers (Simmonds) n 20 x more likely to die than get RRT n Keith et al. Arch Int Med 164: 659; 2004 n Asymptomatic
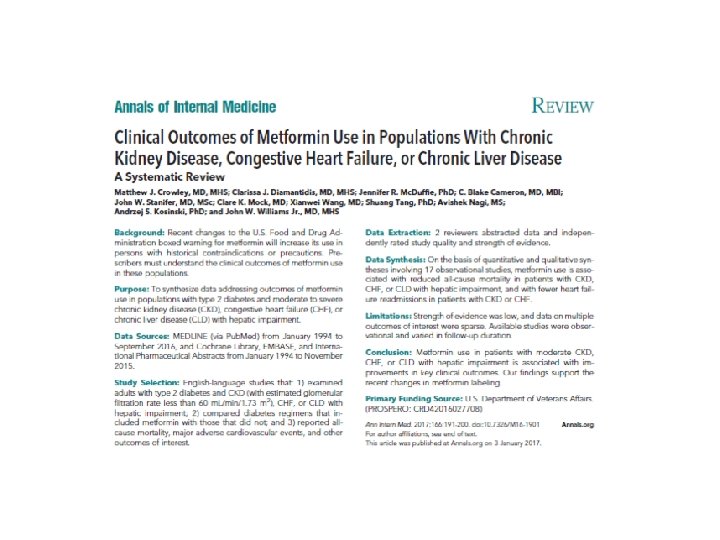
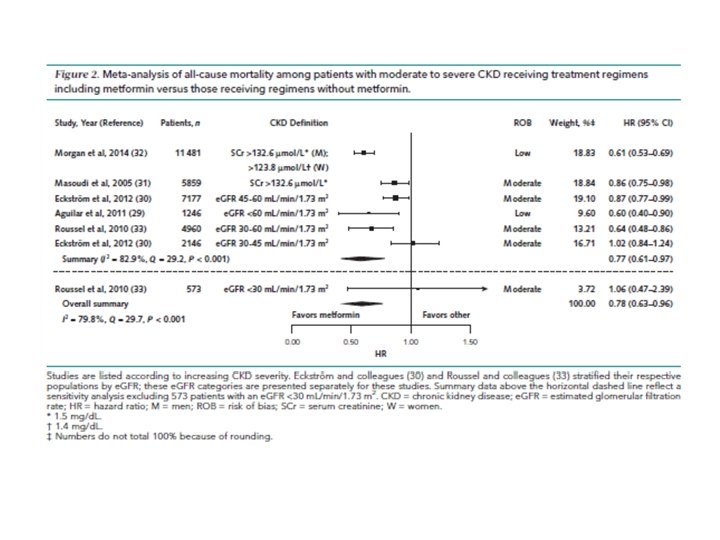
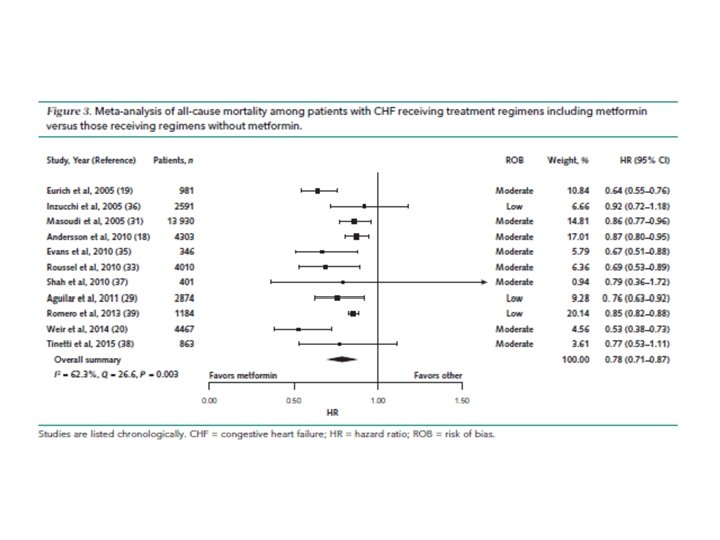
Methods • Systematic review of 17 observational studies comparing diabetes regimens with and without metformin • Metformin patients had lower all-cause mortality with heart failure, renal impairment, or chronic liver disease with renal impairment • Metformin use in patients with renal impairment or heart failure was associated with fewer heart failure readmissions • FDA-Labelling for metformin was revised to increase use and dose in patients with renal impairment • Contra-indication remained for those with e. GFR< 30 ml/min • The latter is highly contested, as lactic acidosis is extremely rare, and was basically only seen with the predecessor phenformin
If you do not know where you are going, you have to be careful as you may not get there Yogi Berra
Non-Pharmacological treatment of hypertension • • • Lifestyle Changes: smoking, alcohol, weight loss, exercise ? Related to 1): yoga, meditation, reiki Early 20 th century: surgical splanchnicectomy, replaced by the dream of medication as solution Renal denervation: radiofrequency or chemical Carotid Baroreflex Stimulation Carotid Body ablation
BP REDUCTIONS MATTER Small decreases make a difference: Reduction of 2 mm Hg lowers cardiovascular disease risk by up to 10% Meta-analysis of 61 prospective, observational studies • 1 Million adults 7% Reduction • 12. 7 Million persons-years in risk of IHD mortality Decrease of 2 mm Hg in mean SBP 10% Reduction in risk of stroke mortality SBP - systolic blood pressure; IHD - ischemic heart disease. SBP - systolic blood pressure; IHD - Lewington S et al. Lancet. 2002; 360: 1903 -1913.
‘Resistant Hypertension’ • Inadequate BP control despite at least 3 antihypertensive agents from different classes, including a diuretic (ESC-JNC 7) • Prevalence of resistant hypertension ranges from 5 -30% (population/center effects) • Obvious 2 nd causes to be excluded • Important role for aldosteron antagonists • Significant player: the sympathetic system, or the ‘Kidney-Brain’ link
The kidney-brain link
Sympathetic kidney-brain connection • In essential hypertension increased efferent sympathetic drive to the kidneys • This is evidenced by elevated ‘renal noradrenalin spillover’ • Definition: the amount of transmitter that escapes neuronal uptake and local metabolism and thus ‘spills over’ into the circulation, measured by radiotracer dilution methods • In essential hypertension there is also an increased rate of sympathetic ‘nerve firing’ (modulated by afferent signalling from renal sensory nerves) • Renal denervation techniques destroy the afferent and the efferent limb of this system !
Why Renal Denervation ?
The Symplicity Technique • Via femoral artery catherisation of renal artery • RA wall focally heated up to 50 -70°C with high frequency energy (8 Watt for 2 minutes) • Catheter withdrawn from distal to proximal in steps of at least 5 mm with ablation at each site • Typically 4 -6 areas in a spiral configuration • Procedure complete in 40 -60 minutes • Few post intervention complications, no signs of increased risk renal artery stenosis @ 2 years
Simplycity Renal Denervation
Symplicity HTN-1 Lancet 373: 1275 -1281, 2009 • Multicentre proof-of-concept trial • 50 patients (AU and EU), on average on 5. 1 drugs • Significantly lower BP after RD with FU 12 months • 9 patients drugs increased, 4 decreased • On average, patients remained on 4. 7 drugs • Renal noradrenalin spillover reduced by 47% • Longterm FU of 153 pat, including 45 from S-HTN-1: FU 2 years, efficacy persisted, no major complications
Symplicity HTN-2 Lancet 376: 1903 -1909, 2010 • Multicentre, prospective, randomized trial in 24 centres (weakness) • Random allocation to RD immediately or after 6 mo without med change • Primary outcome: SBP change after 6 mo • 106 patients randomized, 52 to immediate RD, 54 to delayed RD • Significant BP drop in treatment group, compared to controls • Safety good, major point transient bradycardia • Again, patients remained on anverage on 5. 1 drugs • Interesting: 25% experienced increase in e. GFR of >20%
Simplycity HTN-2 Lancet, 2010
Symplicity HTN-2 with 2 yr follow up
The case for Simplicity HTN-3 • There was no sham control group in HTN-1 + 2 • Bloodpressures were only recorded as office, not ambulatory 24 h • Long term effects unknown: efficacy (renal nerve fibers regenerate) and safety • Study was published in the NEJM and showed NO BENEFIT of renal denervation • In Australia currently a trial running that also uses a sham group as this studys’ methodology was poor
Potential other applications: Sleep apnea • Witkowski (Hypertension, 2011): 10 patients with resistant hypertension and OSA improved BP, frequency of apneas (4. 5 against 16. 3 events/hr), Epworth sleepiness scale • ? Mechanism: reduced sodium retention, improved volaemic status, hence less fluid shift to the neck in supine position, and/or improved venous compliance alleviating blood pooling in peripharyngeal tissues.
Potential other applications: Insulin resistance/Type 2 DM • Efficient BP control only achievable by multi level treatment of metabolic syndrome • Hyperinsulinaemia and increased sympathetic tone lead to sodium retention and hyperaldosteronism • Mahfoud (Circulation, 2011) showed that renal denervation in patients with resistant hypertension led to reduced BP, lower fasting glucose levels, reduction in insulin/c-peptide levels • Witkowski (Hypertension, 2011) confirmed a lower Hb. A 1 c after renal denervation • ? Mechanism: reduced sympathetic tone, reduced noradrenalin release, improved perfusion of skeletal muscles leading to better glucose uptake, RAAS inhibition, reduced gluconeogenesis, attenuation of glucagon secretion. • The DREAMS trial (Denervation of the Renal Artery in Metabolic Syndrome, NCT 01465724) is currently recruiting
Carotid baroreceptor stimulation Basically: stimulation of parasympathetic system by ‘irritating’ vagus nerve
The Carotid Body as a Therapeutic Target for the Treatment of Sympathetically Mediated Diseases by Julian F. R. Paton, Paul A. Sobotka, Marat Fudim, Zoar J. Engelman, Emma C. J. Hart, Fiona D. Mc. Bryde, Ana P. Abdala, Nepthali Marina, Alexander V. Gourine, Mel Lobo, Nik Patel, Amy Burchell, Laura Ratcliffe, and Angus Nightingale Hypertension Volume 61(1): 5 -13 December 12, 2012 Copyright © American Heart Association, Inc. All rights reserved.
Gross-anatomical appearance of the human carotid body (CB). Julian F. R. Paton et al. Hypertension. 2013; 61: 5 -13 Copyright © American Heart Association, Inc. All rights reserved.
Schematic representation of the carotid chemoreceptor and baroreceptor reflexes. Julian F. R. Paton et al. Hypertension. 2013; 61: 5 -13 Copyright © American Heart Association, Inc. All rights reserved.
In established hypertension, carotid body denervation (CBD) is antihypertensive, lowers respiratory rate (transiently) and the low frequency of systolic pressure in the spontaneously hypertensive rats (SHR). Julian F. R. Paton et al. Hypertension. 2013; 61: 5 -13 Copyright © American Heart Association, Inc. All rights reserved.
Blood pressure changes in patients after bilateral removal of the carotid body (CB). Julian F. R. Paton et al. Hypertension. 2013; 61: 5 -13 Copyright © American Heart Association, Inc. All rights reserved.
Cardiovascular and respiratory changes after bilateral removal of the carotid body (CB). Julian F. R. Paton et al. Hypertension. 2013; 61: 5 -13 Copyright © American Heart Association, Inc. All rights reserved.
Oh, these guidelines • • • They keep changing It feels like a diet-business Can we really generalize the proposed ones ? Can we do harm with them ? In the end, they work for the majority To me, they are often ‘democratic destruction of the minority’.
SPRINT and ACCORD (2010) • ACCORD did look specifically at diabetics t 2 • ACCORD had 4733 participants • Conclusion of Accord: in patients with type 2 DM, at high risk for cardiovascular events, targeting a BP of less than 120, instead of 140 mm. Hg, did not reduce the rate of a composite outcome of fatal and non-fatal major cardiovascular events.
Editorial: Outcomes Data from SPRINT and the ACCORD Trial and Combined Data from Both Trials
Differences SPRINT and ACCORD • ACCORD included diabetes only, SPRINT excluded diabetics • Sample sizes different (4733 vs. 9361) • SPRINT enrolled an older cohort and included patients with kidney disease • ACCORD showed a (non significant) 12% lower risk of its primary composite CV endpoint, so similar to SPRINT • ACCORD used a factorial design including glycemic control and lipid targets
2016 MJA 2016, in press (27. 05. 16)
Definition and Classification MJA 2016, in press (27. 05. 16)
Recommendations (details) • Lifestyle advice is recommended for all patients. GRADE: Strong; LEVEL: • For patients at low absolute cardiovascular disease risk (<10% 5 year risk) with persistent BP ≥ 160/100 mm. Hg antihypertensive therapy should be started. GRADE: Strong; LEVEL: I • For patients at moderate absolute cardiovascular disease risk (10 -15% 5 year risk) with persistent systolic BP ≥ 140 mm. Hg and/or diastolic ≥ 90 mm. Hg antihypertensive therapy should be started. GRADE: Strong; LEVEL: I • Once decided to treat, patients with uncomplicated hypertension should be treated to a target of <140/90 mm. Hg or lower if tolerated. GRADE: Strong; LEVEL: I • In selected high cardiovascular risk populations where a more intense treatment can be considered, aiming for a target of less than 120 mm. Hg systolic BP can improve cardiovascular outcomes. GRADE: Strong; LEVEL: II • In selected high cardiovascular risk populations where a treatment is being targeted to less than 120 mm. Hg systolic BP, close follow-up of patients is recommended to identify treatment related adverse effects including hypotension, syncope, electrolyte abnormalities and acute kidney injury. GRADE: Strong; LEVEL: II • In patients with uncomplicated hypertension angiotensin converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARB)s, calcium channel blockers, and thiazide diuretics are all suitable first line antihypertensive drugs, either as monotherapy or in some combinations unless contraindicated. GRADE: Strong; LEVEL: I • The balance between efficacy and safety is less favourable for betablockers than other first line antihypertensive drugs. Thus beta-blockers should not be offered as a first-line drug therapy for patients with hypertension that is not complicated by other conditions. GRADE: Strong; LEVEL: I • ACE inhibitors and ARBs are not recommended in combination due to an increased risk of adverse effects. GRADE: Strong; LEVEL: I MJA 2016, in press (27. 05. 16)
Chronic kidney disease Most classes of BP lowering drugs have a similar effect in reducing cardiovascular events and all-cause mortality in patients with chronic kidney disease (CKD). When treating with diuretics the choice should be dependent upon both the stage of CKD and the extracellular fluid volume overload in the patient. Detailed recommendations on how to manage patients with chronic kidney disease are available (18). • In patients with hypertension and CKD any of the first line antihypertensive drugs that effectively reduce BP are recommended. GRADE: Strong; LEVEL: Ib. • When treating hypertension in patients with CKD in the presence of micro- or macro- albuminuria an ARB or ACE inhibitor should be considered as first line therapy. GRADE: Strong; LEVEL: I • In patients with CKD, antihypertensive therapy should be started in those with BP consistently >140/90 mm. Hg and treated to a target of <140/90 mm. Hg. GRADE: Strong; LEVEL: I • Dual renin-angiotensin system blockade is not recommended in patients with CKD. GRADE: Strong; LEVEL: I • For patients with CKD, aiming towards a systolic BP of less than 120 mm. Hg has shown benefit, where well tolerated. GRADE: Strong; LEVEL: II • In people with CKD, where treatment is being targeted to less than 120 mm. Hg systolic BP, close follow-up of patients is recommended to identify treatment related adverse effects, including hypotension, syncope, electrolyte abnormalities and acute kidney injury. GRADE: Strong; LEVEL: I • In patients with CKD, aldosterone antagonists should be used with caution in view of the uncertain balance of risks versus benefits. GRADE: Weak; LEVEL: - MJA 2016, in press (27. 05. 16)
Diabetes • Antihypertensive therapy is strongly recommended in patients with diabetes and systolic BP ≥ 140 mm. Hg. GRADE: Strong; LEVEL: Ib. • In patients with diabetes and hypertension, any of the first line antihypertensive drugs that effectively lower BP are recommended. GRADE: Strong; LEVEL: I • In patients with diabetes and hypertension, a BP target of <140/90 mm. Hg is recommended. GRADE: Strong; LEVEL: I • A systolic BP target of less than 120 mm. Hg may be considered for patients with diabetes in whom prevention of stroke is prioritised. GRADE: Weak; LEVEL: • In patients with diabetes, where treatment is being targeted to less than 120 mm. Hg systolic BP, close follow up of patients is recommended to identify treatment related adverse effects including hypotension, syncope, electrolyte abnormalities and acute kidney injury. GRADE: Strong; LEVEL: -
Older persons • Any of the first line antihypertensive drugs can be used in older patients with hypertension. GRADE: Strong; LEVEL: I • When starting treatment in older patients, drugs should be commenced at the lowest dose and titrated slowly as adverse effects increase with age. GRADE: Strong; LEVEL: • For patients >75 years of age, aiming towards a systolic BP of less than 120 mm. Hg has shown benefit, where well tolerated, unless there is concomitant diabetes. GRADE: Strong; LEVEL: II • In older persons where treatment is being targeted to less than 120 mm. Hg systolic BP, close follow up of patients is recommended to identify treatment related adverse effects including hypotension, syncope, electrolyte abnormalities and acute kidney injury. GRADE: Strong; LEVEL: II • Clinical judgement should be used to assess benefit of treatment against risk of adverse effects in all older patients with lower grades of hypertension. GRADE: Strong; LEVEL: - MJA 2016, in press (27. 05. 16)
Main Recommendations Summary • For patients at low absolute cardiovascular disease risk with persistent BP ≥ 160/100 mm. Hg (Grade 2) antihypertensive therapy should be started. • The decision to treat at lower levels of BP should consider absolute cardiovascular disease risk, and/or evidence of end-organ damage, together with accurate BP assessment. • For patients at moderate absolute cardiovascular disease risk with persistent systolic BP ≥ 140 and or diastolic BP ≥ 90 mm. Hg antihypertensive therapy should be started. • Treat patients with uncomplicated hypertension to a target of < 140/90 mm. Hg or lower if tolerated. MJA 2016, in press (27. 05. 16)
Persistence and adherence in hypertensive patients typically falls over time Evaluated by medication event monitoring system Fall in persistence because of discontinuation of treatment Fall in adherence because of poor execution of dosing regimen Vrijens et al. BMJ 2008; 336: 1114 -1117.
Persistence at 1 Year With Antihypertensive Treatment Compliance at 1 Year (%) 65 64%* 60 58% 55 50 50% 45 43% 40 35 38% Diuretics Beta Blockers CCBs ACEIs ARBs *P<0. 007 vs. ACEIs Bloom BS et al. Clin Ther. 1998; 20: 671 -681.
Incremental SBP reduction ratio of observed to expected additive effects Two drugs are much more effective than doubling dose ACEI, antiotensin-converting enzyme inhibitor; CCB – calcium channel blocker. Wald et al. Am J Med 2009; 122: 290 -300.
Australian Heart Foundation Recommendations “Based on the best available evidence, the most effective combination is: ACE inhibitor/Angiotensin II Receptor Antagonist Plus Calcium Channel Blocker”
Advantages of fixed-dose combination therapy • Vast majority of patients require a combination of at least two drugs to achieve effective BP control 1 • Consider advantages of fixed-dose combination (FDC) therapy in terms of: – – – Pill burden Efficacy Tolerability Compliance Implementation 1. Mancia G et al J Hypertension 2009; 27: 2121 – 2158.
Advantages of FDCs vs. free-drug combinations: improved compliance FDCs should be preferred over free-drug combinations because simplification of treatment is associated with improved compliance 1 (and in Australia reduces patient-costs) Odds ratio 1. 5 Favours FDC 29% 1. 0 0. 5 Use of FDC associated with 29% increase in compliance and persistence compared with free-drug combination 2 Favours free-drug combination 1. Mancia et al. J Hypertens 2009; 27: 2121– 2158. 2. Gupta et al. Hypertens 2010; 55: 399– 407.
BP CRUSH: Patients with BP <140/90 mm. Hg (%) Majority of patients achieved BP target with triple combination therapy* Dual combination 100 Triple combination 86. 7 Total cohort N = 999 90. 3 77. 1 80 63. 8 60 49. 5 40 20 0 OLM/AML 20/5 mg (wks 0 -4) OLM/AML 40/5 mg (wks 4 -8) OLM/AML 40/10 mg (wks 8 -12) OLM/AML/HCTZ 40/10/12. 5 mg (wks 12 -16) OLM/AML/HCTZ 40/10/25 mg (wks 16 -20) Cumulative percentage of patients achieving an Se. BP goal of < 140/90 mm. Hg (secondary endpoint) at least once during the 20 week titrate goal study with a mean baseline BP of 153. 7/91. 9 mm Hg *olmesartan + amlodipine + hydrochlorothiazide Weir et al. J Clin Hypertens 2011; 13: 404– 412.
Modern antidiabetic treatment and the kidney
20 year projected global increase in diabetes IDF 2006 Diabetes Atlas 3 rd Ed.
CV events prevented by different interventions per 1000 patient yrs of treatment Preiss D , and Ray K K BMJ 2011; 343: bmj. d 4243
Individualise and prioritise therapy targets Individualise targets § Tight targets: for young motivated compliant patients, short duration of DM, no micro/macrovascular disease, few co-morbidities § Gentle targets: treat the elderly with respect – E. g. Systolic BP 110 vs 140, Hb. A 1 c 6 vs 8% Prioritise targets 1. BP and lipids: easier to achieve, bigger mortality benefit 2. Glucose control and weight loss
ACEi/CCB better than ACEi/HCT ACCOMPLISH n = 11500, ↑BP & CV risk → CV event or † CV Benazepril + amlodip 510 mg or HCT 12. 5 -25 Trial stopped early at 4 yrs due to 20% benefit for CCB arm: Both CV & CKD
1 mmol/L lower LDL = 22% fewer major CV events Cholesterol Treatment Trialists’ (CTT) Collaboration. Lancet 2010
Diabetic ESKD in Australia: 1980 -2010 From least common to most common cause of ESKD No. patients/year All growth due to T 2 DM
50% of Australian Type 2 diabetics have CKD 10% GFR < 60 & normal u. ACR 25% u. ACR & normal GFR 50% Either or both NEPHRON study MJA 2006; 185 (3): 140 -144 u. ACR = spot urine albumin: creatinine ratio
Missing factors in ATSI T 2 DM: chronic stress Cause: Chronic stress • Socio-economic • Family health Consequence: Cortisol • Insomnia • Constant hunger with central obesity • Insulin resistance with acanthosis • Resistant hypertension with relatively low K+ • Muscle weakness and fatigue • Recurrent infections Schmitt & Spargo Bio Soc Sci 1995
Therapy PRO CON Metformin Experience / Proven outcomes / Cost GI symptoms/ CKD Sulfonylurea Experience / Cost Hypo’s/ Wt. gain / CKD DPP 4 -i (gliptin) Wt. neutral / Low risk of hypo’s Cost / CCF (saxa, not sita) / CKD (except lina) / LFT’s (vilda) TZD (glitazone) Low risk of hypo’s Cost / Fluid retention / Wt. gain / Fracture risk / ? Bladder ca (pio) SGLT 2 -i (gliflozin) Wt. loss / SBP reduction / Low risk of hypo’s New / Dehydration / DKA $ / UTI & thrush / CKD inefficacy Acarbose Low risk of hypo’ / Wt. neutral / Cost Limited efficacy / GI tolerability GLP-1 (incretin analogue) Wt. loss / Low risk of hypoglycaemia Cost / Injection / GI symptoms Insulin Experience / Effective Injection / Wt. gain / Hypo’s 99
Pathophysiology of Hyperglycaemia: missing 3? Adrenal ↑Adrenalin, ↑cortisol Liver Brain Pancreas Decreased Insulin Secretion Increased Glucagon Secretion Increased Hepatic Glucose Production Hyperglycaemia Stress, Impaired satiety Gut Decreased Incretin Effect Muscle Fat Decreased Glucose Uptake Kidney Increased Glucose Reabsorption Adapted from De. Fronzo RA. Diabetes. 2009; 58: 773 -795. Increased Lipolysis 100
Sites/Modes of Action of Pharmacotherapy for T 2 DM Adrenal CBT, SSRI Liver Brain Pancreas CBT, SSRI Sulfonylureas Meglitinides GLP-1/DPP-4 i Gut Metformin TZDs DPP-4 i Hyperglycaemia Muscle TZDs Metformin α-Glucosidase inhibitors GLP-1/DPP-4 i Fat Kidney TZDs Metformin SGLT 2 inhibitors Adapted from De. Fronzo RA. Diabetes. 2009; 58: 773 -795. 101
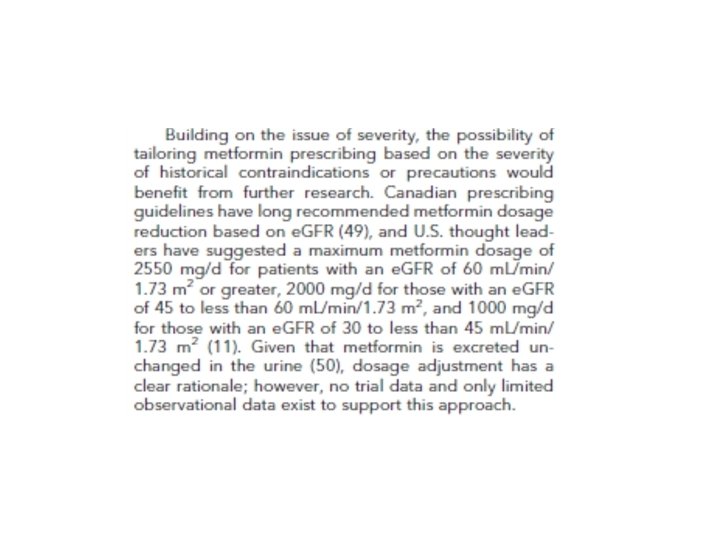
Drug modification in CKD Renally-excreted: dose-adjust to GFR as % § eg Metformin 2 g/day with GFR 30 -40 = 1000 mg/day Nephrotoxic: cease and repeat GFR § eg NSAID, diuretic, ACEI ↑CKD complication: reduce or cease § ↑BP: NSAID, decongestants, steroids § ↓Hb, ↑bleeding time : aspirin & clopidogrel § ↑urea: steroids
DPP 4 i safety – watch the BNP and lipase
Sodium glucose co-transporter (SGLT 2) inhibitors Induce prox tubular glycosuria Benefits: • reduce Hb. A 1 c 1% with few or no hypo’s used alone • lower weight & BP Risks: • dehydration (esp if on diuretics) • hypo’s with SU or insulin • UTIs, vulvovaginitis, balanitis Cefalu, Lancet Sept 2013
SGLT 2 i (Canagliflozin), Placebo & CKD: ↓wt, BP, GFR & u. ACR Wt GFR u. ACR BP Yale et al. doi: 10. 1111/dom. 12348
Gliflozin guidelines 20% reduction in insulin/ SU requirements 50% reduction in BP Rx/diuretic Issues: Daily BP, weight, BSL Daily groin/apron wash, dry, baby powder Zinc/castor oil if red, clotrimazole if thrush MSU pot & cephalexin, pre-emptive Rx if dysuria Hold SGLT 2 i if too symptomatic, try alternate daily
SGLT 2 i: CV benefit data CV † CCF Zinman, NEJM, Sept 2015
SGLT 2 i: CKD benefit data Wanner, NEJM, June 2016
Therapy PRO CON Metformin Experience / Proven outcomes / Cost GI symptoms/ CKD Sulfonylurea Experience / Cost Hypo’s/ Wt. gain / CKD DPP 4 -i (gliptin) Wt. neutral / Low risk of hypo’s Cost / CCF (saxa, not sita) / CKD (except lina) / LFT’s (vilda) TZD (glitazone) Low risk of hypo’s Cost / Fluid retention / Wt. gain / Fracture risk / ? Bladder ca (pio) SGLT 2 -i (gliflozin) Wt. loss / SBP reduction / Low risk of hypo’s New / Dehydration / DKA $ / UTI & thrush / CKD inefficacy Acarbose Low risk of hypo’ / Wt. neutral / Cost Limited efficacy / GI tolerability GLP-1 (incretin analogue) Wt. loss / Low risk of hypoglycaemia Cost / Injection / GI symptoms Insulin Experience / Effective Injection / Wt. gain / Hypo’s 110
Therapy PRO CON Metformin Experience / Proven outcomes / GI symptoms/ CKD BASELINE Cost Sulfonylurea Experience / Cost Hypo’s/ Wt. gain / CKD DPP 4 -i (gliptin) Wt. neutral / Low risk of hypo’s Cost / CCF (saxa, not sita) / CKD (except lina) / LFT’s (vilda) TZD (glitazone) Low risk of hypo’s SGLT 2 -i (gliflozin) Wt. loss / SBP reduction / Low risk of hypo’ Acarbose Low risk of hypo’ / Wt. neutral / TOO Cost GLP-1 (incretin analogue) Wt. loss / Low risk of hypoglycaemia Cost / Injection / GI symptoms Insulin Experience / Effective Injection / Wt. gain / Hypo’s Fluid retention / Wt. gain / Fracture TOO RISKY risk / ? Bladder ca (pio) New / Dehydration / DKA $ / UTI & thrush / CKD inefficacy Limited efficacy / GI tolerability WEAK 111
Therapy PRO CON Metformin Experience / Proven outcomes / GI symptoms/ CKD BASELINE Cost Sulfonylurea Experience / Cost Hypo’s/ Wt. gain / CKD HYPOs/WT GAIN DPP 4 -i (gliptin) Wt. neutral / Low risk of hypo’s Cost / CCF (saxa, not sita) / CKD (except lina) / LFT’s (vilda) SGLT 2 -i (gliflozin) Wt. loss / SBP reduction / Low risk of hypo’ New / Dehydration / DKA $ / UTI & thrush / CKD inefficacy GLP-1 (incretin analogue) Wt. loss / Low risk of hypoglycaemia Cost / Injection / GI symptoms Insulin GAIN/ Wt. gain / Hypo’s Experience / Effective. HYPOs/WT Injection 112
BYDUREON Pen: Microsphere technology enables once-weekly dosing 1, 2 Proven microsphere technology provides a continuous level of exenatide § Biodegradable polymer that dissipates into CO 2 and water § Technology used in extended-release products, e. g. risperidone & naltrexone Subcutaneous injection of microsphere suspension of exenatide Individual microspheres aggregate and initial release of exenatide Microsphere degradation and continued release of exenatide Adapted from 1. De. Young MB et al. 20111 Reference 1. De. Young MB et al. Diabetes Technol Ther 2011; 13: 1145– 54. 2. BYDUREON Approved Product Information. Further degradation and metabolism of microsphere polymer provide sustained level of exenatide
DURATION-2: BYDUREON vs sitagliptin or pioglitazone, on background metformin BYDUREON effective as first medication added to metformin 1, 2 At the primary endpoint of 26 weeks, Hb. A 1 c changes from baseline were – 1. 5% with BYDUREON, – 0. 9% with sitagliptin and – 1. 2% with pioglitazone (p<0. 05 for BYDUREON vs both comparators) 1 Hb. A 1 c reductions were sustained to week 52 throughout continued treatment with BYDUREON, or after switching from sitagliptin or pioglitazone to BYDUREON at week 262 Hb. A 1 c Change from Week 26 to Week 52: Change in Hb. A 1 c (%) -0. 5 -1. 0 -1. 5 -15 -2. 0 0 4 6 1 0 1 4 1 8 2 2 2 3 6 0 Time (weeks) 3 4 4 0 4 6 5 2 Change in Hb. A 1 c from baseline (mmol/mol) Sitagliptin BYDUREON – 0. 31% (95 % CI, – 0. 50 to – 0. 13), 0 P<0. 05 BYDUREON 0. 06% (95 % CI, – 0. 13 to 0. 25), P value not reported Pioglitazone BYDUREON – 0. 10% (95 % CI, – 0. 29 to 0. 09), -5 P value not reported 0. 0 -20 BYDUREON, BL=8. 6% (70. 5 mmol/mol) Sitagliptin BYDUREON, BL=8. 5% (69. 4 mmol/mol) Pioglitazone BYDUREON, BL=8. 5% (69. 4 Graph adapted from Wysham C, et al. 2011, showing data for the evaluable population as least squares mean mmol/mol) ± standard error. 2 BL=baseline; CI=confidence interval. Reference 1. Bergenstal RM, et al. Lancet 2010; 376: 431– 9; 2. Wysham C, et al. Diabet Med 2011; 28: 705– 14.
DURATION-3: BYDUREON vs insulin glargine Hb. A 1 c improvement with BYDUREON vs insulin sustained for 3 years 1 Insulin glargine (n=220) Once daily, variable dose based on treat-totarget algorithm* Exenatide QW (n=228) 2 mg once weekly 8. 5 Hb. A 1 c (%) 8. 0 7. 5 Δ -0. 20 % p=0. 03 7. 0 6. 5 0 8 1 8 2 6 3 6 4 8 6 0 7 8 2 4 Time (weeks) 9 6 1 0 8 12 0 13 2 14 4 Modified from Diamant M, et al. 2014. 1 *The daily dose of insulin glargine was based on the INITIATE algorithm (Initiate Insulin by Aggressive Titration and Education) and was individually adjusted to achieve fasting glucose values of 4. 0– 5. 5 mmol/l. In the Insulin glargine arm, from a starting daily insulin dose of 10 IU/day, mean dose increased to approximately 31 IU/day at 26 weeks. Background therapy: Metformin with or without sulfonylurea. Reference 1. Diamant M, et al. Lancet Diabetes Endocrinol 2014; 2: 464 -73. 15 6
DURATION-3: BYDUREON vs insulin glargine Weight change over 3 years 1, 2 Treatment with Bydureon resulted in significant weight reduction compared to weight gain with insulin glargine over 3 years 1* *BYDUREON is not indicated for weight loss. 2 Insulin glargine, BL=90. 6 kg (n=222) Bydureon, BL=91. 2 kg (n=233) Change in bodyweight (kg) 4 Change from BL: +2. 01 ± 0. 28 kg 2 0 -2 – 2. 49 ± 0. 28 kg* -4 0 8 1 8 2 6 3 6 4 8 6 0 7 8 2 (weeks) 4 Time 9 6 1 12 13 14 0 0 2 4 8 Graph adapted from Diamant M, et al. 2014, showing data for the modified intent-to-treat population as least squares mean ± standard error. 1 *p<0. 001. BL=baseline. Reference 1. Diamant M, et al. Lancet Diabetes Endocrinol 2014; 2: 464– 73; 2. BYDUREON Approved Product Information. 15 6
DURATION-2: individual efficacy vs weight change Hb. A 1 c 7 v 6. 5 Weight f. BSL Hb. A 1 c vs Weight Bergenstal et al. Lancet 2010 376; 431 -439
BYDUREON PEN: SUMMARY § BYDUREON is the first approved once weekly GLP-1 receptor agonist § Hb. A 1 c reductions are sustained for up to 6 years vs baseline† 2 § Potential for weight reduction over 6 years vs baseline* and low risk of hypoglycaemia†† 1, 2 § Most common adverse events: gastrointestinal (nausea, diarrhoea, vomiting, constipation), nasopharyngitis, hypoglycaemia, injection site reactions (pruritus, nodules, erythema, induration)1 †Open-label, uncontrolled extension study in patients administered BYDUREON with background therapy. 43% of patients remained in the study at Year 6. *BYDUREON is not indicated for weight loss. 1 ††SUs are associated with an increased risk of hypoglycaemia. When BYDUREON is added to SU therapy, a reduction in the dose of SU should be considered to reduce the risk of hypoglycaemia. 1 Reference 1. BYDUREON Approved Product Information. 2. Henry RH, et al. Poster presented at ADA 2014. 964 -P
Swedish Registry outcome data: GLP 1 a best All cause † All CVD GLP 1 a CHD CCF DPP 4 i & TZD GLP 1 a N = 20, 442, 2005 -2012. Ekstrom Diab Obes Metab 2016
GLP 1 analogue & CV outcome RCT N = 9340, >50 yr & CV factor, 3. 8 yr f/up, no DPP 4 i Primary EP = 3 -pt MACE: 13. 0 vs 14. 9%, HR 0. 87, p<0. 001 Marso, NEJM 2016
Take home messages (presentation on perthkidneys. com. au) Please do not get obsessed with guidelines as they apply to the ‘average’ patient Telehealth will increase to play an important role for remote patients and improves interaction GP, specialist and patient Exciting new anti diabetic drugs are in development that have promising effects on cardiovascular outcome but also on renal outcome. Could they with ACE/ARB become our new ‘neproprotective generation and combined with ACE and ARB even do better ? ?