Nephritic Syndrome Done by Ahmad AlMasri Its an

Nephritic Syndrome Done by: Ahmad Al-Masri

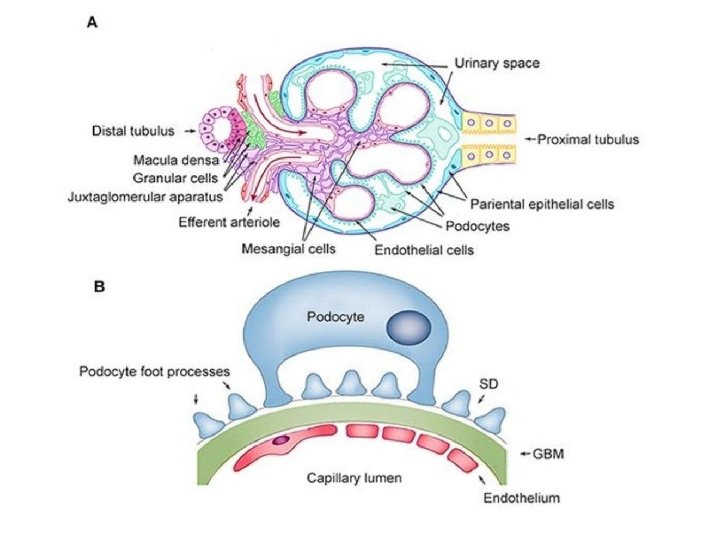
• It’s an Inflammatory process that involves glomeruli (damage involving the basement membrane , capillary endothelium , and mesangium) (while in nephr. Otic syndrome the main structure to be damaged is Podocyte) • Due to the glomeruli damage: • filtration barrier is weakened and enables passage of proteins , erythrocytes • ↓GFR Oliguria & ↑BUN/Cr ratio • ↑Hydrostatic pressure Hypertension & Edema
 Proteinuria (<3. 5 g/day) Swelling/edema Fatigue")
Classic presentation: • • • Dark urine (RBCs) Proteinuria (<3. 5 g/day) Swelling/edema Fatigue (uremia) Hypertension
 v. s. Secondary • Or classified")
Causes • Could be classified Primary ( idiopathic) v. s. Secondary • Or classified as Immune mediated v. s. Pauciimmune
 • is an acute GN resulting from the secondary sequelae")
Rapid progressive glomerulonephritis (RPGN) • is an acute GN resulting from the secondary sequelae of inflammatory (crescenteric) GN, of which there are many causes.

Crescenteric apperance Linear IF Granular IF Negative IF

Post-infectious GN • GN secondary to bacterial infection most commonly the nephritogenic strains of streptococcus (group A beta hemolytic streptococci). • Immune complexes deposit in subendothelial space. • Common in children (can also occur in adults) • Classic case: • Child presented 2 -3 weeks following strep throat infection or 6 weeks post impetigo with Nephritic syndrome findings

Post-infectious GN • If we take a Bx. we will see • Under light microscope: Enlarged, hypercellular glomeruli • Under immunofluorescence: Granular apperance (Ig. G, Ig. M, C 3) • Under Electron microscopy: Subepithelial “humps’’
 • Adults have worse")
Post-infectious GN • Good prognosis in children (95% recover completely) • Adults have worse prognosis (About 60% recover) • No specific therapy (supportive with management of high blood pressure and fluid overload , spontaneous resolution is expected )

Ig. A Nephropathy Berger’s Disease • Most common form glomerulonephritis in adults worldwide. • Most common cause of repeated episodes of hematuria (nephritic). • Typically cause hematuria 2 days post URTI or Diarrheal illness. • Over time leads to ESRD and HD (50% patients) • Affect mainly Males , especially Asian or white population.

Ig. A Nephropathy Berger’s Disease • Ig. A Immune complexes deposit in mesangium. • Bx. under immunofluorescence: Granular apperance (Ig. A) • Classic case: • Recurrent episodes hematuria since childhood, follow URI or diarrheal illness, Slowly worsening renal function (BUN/Cr) over time, Possible progression to ESRD and HD (20 yrs+) • Don’t confuse with other glomerular disorders 1) Post-strep GN: weeks after infection 2) Ig. A GN: days after infection 3) Minimal change: nephrotic syndrome after URI

Ig. A Nephropathy Berger’s Disease • Patients who have Ig. A nephropathy with a low risk of progressive disease should be treated with ACE-I to maintain a goal 24 hour urine protein excretion of less than 1 g /24 hours , and a blood pressure of less than 130 / 80. • Immunosuppressive therapy must be considered for: 1 - patients with persistent proteinuria ( more than 1 g/24 h) , 2 -progressive kidney dysfunction, 3 -or histological findings indicative of RPGN ( like crescents ) This includes pulse corticosteroids and cyclophosphamide followed by azathioprine with ACE-I. • Few studies shows that Fish Oil have role in delay some of the late complications of Ig. A nephropathy

Henoch-Schonlein Purpura • • Ig. A nephropathy + extra-renal involvement Skin: palpable purpura on buttocks/legs GI: abdominal pain, melena Joint pains Most common childhood systemic vasculitis Diffuse Ig. A deposition Tissue biopsy: demonstrates Ig. A

Lupus Nephritis • They are subdivided into 6 types, here in nephrtic syndrome we are concern with type lll (Focal Proliferative lupus nephritis) & type IV (Diffuse Proliferative lupus nephritis). • Focal: less than 50% glomeruli affected • Diffuse: More than 50% glomeruli affected • Anti-ds. DNA Subendothelial deposits

Lupus Nephritis • If we take a Bx. we will see • Under light microscope: capillary loops thickened • “Wire looping” • Under immunofluorescence: Granular apperance • “Full house” immunofluorescence (Ig. G, Ig. A, Ig. M, C 3, C 1 q)

Lupus Nephritis • Usually we take Bx. To know the severity to decide the prepare treatment. • Steroids alone or with Cyclophosphamide?

Membranoproliferative glomerulonephritis • Also called mesangiocapillary GN. • Immune complex formation secondary to chronic antigen stimulation. • Common causes are : 1. Chronic indolent infections including hepatitis C, syphilis , mastoiditis …etc. . 2. Autoimmune such as Sjogren , lupus …etc. 3. Essential cryoglobulinemia ( types I and II ) 4. Malignancies such as carcinomas , sarcomas , lymphomas and leukemias.

immune-complex and/or complement protein deposition in the mesangium and sub endothelium of the capillaries this results in proliferation of the mesangial and remodeling of the capillary wall

• We usually treat them with: 1. Corticosteroids 2. Immunosuppressive agents 3. Antiplatelets • More than 50 % progress to advanced CKD.

Anti-GBM antibodies disease Goodpasture’s Syndrome • Ig. G antibodies develop against the GBM (alpha-3 chain to type IV collagen ) , deposited in a linear patter. • Classic case: • Young adult, Male present with Hemoptysis & Hematuria • Treatment usually is Plasmapheresis using albumin replacement for 1 -2 weeks , followed by corticosteroids and cyclophosphamide for 3 -6 months , Maintenance with azathioprine for 1 -2 years
 • All vasculities are")
Vasculities syndrome • Most patients ANCA positive (c-ANCA or p-ANCA) • All vasculities are associated with Fever + weight loss. • Churg-Strauss syndrome (p-ANCA): they present with Eosinophilia, history of resistant asthma. • Wegener's Granulomatosis (c-ANCA): they present with upper respiratory findings (sinusitis/otitis) • All can lead to pauci-immune nephritis

Alport Syndrome Hereditary Nephritis • Genetic Mutations in alpha-3, alpha-4, or alpha-5 chains of type IV collagen. • Chains found in basement membranes kidney, eye, ear • Inherited: X-linked • Classic triad: • Hematuria, Hearing loss, eye abnormalities • Look for child with triad and family history

Thank You
- Slides: 24