NEOPLASMS OF THE GASTROINETESTINAL TRACT Prof Dr Ferenc














 Nx Regional lymph nodes")

")






 SARCOMA OF THE STOMACH Leiomyosarcoma GIST (Gastrointestinal stromal tumor) 1 -3% of")

 Personal history")













 Random")




 Random")




 Biliary truct")





- Slides: 57
NEOPLASMS OF THE GASTROINETESTINAL TRACT Prof. Dr. Ferenc Szalay 1 st Department of Semmelweis University Budapest, 2005
Neoplasms of the Gastrointestinal Tract Npls of GI tract continue to be the most common malignant tumors Esophagus Stomach Pancreas Liver Biliary tract Small bowel Colon
ESOPHAGUS Squamous cell cc. Adenocarcinoma INCIDENCE 5/100. 000 black men 4 -5 x more comonly affected mail > femail dramatic regional differences in certain areas of China: incidence 1: 1000 adenocarcinoma in western countries
ESOPHAGUS ETIOLOGY and PATHOGENESIS Cause of squamous cell cc. is unknown Enviromental factors: tobacco alcohol abuse lye ingestion, hot tea radiation long term stasis (achalasia) Adenocarcinoma association with Barrett’s GERD inherited disorder: tylosis
Normal
Barrett’s oesophagus
Barrett’s dysplasia Columnar cells instead of squamous cells
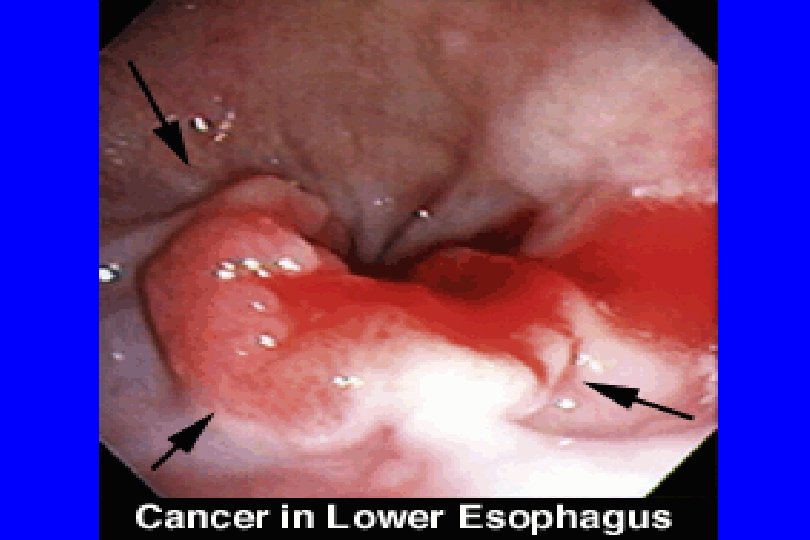
Adenocarcinoma of esophagus
ESOPHAGUS CLINICAL MANIFESTATIONS Dysphagia Anorexia Weight loss Regurgitation Fistula Pain Hoarsness GI bleeding solid food 2 nd liquids 1 st aspi ration pneumonia tracheooesophageal due to impingement of laryngeal nerve occult iron deficient anemia massive and fatal if erodes aorta
ESOPHAGUS COMPLICATIONS Silent Symptomatic Metastatic no serosal lining metastasize early to regional lymph nodes
ESOPHAGUS DIAGNOSIS Double contrast barium Endoscopy biopsy - cytology, histology CT Endoscopic ultrasonography
Radiographic evaluation in suspected esophageal cancer
Gastroesophageal junction type II tumors
Esophageal cancer
AJCC Staging of Esophagus: TNM Staging Regional lymph nodes (N) Nx Regional lymph nodes cannot be assassed N 0 No regional lymph node metastasis N 1 Regional lymph node metastasis Distant metastasis (M) Mx Distant metastasis cannot be assassed M 0 No distant metastasis M 1 Distant metastasis Tumors of lower or upper esophagus M 1 a Metastasis in nonregional lymph node M 1 b Distant metastasis (eg: liver, bone, brain) Tumors of middle esophagus M 1 a Not applicable M 1 b Metastasis in nonregional lymph node or distant metastasis (eg: liver, bone, brain)
AJCC Staging of Esophagus: TNM Staging Stage Tumor Node Metastasis Stage 0 Stage I Tis T 1 T 2 T 3 T 4 Any T N 0 N 0 N 1 N 1 Any N M 0 M 0 M 1 a M 1 b Stage IIA Stage IIB Stage III Stage IV A Stage IV B
ESOPHAGUS TREATMENT Surgical resection: cure only in 10 -30% Palliation: radiation plastic tube (prosthesis) metal stent dilatation endoscopic laser thermal
Resected esophageal specimen
CARCINOMA OF THE STOMACH INCIDENCE and predisposing factors Adenocarcinoma > 90% of malignant tumors of the stomach Since 1940 s unexplained decrease in incidence Marked variation: High rate in Japan, South America, Eastern Europe Following emigration very slowly Helicobacter pylori Diet high salt and nitrates Pernicious anemia - atrophic gastritis
CARCINOMA OF THE STOMACH CLINICAL MANIFESTATIONS Clinical presentation depends on morphologic characteristics: infiltrating or ulcerating size of the tumor presence of gastric outlet obstruction metastatic or nonmetastatic Pain Nausea and vomiting Anorexia Iron deficiency anemia Paraneoplastic signs
CARCINOMA OF THE STOMACH DIAGNOSIS Upper endoscopy BIOPSY histology Endoscopic sonography Double contrast barium
CARCINOMA OF THE STOMACH TREATMENT and PROGNOSIS Surgery only 1/3 are resectable for cure Curative for early gastric cancer Survival for most patients< 5%
LYMPHOMA OF THE STOMACH Relatively uncommon <15% of gastric malignancies 2% of all lymphomas most frequent extranodal site for lymphoma increased in frequency durint the past 25 ys Non-Hodgkin’s lymphoma (vast majority) Hodgkin’s lymphoma is uncommon MALT (mucosa associated lymphoid tissue) - H. p. Treatment: Subtotal gastrectomy, combination chemotherapy, Helicobacter pylori eradication
GASTRIC (NONLYMPHOID) SARCOMA OF THE STOMACH Leiomyosarcoma GIST (Gastrointestinal stromal tumor) 1 -3% of gastric npls. All such tumors should be analyzed for mutation in the ckit receptor GISTs are unresponsive to conventional chemotherapy 50% respond to imatinib mesylate (Gleevec), a selective inhibitor of the c-kit tyrosinase kinase
CARCINOMA OF THE COLON INCIDENCE and predisposing factors 3 rd most comon cc. in men, 2 nd in women 3 rd most common cause of cancer death CRC is 15% of all malignant tumors More comon in developed countries Emigrants get the risk characteristic for new enviroment Role of diet Genetic factors
CARCINOMA OF THE COLON RISK FACTORS Increasing age Inflammatory bowel disease (UC) Personal history of colon cancer or adenoma Family history of colon cancer Familial polyposis syndromes (adenomatous polyps) History of breast or female genital cancer Peutz-Jeghers syndrome (hamartomas)
CARCINOMA OF THE COLON ETIOLOGY and PATHOGENESIS Enviromental factors Diet low in fiber Diet high in animal fat and protein Toxic bile acids (role of colonic bacteria) Role of different factors: calcium, vitamin-D selenium COX system Unknown ? ? Oncogens Genetic factors
Low fiber → High concentration of gut bile acids (low dilution and prolonged contact through lack of bulk) and fecal mutagens / carcinogensis High concentration of bile and metabolits → Promoting effect in colon carcinogenesis Mechanisms under study Fried food → Mutagens → Colon carcinogenesis? Role of fecal flora? Role of micronutrients (vitamins, minerals, antioxidants) and different types of fiber in production and metabolism of carcinogens, bile acids, promoters? Specific role of calcium (formation of insoluable calcium phosphate / bile acids? Direct effect on proliferation? ) Mechanisms of promotion?
Genes altered in colon cancer Gene Chromosome Sporadic tumors with alterations, Class % Function K-ras 12 50 Protooncogene Signal transduction APC 5 60 Tumor supressor ? Cell adhesion DCC 18 70 Tumor supressor ? Cell adhesion p 53 17 75 Tumor supressor Cell cycle control (G 1/S arrest) h. MSH 2 2 DNA Mismatch repair Maintains fidelity of DNA replication h. MLH 1 3 DNA Mismatch repair Maintains fidelity of DNA replication
CARCINOMA OF THE COLON CLINICAL MANIFESTATIONS Few early warning signs Depend on location, size, bleeding tendency GI blood loss occult blood melaena hematochezia Alteration of bowel habits (left sided or distal tumors) Owerflow diarrhea (severe but incomplete obstruction) Abdominal pain (uncommon, obstuction related) Weight loss, anorexia (nonspecific, appear late) Perforation, malignant ascites, liver metastasis
Colonic obstruction from a carcinoma of the transverse colon Dilated small and large bowel proximal to the lesion Collapsed bowel distal to the obstructing carcinoma
CARCINOMA OF THE COLON DIAGNOSIS History: Should be suspected over age 40 with symptoms of GI blood loss, etc. Digital rectal examination Double-contrast barium enema Colonoscopy Biopsy Carcinoembrionic antigen (CEA) useful in follow-up surgery to detect recurrence
CARCINOMA OF THE COLON TREATMENT and PROGNOSIS Surgery remove tumor and adjacent colon and mesentery preoperative CT to exclude synchronous colon tu. and metastases procedure depends on location of the tumor save sphyncter ani if possible Radiation Chemotherapy (5 -FU, irinotecan, cysplatin) Palliative Follow-up after surgery
CARCINOMA OF THE COLON SCREENING AND PREVENTION Link between adenomatous polyps and cancer ! Testing for occult fecal blood over age 40 -50 y Colonoscopy over age 50 y Colonoscopy in high risk population Diet
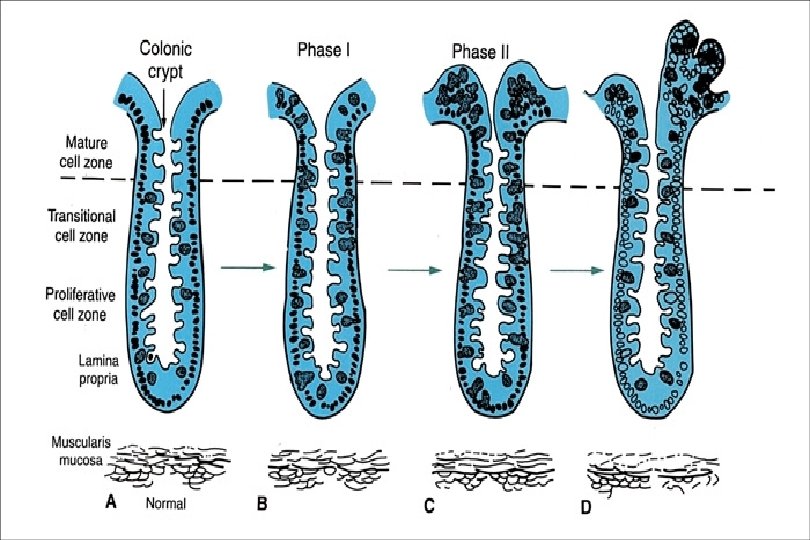
POLYPS OF THE GASTROINTESTINAL TRACT Overgrowth of tissue, usually of epithelial cells, that arises from the mucosal surface and extends into the lumen of the GI tract single or sporadic or pedunculated (stalk) or neoplastic or benign or multiple familial sessile (flat base) non-neoplastic malignant May occure enywhere throughout the GI tract
Large pedunculated polyp
Pedunculated polyps
Large sessile polyp
POLYPS OF THE GASTROINTESTINAL TRACT INCIDENCE Adenomatous colonic polyps are very comon Increase with age 50 year-old 20% chance 70 year-old 40% chance Patients with one polyp have higher frequency of synchronous P. greater potential for additional P. over time
POLYPS OF THE COLON Neoplastic Polyps Bening adenomatous polyps (tubular, mixed or villous) Random occurences Familial- familial polyposis of the colon Gardner’s syndrome Turcot’s syndrome, family cancer syndrome Malignant polyps- carcinomatous changes, in situ or invasive
Tubular adenoma of the colon
Tubulovillous adenoma
Tubulovillous adenoma
Percent of adenomas containing invasive cancer Adenoma size, cm
POLYPS OF THE COLON Neoplastic Polyps Bening adenomatous polyps (tubular, mixed or villous) Random occurences Familial- familial polyposis of the colon Gardner’s syndrome Turcot’s syndrome, family cancer syndrome Malignant polyps- carcinomatous changes, in situ or invasive Non-Neoplastic Polyps Inflammatory „pseudopolyps” Peutz-Jeghers syndrome - hamartomas Mucosal polyps with normal epithelium Juvenile polyps
Hereditary nonpolyposis colorectal cancer Three or more relatives with colorectal cancer (one must be first-degree relative of other two) Colorectal cancer involving at least two generations One or more colorectal cancer cases before age 50
Characteristics HNPCC Mean age at diagnosis, y 44. 6 Multiple colon cancers, % 34. 5 Synchronous 18. 1 Metachronous 24. 3 Proximal location, % 72. 3 Excess malignancies at other sites Yes Mucinous and poorly differentiated cancers Common RER + % 79 Sporadic 67 4 -11 3 -6 1 -5 35 No Infrequent 17
Cutaneous manifestations of gastrointestinal tract polyposis syndromes Familial adenomatous polyposis and Gardner's syndrome Epidermoid cysts Desmoid tumors Pigmented lesions Peutz-Jeghers syndrome Mucocutaneous pigmentation Multiple hamartoma syndrome (Cowden's disease) Trichilemmomas Oral mucosal papillomatosis Cowden's fibroma Acral keratoses Muir-Torre syndrome Sebaceous hyperplasia Sebaceous adenomas Sebaceous epithelioma Sebaceous carcinoma Multiple keratoacanthomas
TUMORS OF THE LIVER Benign Tumor-like Malignant Metastatic
TUMORS OF THE LIVER Benign Hemangioma Hepatocellular adenoma Focal nodular hyperplasia (FNH) Biliary truct adenoma Intrahepatic cytadenoma
TUMORS OF THE LIVER Tumor-like Soliter cysts Polycystic liver Echinococcus cyst Liver abscess Haematoma Hamartoma
TUMORS OF THE LIVER Malignant Hepatocellularis carcinoma Fibrolamellar carcinoma Hepatoblastoma Cholangiocarcinoma Angiosarcoma Metastatic From any organ except brain
PBC talaján, a diagnózis után 18 évvel kialakult HCC A szérum AFP értéke a halál előtt 3480 ng/ml volt (norm: 0 -15 ng/ml) Immunhisztológiai vizsgálat: a piros foltok jelzik az AFP pozitivitást
Polycystás máj 1 cm
Májmetastasis különböző megjelenései