Neonatal Physical Assessment Sabha Mariam Alaa Nabila Nermin

Neonatal Physical Assessment Sabha. Mariam. Alaa. Nabila. Nermin

physical examination The aim of the first examination performed within 24 hours of birth is to detect any observable congenital malformations. “The baby should have a complete physical examination within 24 hours of birth, as well as within 24 hours before discharge”.

Apgar scoring 1. The Apgar score helps find breathing problems and other health issues. 2. It is part of the special attention given to a baby in the first few minutes after birth. 3. The baby is checked at 1 minute and 5 minutes after birth for heart and respiratory rates, muscle tone, reflexes, and color. 4. A baby who needs help with any of these issues is getting constant attention during those first 5 to 10 minutes. 5. Each area can have a score of 0, 1, or 2, with 10 points as the maximum. 6. Most babies score 8 or 9. 7. Apgar scores of 6 or less usually mean a baby needed immediate attention and care.

The Apgar Scoring System Sign Score = 0 Absent Score =1 2 = Score Below 100 Above 100 Heart rate per minute Breathing Absent Weak, irregular, or Good, crying effort gasping Flaccid Some flexing of Well-flexed, or active Muscle tone arms and legs movements of arms and legs Reflex or No response Grimace or weak Good cry irritability cry , Blue all over , Body pink hands Pink all over Color or pale and feet blue

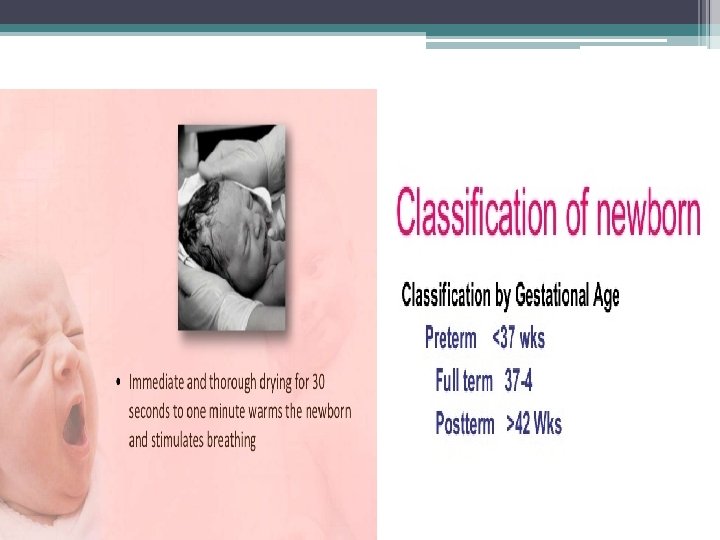
Measurement There are 3 components for growth measurements in neonates : 1. Weights: - A healthy term baby weights approximately 2. 6 kg - 3. 8 kg. - Babies less than 2. 5 kg are considered low birth weights.

2. Length - Acceptable newborn lengths ranges from 48 – 52 cm at birth.

3. head circumference : - The head circumference measurement of the occipitofrontal diameter should be in the range of 32– 36 cm for a term baby.

4. Chest circumference - Normal range 33 – 35 cm.

Vital Sings : 1. Temperature - should be taken axillary. - the normal temperature for newborn is 36. 5 – 37. 50 c. & Methods of heat loss : Convection. Radiation. - Evaporation. - Conduction. - -

2. Respiratory rate & Heart rate Normal respiratory rate is 30 – 60 / minute. Normal heart rate is 100 – 160 beat / m.

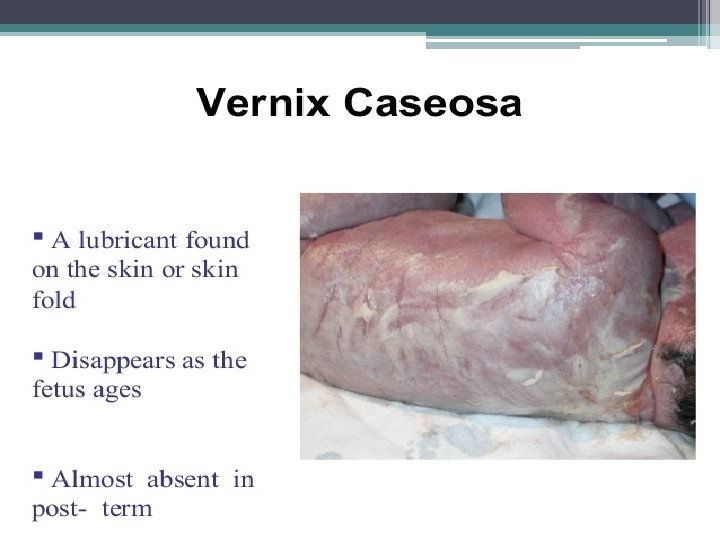
Assessment of the neonatal skin The colour of the skin is generally considered a reflection of good health, but is most difficult to assess accurately in the first few hours of extra uterine life and the midwife needs to distinguish between different types and degrees of blue skin to know if the baby is well or whether to refer to the neonatal registrar.

A blue skin as a result of other factors * Most babies will have peripheral shutdown (acrocyanosis) * Jaundice * Perioralcyanosis

* petechiae which are pinpoint hemorrhagic spots on the skin, usually as a result of a tightening cord around the neck * Rashes Words to describe rashes vesicles Pustules Flat& Red

Port wine stain: red, purple markings

Common skin lesions found at birth Vascular birth marks found at birth Vascular proliferations or ‘stork marks: uperficial capillaries blanche on pressure, esolve spontaneously Strawberry haemangioma: bright red in colour Cavernous haemangioma: similar to the strawberry but invades deeper into the vascular tissues Vasculature malformations Mongolian blue spots: blue-black discoloration usually found over the buttocks Pigmented naevi : a dark brown patch on the lower back with speckles. Milia : small white follicular cysts commonly known as milk spots.

Assessment of the neonatal head
 closes")
The bones, sutures and fontanelles can then be examined *The posterior fontanelle (lambda) closes around 6 weeks. *The anterior fontanelle (bregma) closes at 18 months of age.
 large head is also")
Abnormal head macrocephaly microcephaly (greater than the 97 th centile) large head is also associated with hydrocephaly and congenital syndromes. (below the 2 nd centile) small head is associated with poor brain development.

Cephalhematoma is a subperiosteal collection of blood between the skull and the periosteum. * Disappear within afew weeks. caput succedaneum Observation and palpation of the scalp will indicate the presence and degree of caput succedaneum which will resolve in 2– 3 days.

Anencephaly is the absence of a major portion of the brain, skull, and scalp that occurs during embryonic development

Encephalocele A sac-like protrusion of the brain through an opening in the midline of the skull.

Cuts, abrasions and bruises These are carefully assessed as they may serve as portals of entry for infection.

congenital torticollis q q The head may be held to one side and is the result of traction and tearing of the muscle. Physiotherapy referral will be made once diagnosed

Assessment of the neonatal face Facial palsy ü affected side of the face droops and the infant is unable to close the eye tightly on that side. When crying the mouth is pulled across to the normal side. ü This is a result of damage to the seventh cranial nerve (facial), known as Bell's palsy, during the application of forceps or from head compression against the sacral promontory during birth. ü Spontaneous resolution is usually within 7– 10 days; this may extend to months or years if the damage is severe

Eye: The eyes should be symmetrically positioned on the face in relation to the other facial features such as eyelids, eyebrows and the slant of the palpebral fissures. q The outer and inner canthal distance can be divided equally. * Cataracts q – Eyes appear cloudy

Ear: q The ear position should be similar on both sides. q Malformed and/or low set ears are associated with chromosomal abnormalities or urogenital malformations and warrant referral. argue that peri-auricular skin tags can indicate hearing impairment. q Normal ear tag microtia peri-auricular

Mouth Lip and Palate: q Cleft lip can be either unilateral or bilateral and can extend into the hard and soft palate. q A cleft palate is not always obvious and requires thorough assessment in order to confirm its presence.

q q Cleft lip and/or palate may be familial or may be as a result of maternal medication (e. g. phenytoin) or chromosomal abnormality (e. g. Down syndrome). The baby may also experience problems with feeding.

Chin Normal chin Microganthia

ankyloglossia A tight frenulum that is attached too far forward to the floor of the mouth restricts mobility of the tongue to different degrees and will give the appearance of tongue-tie (ankyloglossia). * Treatment for severe tongue-tie is frenulotomy (surgical division of the frenulum), especially when breastfeeding is being adversely affected.
")
Chest In drawing (Retractions)

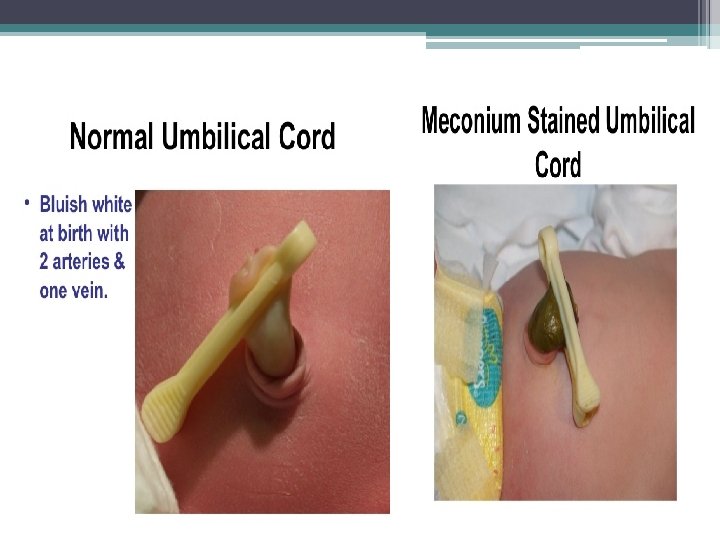
umbilicus o o The cord should be checked for bleeding. The cord vessels should have two arteries and one vein. AA v

comparison OMPHALOCELE • The internal organs remain in a sac • Protrudes through the umbilicus GASTROSCHESIS • The umbilical cord is not involved • The internal organs are NOT enclosed in a sac

Anus Inspection for the presence and appearance of the anus is vital. o The presence of meconium does not always exclude imperforate anus (anal atresia). o

Spine or back assessment : Spina bifida: defect in closure of the neural tube that is associated with malformation of the vertebra & spinal cord.

Saccrococcygeal Teratoma * A tumor found in the midline of the body. • In newborns, the most common location is the sacrococcygeal region- at the base of the spine. • This is a mass of tissue, and does not come out of the spinal cord as in Spina bifida.

Limbs, hands and feet normal hand

Erb's palsy * is a paralysis of the arm caused by injury to the upper group of the arm's main nerves, * (C 5, 6) - Upper Lesion. Klumpke's palsy * is a variety of partial palsy of the lower roots of the brachial plexus. * (C 8, T 1) - Lower lesion.


Neurological Examination • Means looking at muscles and nerves Hypotonia

Thank You
- Slides: 46