NEONATAL JAUNDICE DR NADEEM ALAM ZUBAIRI MBBS MCPS

NEONATAL JAUNDICE DR NADEEM ALAM ZUBAIRI MBBS, MCPS, FCPS Consultant Neonatologist / Paediatrician


Scenario 1 • A baby boy is born 3. 5 kg to a mother as a result of SVD. He did not need any resuscitation at birth and went home within 24 hrs. Mother noticed him to be jaundiced on D 3 of life and brought him to you.

Scenario 1 Continued • A house officer takes history and asks following questions. – When did the mother first notice jaundice? • After first 24 hrs – Is this mother’s first pregnancy / H/O abortions? • She is a primigravida – Is the baby breast fed? • Exclusively and feeding well – What is the color of the stool? • Yellow

Scenario 1 • House officer makes a provisional diagnosis of: Physiological Jaundice – Serum total bilirubin – Mother and baby’s blood group – FBC, retics and peripheral film Continued

Scenario 1 Continued • Serum bilirubin 180 umol/l on day 3 of life( 10 mg/dl) • • • FBC Hb 18. 3 g/dl, retics 2% TLC 18 x 103 Baby’s blood group A+ Mother A+ Coomb’s test Negative

Scenario 1 Continued

Scenario 1 Physiological Jaundice Why ? Continued

EXCLUSION CRITERIA Ø Unconjugated bilirubin > 12. 9 mg/dl Ø Bilirubin level increasing > 5 mg/dl/day Ø Jaundice in first 24 hours of life Ø Conjugated bilirubin level > 2 mg/dl Ø Clinical jaundice persisting > 2 week

Neonatal Jaundice • Hyperbilirubinemia in infants ≥ 35 weeks gestation is defined as a TSB >95 th percentile for hours-of-age on the Bhutani nomogram PHYSIOLOGIC & PATHOLOGIC JAUNDICE

Bilirubin Metabolism

Mechanism of Neonatal Jaundice • Increased production of bilirubin • Decreased uptake • Decreased conjugation • Increased enterohepatic circulation

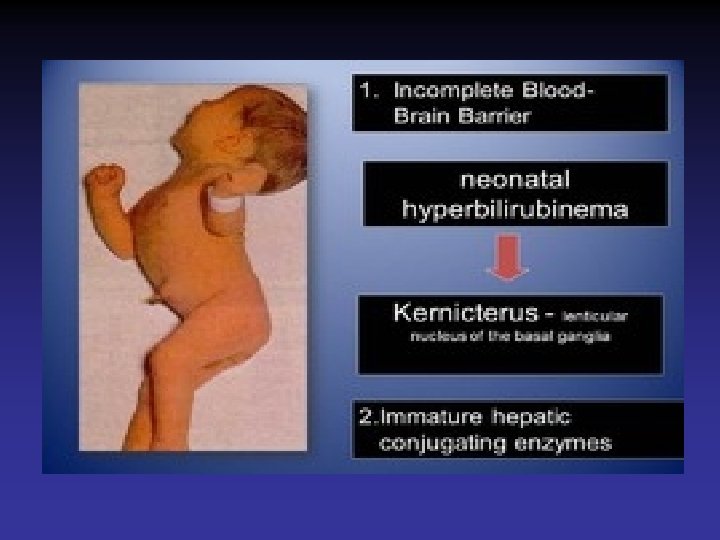
Why do newborns develop physiological jaundice? • Decreased RBC life span • Decreased Y protein and Ligandin in liver • Decreased activity of UDP glucronyl transferase • Increased enterohepatic circulation

Physiological Jaundice • Appear after 24 hours • Maximum intensity by 4 th-5 th day in term & 7 th day in preterm • Clinically not detectable after 14 days • Disappears without any treatment

Scenario 2 • A baby boy is born to a multigravida mother at term gestation following an uneventful pregnancy. He develops jaundice at 16 hours of age.

Scenario 2 Continued • A house officer takes history and asks following questions. – When did the mother first notice jaundice? • Within 1 st 24 hrs – Is this mother’s first pregnancy / H/O abortions? • She is a multigravida – Is the baby breast fed? • Started breastfeeding – What is the color of the stool? • Yellow

Scenario 2 • House officer makes a provisional diagnosis of: Pathological Jaundice – Serum total bilirubin – Mother and baby’s blood group – FBC, retics and peripheral film Continued

Scenario 2 Continued • Serum bilirubin 280 umol/l i. e. 15. 5 mg/dl (at 16 hrs of age) • • • FBC Hb 12. 3 g/dl TLC 18 x 103, retics 10% Baby’s blood group O + ve Mother O - ve Coomb’s test positive

Scenario 2 Continued

Scenario 2 Pathological Jaundice Secondary to Rh Incompatability
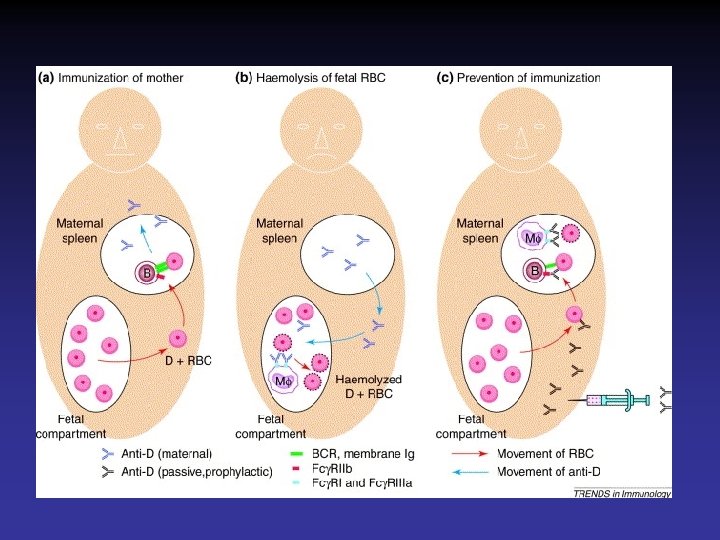

Pathological Jaundice • Appears within 24 hours of age • Serum bilirubin > threshold line

Scenario 3 A baby boy is born to a primigravida mother. He develops jaundice at 18 hrs of age. He is brought to you for evaluation and management.

Scenario 3 Continued • A house officer takes history and asks following questions. – When did the mother first notice jaundice? • Within 1 st 24 hrs – Is this mother’s first pregnancy / H/O abortions? • She is a primigravida – Is the baby breast fed? • Feeding poorly – What is the color of the stool? • Yellow

Scenario 3 Continued • House officer makes a provisional diagnosis of: Pathological Jaundice – Serum total bilirubin – Mother and baby’s blood group – FBC, retics and peripheral film
 • •")
Scenario 3 • Serum bilirubin 230 umol/l (at 20 hrs of age) • • • FBC Hb 12. 3 g/dl TLC 18 x 103, retics 10% Baby’s blood group O + ve Mother O + ve Coomb’s test negative Peripheral film spherocytes Continued

Scenario 3 Continued

Scenario 3 Pathological Jaundice Secondary to Hemolysis due to Hereditary spherocytosis

Scenario 4 A baby boy is born to a primigravida mother. He had a prolonged labor and was delivered secondary to ventouse application. After delivery he did not require any resuscitation but had a massive cephalhematoma on the head. He develops jaundice at 3 days of life. He is brought to you for evaluation and management.

Scenario 4 Continued • A house officer takes history and asks following questions. – When did the mother first notice jaundice? • After 1 st 24 hrs – Is this mother’s first pregnancy / H/O abortions? • She is a primigravida – Is the baby breast fed? • Feeding adequately – What is the color of the stool? • Yellow

Scenario 4 Continued • House officer makes a provisional diagnosis of: Physiological Jaundice – Serum total bilirubin – Mother and baby’s blood group – FBC, retics and peripheral film
 • •")
Scenario 4 • Serum bilirubin 350 umol/l (at 72 hrs of age) • • • FBC Hb 12. 3 g/dl TLC 18 x 103, retics 3% Baby’s blood group O + ve Mother O + ve Coomb’s test negative Peripheral film Normal Continued

Scenario 4 Continued

Scenario 4 Pathological Jaundice Secondary to Cephalhematoma

OTHER CAUSES OF UNCONJUGATED HYPERBILIRUBINEMIA Ø BREAST MILK JAUNDICE Ø DEFECTS OF CONJUGATION #Crigler Najjar Syndrome I & II #Gilbert Syndrome Ø METABOLIC DISORDERS #Glactosemia #Hypothyroidism Ø POLYCYTHEMIA

Kramer’s rule Clinically jaundiced when the bilirubin level reaches 80 -120 μmol/L

Why bother? n Deposition of unconjugated bilirubin in brain leads to BIND (bilirubin induced neurologic dysfunction) n Prevention of Acute bilirubin encephalopathy and Kernicterus

Treatment • Goals – Prevention of kernicterus – Maintenance of hydration and nutrition • Interventions – Intensive Phototherapy – Exchange transfusion

Phototherapy • Mechanism of action – Skin exposure to lights causing geometric photoisomerization allowing excretion • Technique – Light source • Lamps, spotlights, fiber optic blankets, • Blue light • Wave length: 420 -500 nm – Positioned 50 cm above infant – Largest surface area possible exposed




Complications of Phototherapy • Dehydration – Increased insensible water loss – loose stools • Irritability or lethargy • Skin rashes • Overheating • Retinal injury


Exchange Transfusion

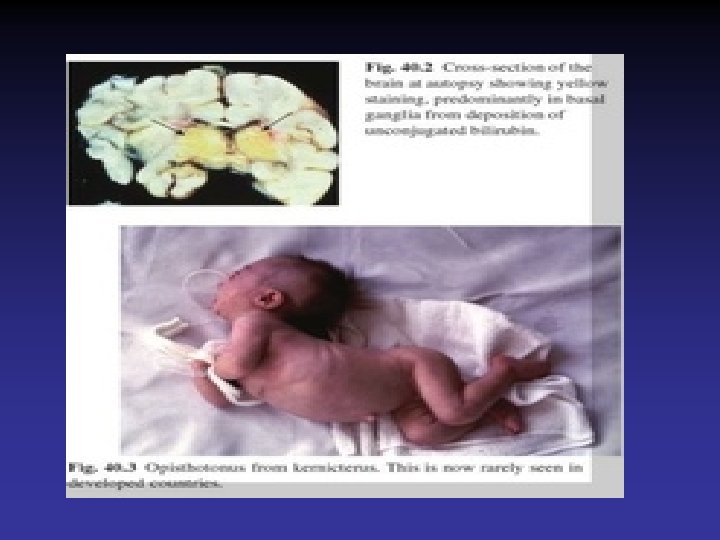
Bilirubin Encephalopathy • Deposition of unconjugated bilirubin in the basal ganglia and brainstem nuclei causing neurotoxic effects • Acute manifestations are lethargy & poor feeding • Severe cases, irritability, increased muscle tone opisthotonos, seizures and coma • Survivors may develop choreoathetoid cerebral palsy (due to damage to the basal ganglia), learning difficulties and sensorineural deafness

Summary • Neonatal jaundice is a fairly common condition • Keep a vigilant eye • Try to differentiate physiological from pathological jaundice • Early and effective phototherapy • Prevent BIND


- Slides: 56