Neonatal GI Problems 2 The Surgical Abdomen Abdominal

Neonatal GI Problems 2: The “Surgical Abdomen” Abdominal Wall, NEC, CDH and some cases CHO NICU Lecture PJ, AD, DD Revised 06/29/11

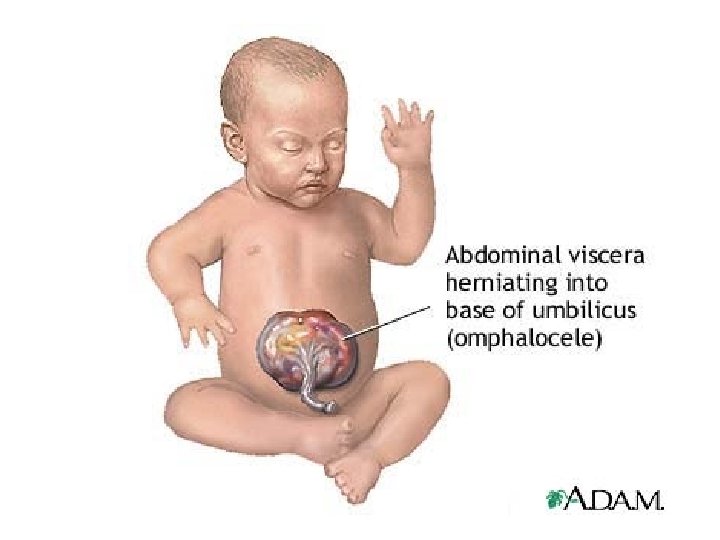
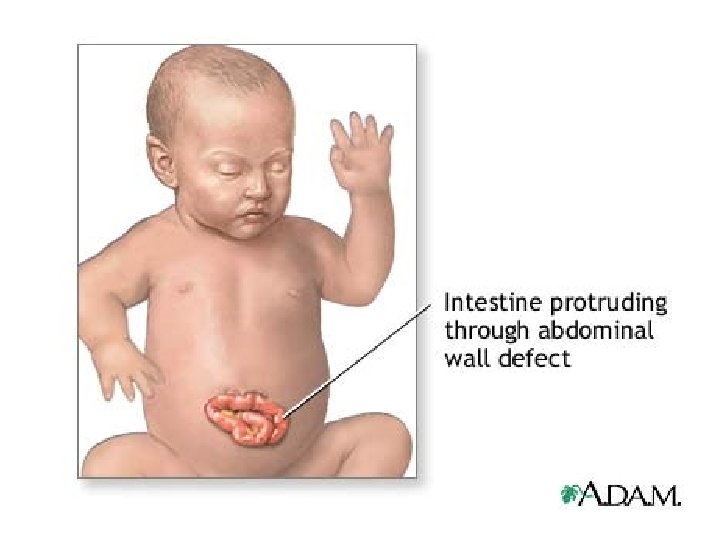
Abdominal Wall Defects

Abdominal wall defects Omphalocele Covering sac with cord 10 -20% premature Other major anomalies cardiac, CNS, renal syndromes, trisomies malrotation Liver may be in sac Malabsorption Gastroschisis No sac, cord to the side 50% premature, SGA common Occasional minor anomalies intestinal atresias Liver never out Malabsorption, prolonged ileus



Abdominal Wall Defects Management • Cover the defect: sterile non-latex gloves, turkey bag, plastic wrap, sterile saline soaked gauze • Vascular access: IV, arterial line • D 5/D 10 1/2 NS 120 -150 ml/kg/day • NG/OG drainage • Volume expander, blood pressure support • Respiratory support: lung hypoplasia is common • Blood culture, antibiotics (ampicillin, gentamicin)

NEC

Necrotizing Enterocolitis Management NPO, OG/NG to low intermittent suction Vascular access, IV and arterial Volume, pressors to support blood pressure Blood culture, antibiotics: ampicillin, gentamicin, clindamycin Respiratory compromise and apnea are common Blood products to correct coagulopathy, anemia, and thrombocytopenia • Serial abdominal x-rays (2 views), CBC, blood gasses • • •

CDH


Congenital Diaphragmatic Hernia: Pathophysiology • Pulmonary hypoplasia: affects both lungs – Pulmonary vascular hypoplasia • Pulmonary artery hypertension • Associated anomalies: cardiac, limb, and syndromes • Tracheobronchial anomalies

Congenital Diaphragmatic Hernia: Delivery Room Management • Place orogastric tube • Limit bag/mask ventilation • Early intubation of infants with respiratory distress • Consider administration of surfactant • Limit peak pressures to < 25 cm H 2 O • Avoid overventilation and overdistention

Congenital Diaphragmatic Hernia: Initial management • • • Vascular access Accept p. CO 2 in the 40’s - 60’s Cardiovascular support: volume, pressors Look carefully for other anomalies Echocardiogram Head ultrasound

Congenital Diaphragmatic Hernia: Respiratory Management • • • Permissive hypercapnea (PCO 2 50 s-60 s) Spontaneous respiration vs. paralysis High frequency oscillation Avoid overdistention and pneumothorax Surfactant

Congenital Diaphragmatic Hernia: Management of Pulmonary Hypertension • Previous therapies: intentional hyperoxia and hyperventilation, Na. HCO 3 infusion – Don’t do this!!!! • Maintenance of systemic blood pressure • Nitric oxide – No benefit in a large randomized prospective trial in neonates with diaphragmatic hernia – May have some short term benefits

Real Cases…. .

Case 1 Labor & Delivery • • • 570 g, 23 5/7 wks, born 8/27/09 Uncomplicated prenatal course until ROM 8/23 Betamethasone, antibiotics Transferred to Doctors Hospital Vaginal delivery, Apgars 1/5 Intubated, Surfactant in DR Anna Bergquist CHO MR 960776

Case 1 Early Course • • • HA and trophic feeds started day 1 Extubated day 4 PDA Rx’d with 2 courses Indomethacin NUS showed bilat GMH Blood cultures negative ETT culture positive for Ureaplasma Anna Bergquist CHO MR 960776

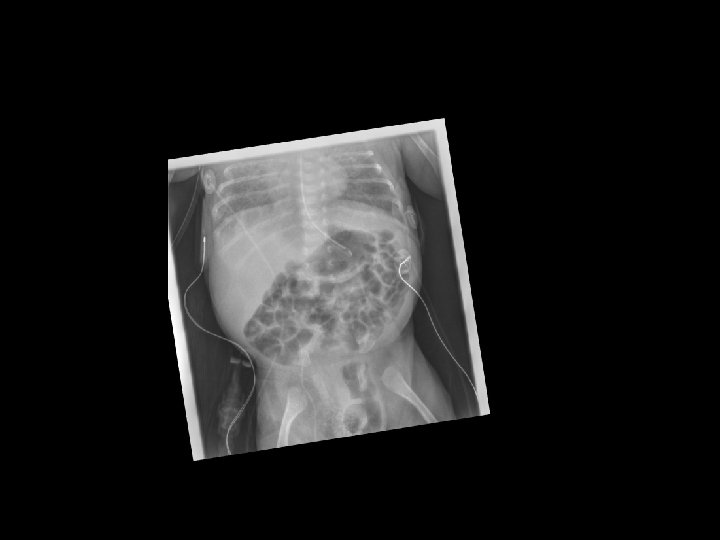
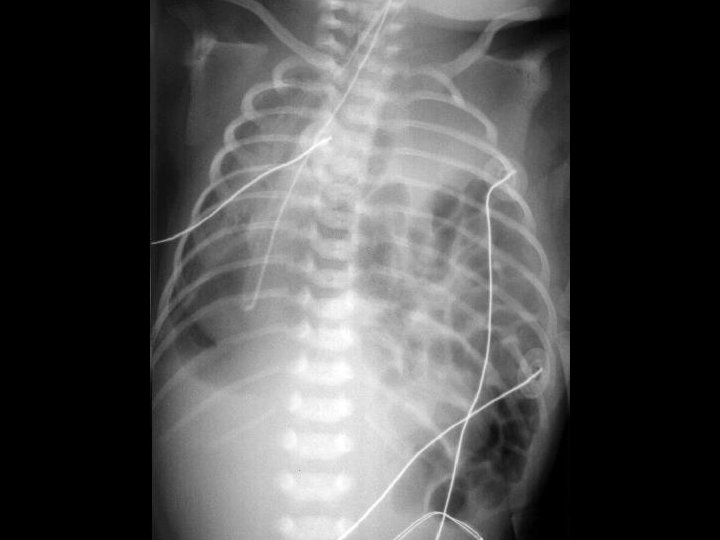
Case 1 Day 12 • On day 12 an Xray was done……


Case 1 Isolated GI Perforation • Not the same as NEC • Increased incidence with: – Low gestational age – Hydrocortisone – Combined Indomethacin & Hydrocortisone – Isolated Indomethacin not a risk factor (? ) • Symptoms secondary to peritonitis • Heals spontaneously – Risk for strictures

Case 2 Labor & Delivery • • • 530 g, 23 3/7 wks, born 7/29 Pre-term labor at 21 wks Betamethasone, antibiotics Cesarean for breech Apgars 2/3/10 Intubated in DR Jose Chavez CHO MR 960117

Case 2 Early Course • • • HA and trophic feeds started day 1 Prophylactic Indomethacin Failed initial attempt at extubation Blood cultures negative Echo on day 12 showed PDA – Started Indomethacin – Hypotension Rx’d with dopamine, hydrocortisone – Indomethacin D/C’d because of hypotension • Pulmonary hemorrhage, HFOV on day 13 Jose Chavez CHO MR 960117

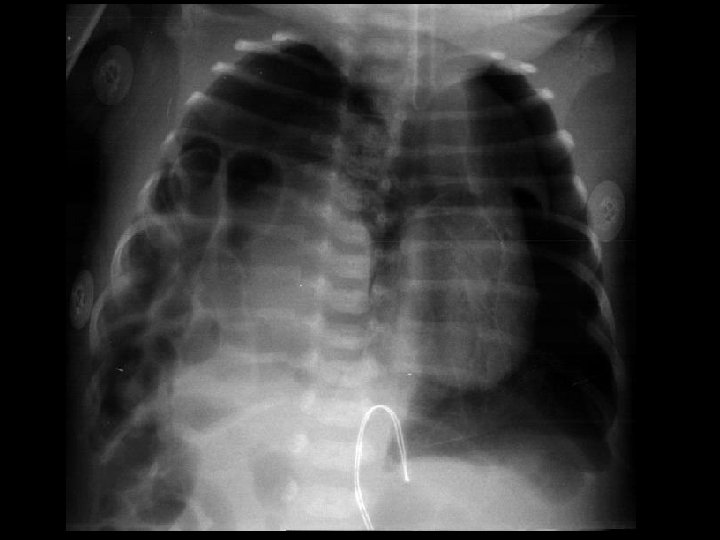
Case 2 Early Course • Trophic feeds re-started d 14 – Stopped on d 17 for abdominal distension – Prominent bowel loops, no pneumatosis – NPO for 7 days • Feeds re-started around d 21 • NPO again on 8/29 (d 30) for abdominal distension Jose Chavez CHO MR 960117
 for PDA ligation")
Case 2 Transfer • • • Transferred on 8/30 (1 month) for PDA ligation 800 g, systolic murmur, abdomen distended but soft NPO on HA PC/PS 17, PEEP 8, Rate 50 Multiple meds: – – – – Albuterol Pulmicort Caffeine Lasix Fluconazole Vancomycin Phenobarbitol Ativan Jose Chavez CHO MR 960117


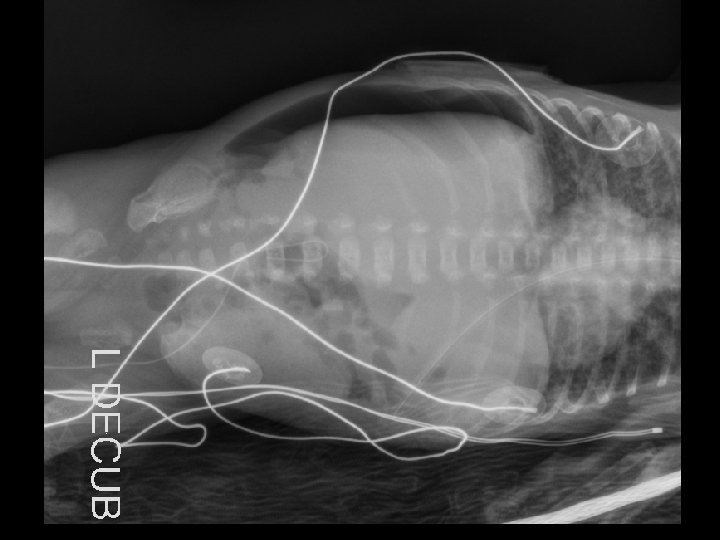
Case 2 Radiology Evaluation • Upper GI – Flow through normal duodenum, duodenal-jejunal junction, jejunum • Contrast enema – Microcolon – Distended RUQ loops do not fill during enema • Small bowel follow-through – Opacification of distended loops Jose Chavez CHO MR 960117
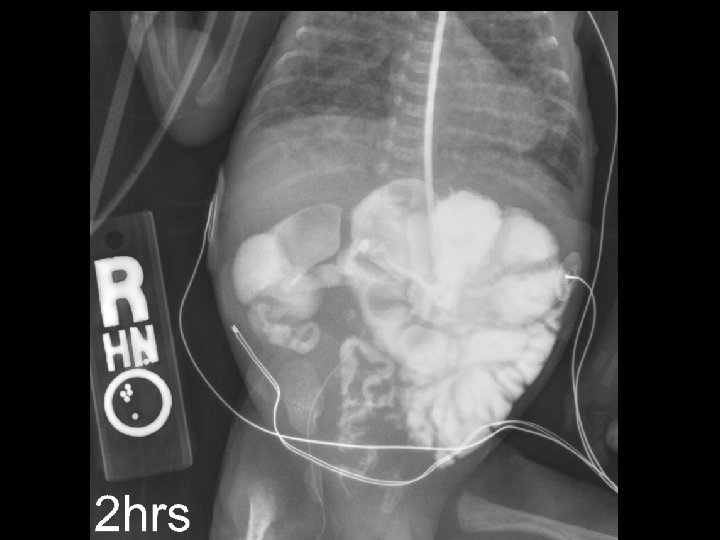

Case 2 Radiology Diagnosis • Microcolon • Dilated ileum secondary to obstruction • Differential diagnosis: – Stricture – Adhesions – Meconium Ileus Jose Chavez CHO MR 960117

Case 2 Surgery • Exploratory laparotomy • Extensive lysis of adhesions • Resection of 11 cm of distal ileum secondary to a concealed perforation • Creation of a double-barrel ileostomy Jose Chavez CHO MR 960117

Case 2 Findings at Surgery “Most of the small bowel in the proximal part of the jejunum all the way to the distal jejunum was quite small, and so was the ascending, descending colon. The distal small bowel appeared very distended and there was a lot of adhesions in the right lower quadrant involving several loops of distal ileum. It was apparent that there was a concealed perforation involving a segment of the distal ileum causing a significant amount of inflammatory changes and adhesions, which is causing the bowel obstruction. ” Jose Chavez CHO MR 960117

Case 2 What Caused the Adhesions? • Isolated perforation? • NEC leading to intestinal perforation? • Obstruction leading to perforation? – – • • Atresia Stenosis Web Volvulus Hirschprungs? Meconium ileus? Microcolon? In-utero perforation? Jose Chavez CHO MR 960117


Vomiting Surgical vs Medical • • • Pyloric stenosis Bowel atresia Malrotation with volvulus NEC Hirschsprungs disease Meconium ileus/plug Intussuception Incarcerated inguinal hernia Imperforate anus Stricture • • • Inborn errors of metabolism Gastroesophageal reflux Gastroenteritis Pyelonephritis Sepsis/meningitis Intracranial pathology

Final Thoughts • Normal abdominal Xray is: – Multiple, irregular, overlapping polygons • Bilious emesis is bad: – Malrotation can occur with normal XR – Volvulus is an emergency • Unexplained distension requires contrast studies: – Pediatric radiologist – Pediatric surgeon

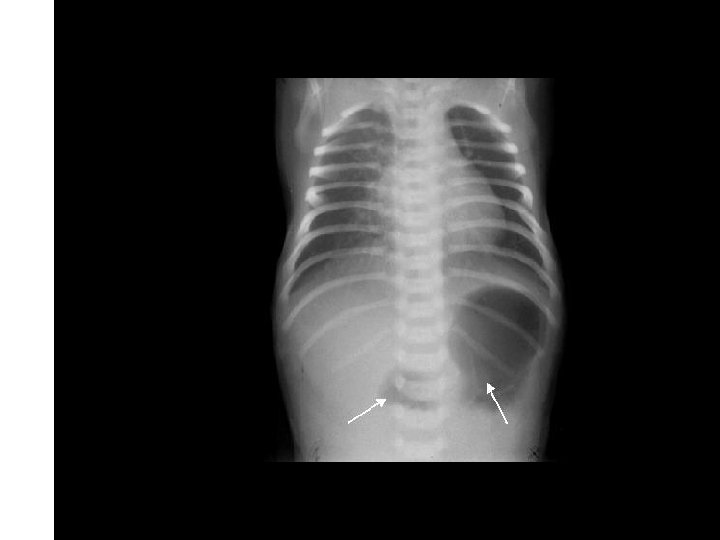
Case 1 Oh, oh…. . • On day 12…. – Free air noted on abdominal XR – No clinical abdominal symptoms • Rx…. – Intubated for transport – NPO – Antibiotic coverage expanded – Transported to Oakland Anna Bergquist CHO MR 960776
")
Case 1 Admission to Children’s Weight 560 g HR 157, BP 49/24 (mean 34) Grade 1/6 murmur, good pulses and perfusion Lungs unremarkable Abdomen “…full but not tense and does not appear tender. ” • Comfortable, vigorous, responsive • • • Anna Bergquist CHO MR 960776

Case 1 “Mini Laparotomy” “… a right lower quadrant incision was made. The peritoneum was entered. Purulent fluid presented, which was cultured. A small feeding tube was placed gently in the abdomen and the abdomen was irrigated with warm saline in all 4 quadrants. A little more purulent fluid came from the pelvis. An 1/8 -inch Penrose drain was then positioned through the opening down toward the pelvis and secured to the skin using a 5 -0 PDS suture. A stoma bag was placed over the drain. ” Anna Bergquist CHO MR 960776

Case 2 Post-op Course • • EEG for “jerking” normal NUS showed GMH, subsequently resolved • PDA ligation 9/25 (2 months) • Feeds started 9/29 – Distal re-feeding of ostomy output – Advanced to full feeds by 10/18 • Extubated 10/10 – Room Air 11/5 • Ostomy takedown 11/19 (4 months) – “Extensive lysis of adhesions” – Feeds re-started 11/29 – Adavanced to full feeds by 12/4 Jose Chavez CHO MR 960117
 Weight 2. 96")
Case 2 Discharge • • • Home Dec 24 (5 months) Weight 2. 96 kg Ad lib Enfacare 24 Multivitamins Room Air • Stage 3 ROP Jose Chavez CHO MR 960117


- Slides: 51