Neonatal GI Problems 1 The Surgical Abdomen Obstruction

Neonatal GI Problems 1: The “Surgical Abdomen” Obstruction CHO NICU Lecture PJ, AD, DD Revised 06/29/11

Causes of GI Obstruction Upper Tract �Esophageal atresia +/- tracheoesophageal atresia �Gastric causes: antral web, bezoar �Pyloric stenosis �Duodenal �atresia/stenosis, �annular pancreas �duodenal web �Malrotation �volvulus

Causes of GI Obstruction Mid-Gut �Jejunal atresia �Ileal atresia �Meconium ileus (associated with cystic fibrosis) �Small bowel perforation �NEC �Adhesions, strictures �Intussusception �Appendicitis �Abdominal wall defects � Omphalocele � Gastroschisis

Causes of GI Obstruction Distal Gut �Colonic atresia/stenosis �Hirschsprung’s disease �Meconium plug syndrome (associated with Hirschsprungs) �Small left colon syndrome (IDM) �Incarcerated inguinal hernia �Imperforate anus

Non-Surgical Causes of Ileus �Sepsis �UTI �Electrolyte abnormalities: �Hypokalemia �Hypermagnesemia �Drugs: morphine
 �")
Intestinal Obstruction �Symptoms and findings might include: � Abdominal distention � Emesis (bilious) � Tenderness � Visible loops of bowel, abdominal wall erythema �Associated problems: � Respiratory compromise, apnea � Hypovolemia, hypotension � Sepsis (NEC, perforation) � Electrolyte imbalance � Neutropenia (sepsis) � Thrombocytopenia (sepsis, perforation, bowel necrosis) � Check for incarcerated inguinal hernia, imperforate anus

Treatment of Intestinal Obstruction �NG/OG to low intermittent suction �Correct hypovolemia and hypotension � Third spacing into the lumen of the distended bowel �IV Fluids D 5/D 10 with 1/2 NS at 120 -150 m. L/kg/day �Correct electrolyte abnormalities and acidosis �Blood culture and Antibiotics � Ampicillin, Gentamicin, Flagyl (sometimes) �Respiratory support for abdominal distension or apnea

TEF/EA



Tracheo-esophageal fistula and esophageal atresia

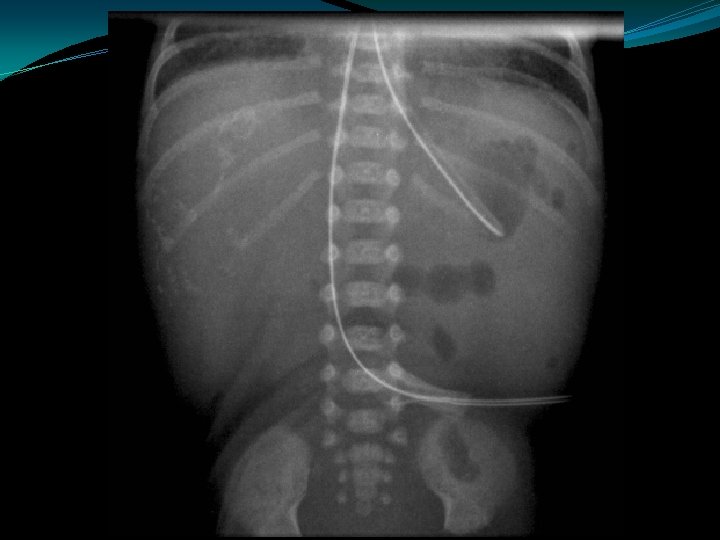
Esophageal Atresia & Tracheo-esophageal Fistula Symptoms �Respiratory distress from aspiration �Poor handling of secretions: drooling, frequent suctioning, choking or other symptoms with feeding �Inability to pass OG/NG to stomach �Abdominal distention may occur with swallowing of air through TEF or due to associated anal atresia

Esophageal Atresia & Tracheoesophageal Fistula Associated Problems �Prematurity �RDS, pulmonary aspiration �VACTERL (vertebral anomalies, anal atresia, cardiac anomalies, TEF, renal, limb) �Abdominal distention due to air passed through TEF can cause gastric perforation

Esophageal Atresia & Tracheoesophageal Fistula: Management �CXR with tube to the pharyngeal pouch �LIS to the pharyngeal tube �Blood culture, ampicillin and gentamicin �Manage respiratory problems �Examine for anomalies: VACTERL

Bilious Vomiting � 40% of babies with bilious vomiting require surgical intervention �Bilious vomiting in the neonate is due to mechanical obstruction until proven otherwise

Malrotation � 1/5000 live births � 80% occur during 1 st month of life �most during the 1 st week of life �Higher incidence in males (2: 1) �Normal exam early during course �Sx of obstruction: �Bilious vomiting �Sx of bowel ischemia: �Bloody stool, abdominal distension, tenderness, shock

Normal fixation of mesentary

Malrotation with Obstruction �Failure of fixation and rotation of midgut, small bowel, right colon, and transverse colon �Duodenal obstruction from Ladd’s bands

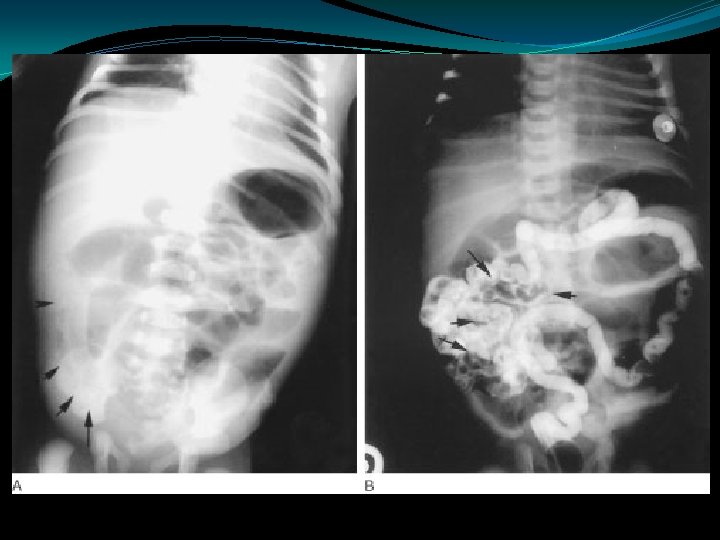
Malrotation with Volvulus �Small bowel twists around superior mesenteric artery, causing ischemia

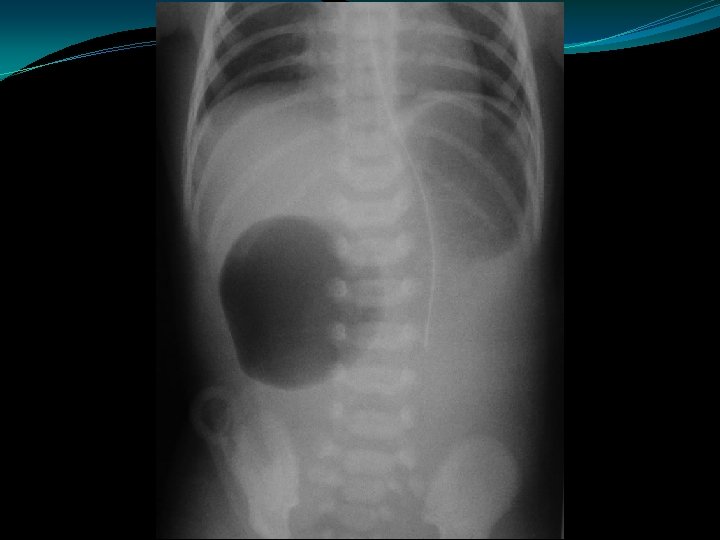
Malrotation/Volvulus Abdominal XRay �Normal film -20% �Dilated duodenal bulb and paucity of distal bowel gas �Double bubble sign �Distal gas filled bowel loops; gas filled volvulus (obstructed mesenteric veins prevent absorption of gas



Duodenal Atresia �Polyhydramnios �Partial obstructions: duodenal web, duodenal stenosis, annular pancreas � 40% of cases associated with trisomy 21 �Most common gut atresia in neonates �“Double bubble”


Hirschsprung’s Disease �Failure to pass meconium in 1 st 24 hrs �Absence of ganglion cells in mesenteric plexus �Most commonly rectosigmoid junction � 10% of cases involve entire colon � 10% of cases associated with Trisomy 21



Hirschsprung’s Disease �Contrast enema �Suction biopsy �Open biopsy �Rectal irrigation �Colostomy vs primary pull-through

In Utero Perforation �Caused by obstruction: �Meconium Ileus �Hirschprungs �Volvulus �Early perforation leads to Ca++ deposits �Later perforation may cause ascites, no Ca++ �Adhesions lead to obstruction

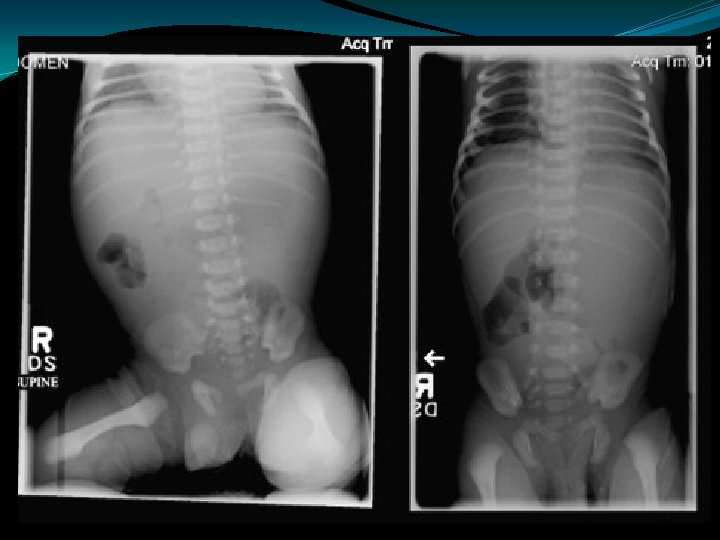
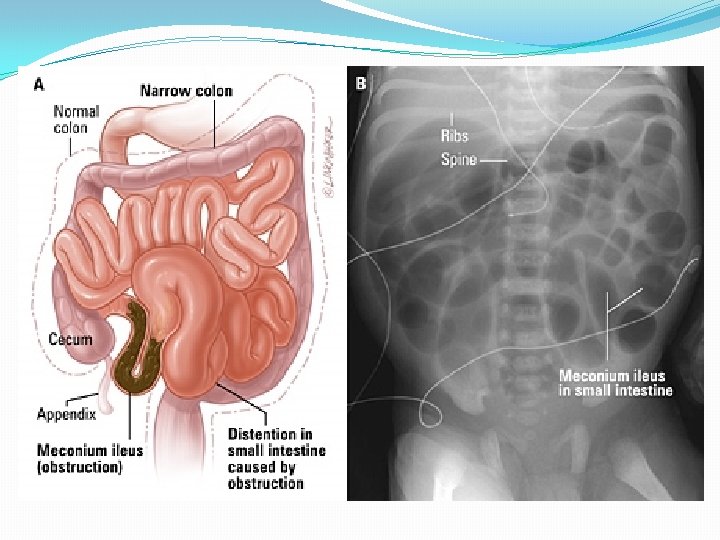
Meconium Ileus �Usually a manifestation of cystic fibrosis � 20% of infants with CF present with mec ileus �Obstruction of proximal ileum by thick, sticky round meconium pellets �Absence of air fluid levels �“soap bubbles” �Complications: �perforation, peritonitis, pseudocyst, ileal atresia/stenosis

Meconium Ileus �Contrast enema: �Small colon �Filled with pellet-like meconium when contrast extends to IC valve �Contrast can wash out the obstructing plugs and meconium plugs �The diagnosis of CF should be ruled-out


Meconium Plug Syndrome �Diagnosis of exclusion �Probably same as "small left colon" syndrome �Transient disorder due to functional immaturity of colon �Common in IDM, premies, PIH, Mg Rx �Infants with CF may present with mec plugs, although mec ileus most common � 10 -30% may have Hirschsprungs also

Meconium Plug Syndrome �Present within the first 24 to 36 hours of age: �Abdominal distention �Vomiting (bilious) �Failure to pass meconium �Plain films show distal intestinal obstruction �Contrast enema usually shows: �distention of the right and transverse colon �transition near the splenic flexure to a narrow descending colon and rectosigmoid region �Meconium within the colon �Main differential diagnosis is Hirschsprung's disease: �In Hirschsprung's disease, aganglionic colon is usually normal caliber �In Meconium Plug Syndrome, colon is usually small


- Slides: 41