Necrotizing Fasciitis Melissa Bauer Alicia Bellefeuille Naomi Burnett

Necrotizing Fasciitis Melissa Bauer, Alicia Bellefeuille, Naomi Burnett, Courtney Cashman, Tomas Cibak, Adam Cooling, Abby Zweifel

Etiology Type 1 ○ ○ ○ Mixed infection from aerobic & anaerobic bacteria ■ e. g. , Staphylococcus aureus, E. coli, Clostridium and Bacteroides species Infecting organisms usually introduced at sites of surgery or trauma Lesion usually found in perineal and abdominal areas Type 2 ○ ○ Caused by group A beta-hemolytic streptococci, possibly with a co-infection by S aureus Primarily affects the extremities Type 3 ○ ○ Associated with Vibrio vulnificus Enters subcutaneous tissues via puncture wounds from fish or marine insects

Pathophysiology ● Bacteria infiltrates the subcutaneous layer ○ ○ Directly from breaks in the skin Indirectly from distant sites of infection ● Pathogens proliferate in subcutaneous tissue at rapid pace ○ Invades and blocks blood vessels and lymphatic system —> causing vasoconstriction and thrombosis ● Decreased blood flow produces hypoxic conditions ○ ○ ○ Neutrophil function is hindered Delivery of antibiotics is impaired Type III pathogens work anaerobically, promoting further proliferation ● Necrosis of skin, fascia, and muscle result

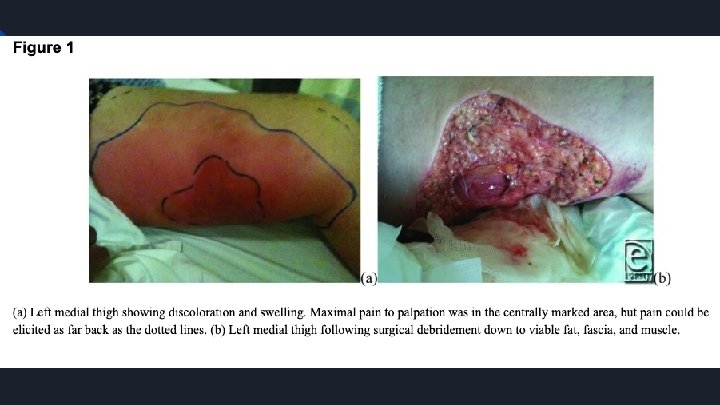
Signs and Symptoms ● Initially present with local symptoms of swelling, erythema, warmth, and tenderness ● Often present with disproportionate pain before cutaneous symptoms ● Vital Signs: tachycardia, fever, hypotension, and tachypnea ● As necrosis sets in, skin turns from red to purple/black or gray/blue ● Blisters and bullae form containing foul-smelling serous and hemorrhagic fluid ● Gaseous bubbles produced by anaerobic strains cause crepitus under the skin ● Advanced progression of the infection can lead to septic shock and multiple organ failure

Effects on Wound Healing ● Necrotizing Fasciitis is a medical emergency that must be treated promptly ● Necrosis of soft tissue can progress as quickly as 1 inch an hour ● Over 1 in 4 of those infected die of NF

Populations ~700 -1200 cases in the US every year since 2010 Anyone has the potential to develop necrotizing fasciitis, but people who are immunocompromised are more largely susceptible.

Risk Factors ● ● ● ● ● Heavy consumption of alcohol or drugs Diabetes Older adults Malnutrition Chronic or severe ill health Peripheral vascular disease Surgery or experienced trauma Obesity Women in childbirth Opportunities for infection: acne, eczema, punctures from pinpricks/insect bites/tattoos, dental treatment, mandibular fracture

Medical Treatments: Prompt Treatment is Key! ● Rapid antibiotic treatment, and prompt surgery are important to stopping this infection. ○ ○ Sometimes antibiotics cannot reach all of the infected areas, because the bacteria have killed too much tissue and reduced blood flow. When this happens, doctors have to surgically remove the dead tissue. Often treated in Burn Centers in a hospital. ● First Line Treatment: Intravenous antibiotic therapy. ○ Intravenous immunoglobulin: Supports the body's ability to fight infection.

Treatments Cont. Wound Care: Surgical debridement to remove damaged or dead tissue in order to stop the spread of infection. ○ ○ ○ Amputations of affected limbs, in some cases. Cardiac monitoring and breathing aids. Blood transfusions and medications to raise blood pressure. Other: ○ Hyperbaric oxygen therapy may be recommended to preserve healthy tissue by supplying oxygen to muscles.

PT Treatment for Wounds & Whole Patient ● ● Recognize signs and symptoms of NF Negative pressure wound therapy Universal precautions (hand washing) Wound debridement —> follow up with wet-to-dry dressings or “packing” ● Encourage mobility ● Increase ROM of extremities ● ADL’s —> promote circulation and tissue perfusion

Prognosis and Severity ● Rapidly spreading, potentially life threatening infection of soft tissues ● Need for several repeated surgical debridements ● Defects are reconstructed with plastic surgery and/or skin grafts ● High mortality rate estimated at 25 -35% ○ Estimated that 26% of cases experience limb loss

Other Considerations when treating Early symptoms evident within 24 hours include: ● ● Increasing pain in the general area of a minor cut, abrasion, or other skin opening Redness and warmth around the wound Flu-like symptoms (diarrhea, nausea, fever, confusion, dizziness, general malaise) Pain that is disproportionate to the injury Necrotizing Fasciitis can be difficult to differentiate from cellulitis ● Blister or bullae formation is important in the differential diagnosis of NF due to being rare in cellulitis Necrotizing Fasciitis is usually NOT contagious ● Transmission can occur through direct contact but requires a skin break (cut or abrasion)

References https: //www. cdc. gov/groupastrep/diseases-hcp/necrotizing-fasciitis. html https: //www. medicalnewstoday. com/articles/7884. php https: //www. webmd. com/skin-problems-and-treatments/necrotizing-fasciitis-flesh-eatingbacteria Misiakos EP, Bagias G, Patapis P, Sotiropoulos D, Kanavidis P, Machairas A. Current concepts in the management of necrotizing fasciitis. Front Surg. 2014; 1: 36. Published 2014 Sep 29. doi: 10. 3389/fsurg. 2014. 00036 Salcido R, Erdman W. Necrotizing Fasciitis: Reviewing the Causes and Treatment Strategies. Adv Skin Wound Care 2007; 20: 288 -93.
- Slides: 14