Necrotizing Enterocolitis AKA NEC By Amy Scheer NNPBC

Necrotizing Enterocolitis AKA: NEC By Amy Scheer, NNP-BC

Objectives What is NEC? Epidemiology/Incidence Signs and symptoms Diagnosis/Staging Management Medical Surgical Outcome Case study

What is Necrotizing Enterocolitis Disorder characterized by ischemic necrosis of the intestinal mucosa Associated with severe inflammation, invasion of enteric gas forming organisms and dissection of gas into the bowel wall and portal venous system

Epidemiolgy One of the most common gastrointestinal emergencies in the newborn infant Exact incidence of NEC unknown due to insufficient reliable data The majority (more than 90%) of cases occur in infants with birth weight <1500 grams and <32 gestational weeks The incidence of NEC decreases with increasing gestational age and birth weight

In the US the incidence of NEC is decreasing (over a 10 year period) Over the same time period the variation of NEC incidence has also narrowed amongst NICUs Mortality ranges from 15 -30% Inversely related to gestational age and birth weight 10% of NEC cases are Term infants Usually have a preexisting illness Congenital heart disease, primary gastrointestinal disorders, sepsis, fetal growth restriction, perinatal hypoxia

Signs and Symptoms Preterm Infant Generally healthy, feeding well & growing prior to diagnosis of NEC Sudden change in feeding tolerance Abdominal signs: tenderness, vomiting (can be bilious), diarrhea, rectal bleeding, distention Several non-specific signs: need for increased respiratory support, apnea, lethargy, temperature instability Potential for associated bacteremia (occurs in 20 -30% of the cases) Timing of Presentation (early onset v late onset)

Signs and Symptoms cont. Term Infants Bilious gastric aspirate or emesis Abdominal Rectal Distension bleeding Median onset of symptoms 7 -12 days
 20% of the")
Laboratory Findings Anemia Thrombocytopenia DIC: Disseminated intravascular coagulation (abnormal coagulation studies) 20% of the cases positive blood cultures

Abdominal Imaging X-rays are used to confirm diagnosis They don’t stand alone to diagnosis; need to look at clinical picture as well Not sensitive in extremely preterm infants
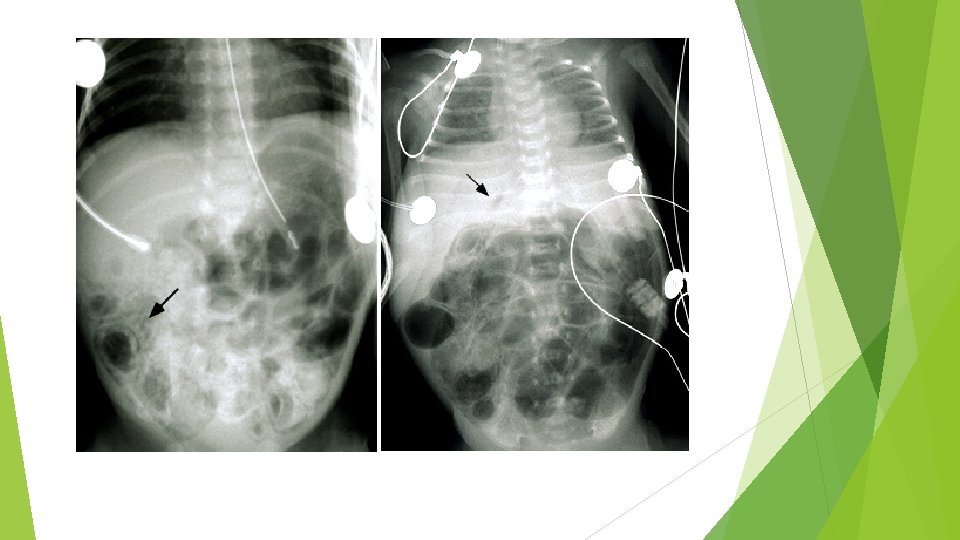
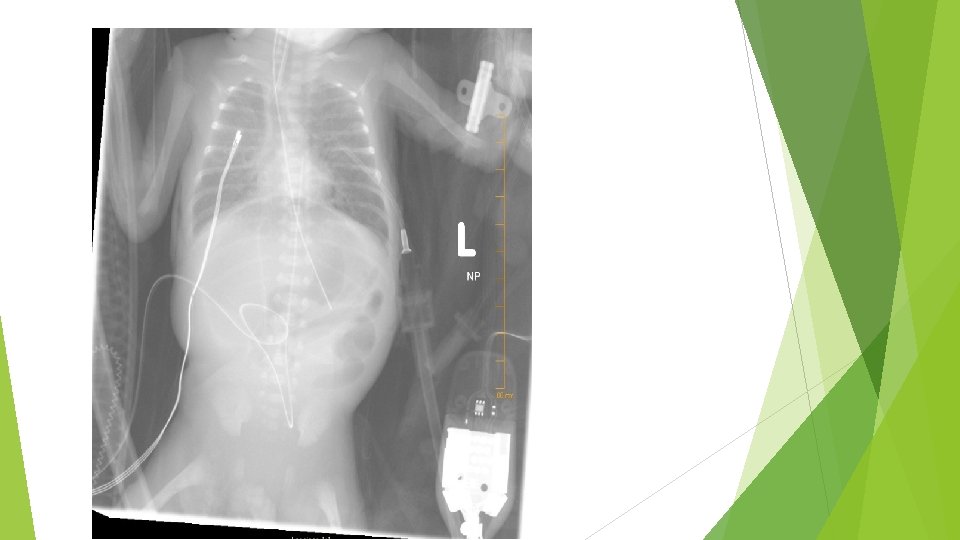
 Common radiographic findings Abnormal gas pattern (non specific) Pneumatosis Gas intestinalis")
Abdominal Imaging (cont) Common radiographic findings Abnormal gas pattern (non specific) Pneumatosis Gas intestinalis (considered a hallmark of NEC) bubbles in the intestinal wall Pneumoperitoneum May Fixed (bowel perforation) result in a football sign on supine radiography dilated loops of bowel


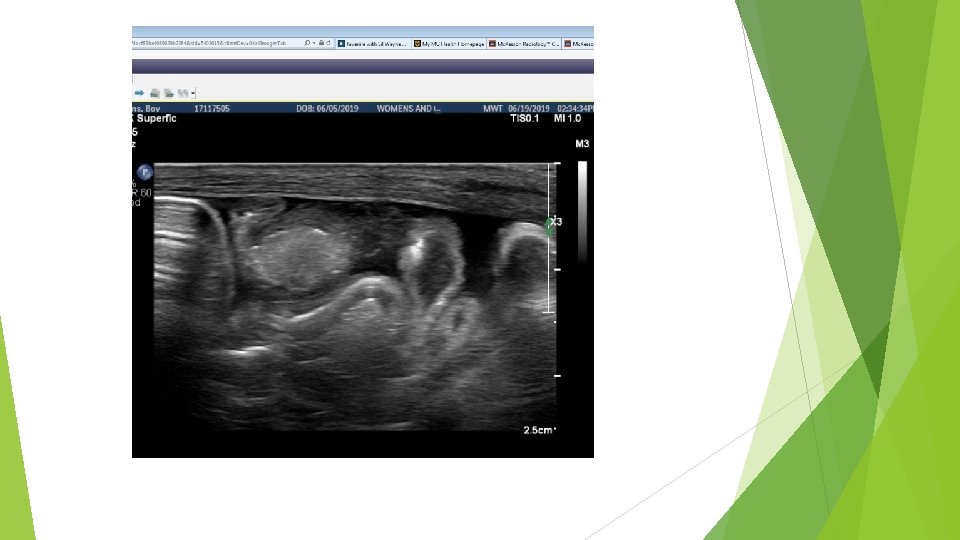
Abdominal Ultrasound Increasing helpful in diagnosis and management Real time visualization of bowel wall thickness, peristalsis and perfusion Findings: Presence of free air, focal fluid collections & increased bowel wall thickness Con: Limited by operator expertise Additional imaging training to read and understand
 Gastric decompression (salem sump to Low intermittent")
Management: Medical Supportive Care Bowel rest (NPO) Gastric decompression (salem sump to Low intermittent suctioning) TPN and lipids (central line placement): optimize nutrition to assist in healing Fluid replacement: due to third spacing or bowel inflammation causing capillary loss Respiratory support Cardiovascular support Hematologic and metabolic abnormalities
 Antibiotic therapy Obtain blood cultures prior to initiation Broad spectrum antibiotics:")
Management: Medical (cont) Antibiotic therapy Obtain blood cultures prior to initiation Broad spectrum antibiotics: Ampicillin, Gentamicin and Metronidazole May need to use Vancomycin (if MRSA or ampicillin resistant enterococcal infection suspected) 10 -14 days usually sufficient May need to use Fluconazole or amphotericin B if fungal infection suspected 20 -30%of NEC Cases also have documented bacteremia
 Monitoring Physical Examination Changes in vital signs Frequent Labs (CBC, coags,")
Management: Medical (cont) Monitoring Physical Examination Changes in vital signs Frequent Labs (CBC, coags, Blood gases, electrolytes) Abdominal imaging Initially every 6 hours Increased or decreased frequency based on clinical findings

Management: Surgical Only absolute indication for surgical intervention is PNEUMOPERITONEUM


 Primary Peritoneal Drain Performed at the bedside in the NICU Primary")
Management: Surgical (cont) Primary Peritoneal Drain Performed at the bedside in the NICU Primary purpose: Pressure relief with evacuation of air and stool contaminated ascites Local Anesthesia Mortality higher Drain site observed for several days Drain is removed Once bowel sounds return feeds are restarted slowly Contrast study may be performed
 Laparotomy Resection of the affected bowel segment Placement General Second of")
Management: Surgical (cont) Laparotomy Resection of the affected bowel segment Placement General Second of ileostomy and mucous fistula Anesthesia procedure for reanastomosis Usually 4 -6 weeks after initial procedure

Complications Acute complications Infectious: Sepsis, meningitis, peritonitis and abscess formation Disseminated Respiratory intravascular coagulation (DIC) and Cardiovascular Complications Hypotension, Metabolic shock, respiratory failure Complications Hypoglycemia and metabolic Acidosis
 Late Gastrointestinal Complications Stricture formation: 24% Usually occur in the Colon but")
Complications (cont) Late Gastrointestinal Complications Stricture formation: 24% Usually occur in the Colon but can occur in ileum and jejunum Multiple sites are common Develop 2 -3 months of the acute episode May develop bacterial overgrowth in the small bowel Repeated infections Bloody stools Failure to thrive
 Short-gut Less 9% syndrome than 25% of normal bowel length of infants")
Complications (cont) Short-gut Less 9% syndrome than 25% of normal bowel length of infants that have surgery for NEC Occurrence increases as gestational age decreases Chronic need for TPN Increases failure risk of Cholestasis and liver
 Risk of Short gut increased by Parental antibiotics on the day NEC")
Complications (cont) Risk of Short gut increased by Parental antibiotics on the day NEC is diagnosed Birth weight <750 g Mechanical ventilation on the day of diagnosis Exposure to enteral feeds prior to the diagnosis Diverting jejunostomy and duration of use (Duro, 2010)

Outcome Mortality: NEC accounts for approximately 10% of deaths in NICU infants Mortality increases with decreasing gestational age Approximately ½ of survivors: NO LONG TERM EFFECTS Other ½ of survivors: Gastrointestinal Growth Complications failure Impaired Neurodevelopmental outcomes

Case Study 30 4/7 gestational week infant Maternal information 20 year old G 1 Pregnancy complicated by severe Pre-eclampsia & fetal severe unilateral renal pyelectasis Prenatal labs: HBs. Ag, HIV, Gonorrhea/Chlamydia, GBBS: negative; Rubella immune and RPR non-reactive Betamethasone was given 1 week before delivery and mother was receiving Mg prior to delivery

Delivery History Infant was delivered via C-section due to severe pre. Eclampsia After 20 seconds of delayed cord clamping infant was brought to radiant warmer, placed in plastic bag on a port a warmer mattress Heart rate >100 bpm PPV at 1 minute of life due to respiratory insufficiency Transitioned to CPAP at 3 minutes of life At 10 minutes of life infant intubated due to worsening respiratory status Infant transported to the NICU in a pre-warmed isolette Birth weight: 1. 23 kg

Course History Respiratory: infant extubated at 1. 5 hours of life after Surfactant Reintubated for surgery due to SIP (spontaneous intestinal perforation on DOL 2 after 1 day of trophic feeds Surgery on DOL 2 with Penrose drain placed; Ileostomy placed on DOL 14 Several intubation and extubations until infant stable on noninvasive ventilation on DOL 18 Enteral feeds of Prolacta/Breastmilk restarted on DOL 14 with progression to full enteral feeds on DOL 20; Infant continued on CPAP at this time Medications: Caffeine, Amoxicillin (prophylaxis), Na. Citrate, Multivitamin with iron and Vitamin D
 DOL")
NEC Course DOL 36 -37: Infant developed watery stools with flecks (gradually improved) DOL 37: Infant had increased emesis and was later noted to be pale, mottled; abdomen was distended and “veiny” KUB: revealed distended bowel concerning for NEC Infant was made NPO and started on fluids; Infectious labwork was obtained; A sump to LIS was placed and started on Gentamicin, Vancomycin and Metronidazole Repeat KUB 6 hours later revealed pneumatosis without perforation Per ID recommendations and NEC diagnosis antibiotics changed to Cefepime

 DOL 40 No perforation noted antibiotics changed to Ampicillin and Gentamicin")
NEC Course (cont) DOL 40 No perforation noted antibiotics changed to Ampicillin and Gentamicin per ID 10 day course of Antibiotics completed on DOL 47 Enteral trophic feeds of unfortified Breast milk started on DOL 48 Refeed DOL 55 ostomy output through mucous fistula on
 Fistula gram showed easy passage of contrast throughout distal bowel to")
NEC course (cont) Fistula gram showed easy passage of contrast throughout distal bowel to rectum Reanastamosis Restarted Full on DOL 79 1/3 of enteral feeds on DOL 83 enteral feeds achieved on DOL 85 Transitioned Discharged to Ad lib demand on DOL 86 Home on DOL 92

References Duro D. Kalish LA, Johnson P, et al. risk factors for intestinal failure in infants with necrotizing enterocolitis: a Glaser Pediatric Research Network study. J Pediatr 2010; 157: 203 Kim, JH. Neonatal necrotizing enterocolitis: Management. Up to Date 2019 Kim, JH. Neonatal necrotizing enterocolitis: Clinical features and Diagnosis. Up to date 2019 Neu J, Walker WA. Necrotizing enterocolitis. N Engl J Med 2011; 364: 255.
- Slides: 37