Neck Pain Treatment of Cervical Spine Pain Benjamin

Neck Pain: Treatment of Cervical Spine Pain Benjamin Bonte, MD Interventional Pain Fellow Hudson Spine & Pain Medicine 10/11/2017

Cervical Spine Disorders • Anatomy • Cervical Spondylosis – Facet pain • Myofascial pain • Cervical radiculopathy • Cervical myelopathy • Modalities/other considerations

Anatomy • 7 cervical vertebrae – Atlas/axis, C 3 -7 • Extension – Occipital C 1 junction, C 1/C 2 • Lateral bending – C 3 -5 levels • Axial rotation – C 1 -2 level
 • Supraspinous")
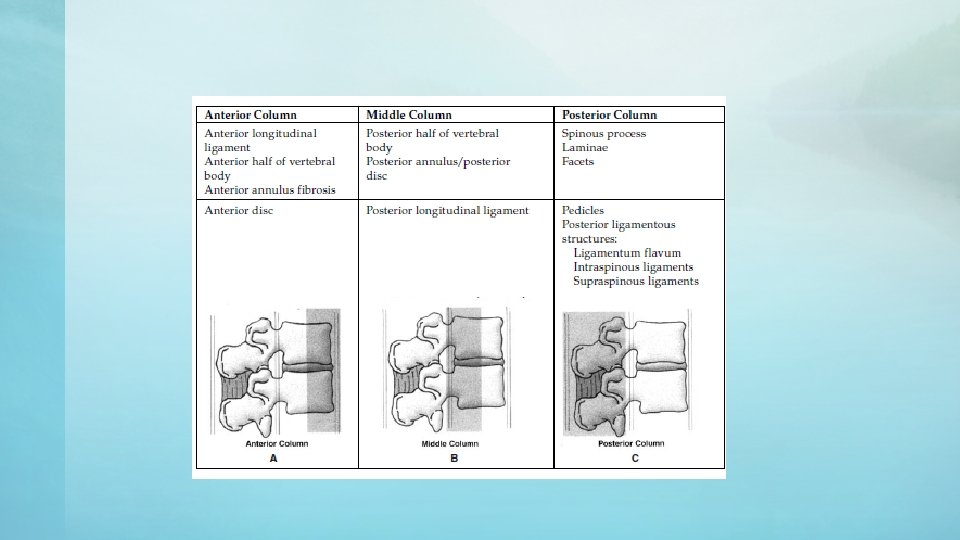
• ALL • PLL • Ligamentum Flavum • Interspinous ligament (midline) • Supraspinous ligament

• C 2/3 – Third occipital nerve • C 3 to T 1

Cervical Spondylosis • Characterized by disc height loss, endplate spurring, uncoverterbral joint hypertrophy, facet joint hypertrophy and ligamentum hypertrophy • Most common at C 5 -6 level

Facet joint pain • Pain related to synovial capsule nociceptors • Imaging may show facet hypertrophy, MRI with synovial capsule enlargement*

Medial Branch Blocks

Medial Branch Blocks • Targets at articular pillar • C 7 – apex of SAP • C 2/3 –multiple locations needed for blocking

Cervical RFA

Evidence? • Significant benefit over sham • Length to 50% return in pain? – 8 vs 263 d.
 • Spurling’s maneuver is most")
Cervical Radiculopathy • Hx, PE (reflexes, strength testing, sensation) • Spurling’s maneuver is most sensitive and specific test • Butler test (SLR of the upper limb) • Rule out imitators
")
Dynatomal maps (referred pain)

Cervical Radiculopathy • Foraminal stenosis due to facet hypertrophy or disc herniation. • MRI – axial view is more useful due to oblique angle of exit. • EMG – assists with localizing lesion

• C 7 -T 1 has largest epidural space relative to the dura and spinal cord. • Ligamentum flavum has lower failure to fuse rate a this level • Lateral view may be impossible due to shoulder • Contralateral oblique can be used to assess depth

Cervical TFESI • Bad publicity • Avoid particulate steroid inj into feeder vessels of VA or ASA (use dexamethasone) • Hit anterior SAP then walk off, stay posterior, inferior. • Digital subtraction angiography strongly advised

Evidence? • PT – Saal&Saal study – Observational trial – 24/26 patients with radiculopathy and neurologic loss who underwent nonsurgical treatment (sensation+) – 20/24 had good or excellent outcome. • Medications – NSAIDS – Oral steroids – Very little evidence for efficacy in cervical – Kaiser study shows good evidence in lumbar radiculopathyies for functional improvement but not in terms of pain.

Evidence? • ILESI and TFESI both have evidence for treating radiculopathy. • ILESI has RCTs to support this, whereas TFESI has descriptive studies. – Stav 1993 – Better pain reduction in ESI group than local anesthetic inj – Better outcomes at 1 year and 1 year. • Both ILESI and TFESI have limited evidence in treatment of axial neck pain.

Cervical Myofascial Pain • Can give referral patterns similar to facet joint referral patterns • X-ray may show straightening of cervical spine

Trigger points • Tender point that causes referred pain • Nelemans PJ, de Bie RA, de Vet HCW, et al: Injection therapy for subacute and chronic benign low-back pain (Cochrane review), Cochrane Database Syst Rev (2), 2000, CD 001824. – When targeting trigger points, Dry needling, lido + steroid all superior to placebo injections

Cervical Myelopathy • Insidious weakness, bowel/bladder changes • PE: test for Hoffman’s sign, spasticity, clonus, Babinski. • Risk factors: cervical stenosis - congenital, degenerative, HNP. • MRI is test of choice – assess for spinal fluid around cord. Torg ratio (diameter of canal to vertebral body) on XR is out of favor. Although sensitive, it has low predictive value for symptomatic cervical stenosis. • Laminectomy indicated for – Multilevel spondylotic myelopathy – Spondylotic myelopathy with congenital canal stenosis.

Stingers • Neurapraxia of the brachial plexus • usually after sport injury causing transient stretching. – Younger athletes – presents similar to brachial plexopathy, generally involving upper trunk/C 5 – Older athletes – may present similar to nerve root impingment • Generally self-resolves

Special Considerations • Cervical Manipulation – Stroke associated with VA dissection – 275 cases in literature since 1925 – No reliable risk factor to identify those at risk from spine manipulation – Risk for VA dissection in general: Migraine, hypertension, OCP, smoking – Lack of ROM testing prior, and use of high-amplitude, high-velocity, high force thrust associated with all accidents in a German study

Special Considerations • Cervical Traction – Head in 20 -30 degrees of flexion, 25 lbs of force applied. – Some evidence that this can treat cervical radiculopathies. – Evidence does not support/efficacy is unknown for axial neck pain.

Special Considerations • Massage – Very difficult to study due to different techniques and lack of a standardized sham treatment. – At least one large RCT supports the use of massage in the treatment of – – – Anxiety/stress Arthritis Fibromyalgia Lymphedema Whiplash Sleep disorders – Contraindications – area of malignancy, cellulitis, trauma, bleeding, DVT/atherosclerotic plaques – Caution – anticoagulation/bleeding disorder, osteoporosis, low BP, hx physical abuse
- Slides: 27