National Immunization Conference Hilleman Lecture Achieving Global Immunization

National Immunization Conference Hilleman Lecture: Achieving Global Immunization for All: Can We Do the Right Thing? Stephen Cochi, MD, MPH Senior Advisor Global Immunization Division Centers for Disease Control and Prevention

Lofty Global Goals § > 90% coverage in every country and > 80% in every district Introduce new vaccines Achieve Polio Eradication § § § Reduce Measles Deaths by 90% by 2010 § Strengthen immunization systems

What is Possible? How Are We Doing? There is good news…. . and not so good news (i. e. , challenges!!)

Causes of 4. 1 million deaths in <5 yr olds (out of 10. 5 million total deaths) in 2002 Source: World Health Report 2004
 Source: WHO/IVB, Data as")
2. 5 million annual childhood deaths due to VPDs (2002) Source: WHO/IVB, Data as of 2002

Very modest reduction in annual childhood deaths from VPDs in 2002 -05* Source: WHO/IVB - *PROVISIONAL Data for 2005
 by year and WHO regions, 2000 -2005 33.")
Number of unvaccinated children (DTP 3) by year and WHO regions, 2000 -2005 33. 6 32. 4 32. 5 31. 0 29. 4 28. 2 China Indonesia India Pakistan Nigeria Source: WHO/UNICEF coverage estimates 1980 -2005, August 2006 Date of slide: 4 September 2006

Number of Unvaccinated Children by Year and WHO Region, 2000 -2005, Projected to 2010* 33. 6 32. 4 32. 5 31. 0 29. 4 28. 4 2010 goal: At least 90% coverage in all countries! 62%↓ ` Source: WHO/UNICEF coverage estimates 1980 -2005 10. 8

Global Immunization Vision A world in 2015 in which…. . § Immunization is highly valued § Every child, adolescent, and adult has access § More people are protected against more diseases § Vaccines are put to best use in improving health/security globally

Realizing the vision Four strategic areas - Reaching more people - Introducing new vaccines & technologies - Integrating with other interventions in health systems context - Global interdependence

Good News There is more funding for global immunization than ever before in history !!

Annual Costs of Immunization, 2000 -2015 +20% +40% +125 %

GAVI projected income through 2015 US$ millions Two projected scenarios, including IFFIm, excluding AMCs $800 High $700 $600 Low $500 $400 $300 $200 Source: GAVI Secretariat, Feb 2006 2015 2014 2013 2012 2011 2010 2009 2008 2007 2006 2005 2004 2003 $0 2002 $100
 HPV Rotavirus Pneumo (conj) Cholera")
The vaccines pipeline HIV/AIDS Future Malaria Dengue Mening (conj) HPV Rotavirus Pneumo (conj) Cholera Underutilized Vaccines Typhoid YF Influenza JE Rubella Hib (conj) Hep. B Measles Traditional EPI Tetanus Polio Pertussis Diphtheria // // 1960 1980 TB 2000

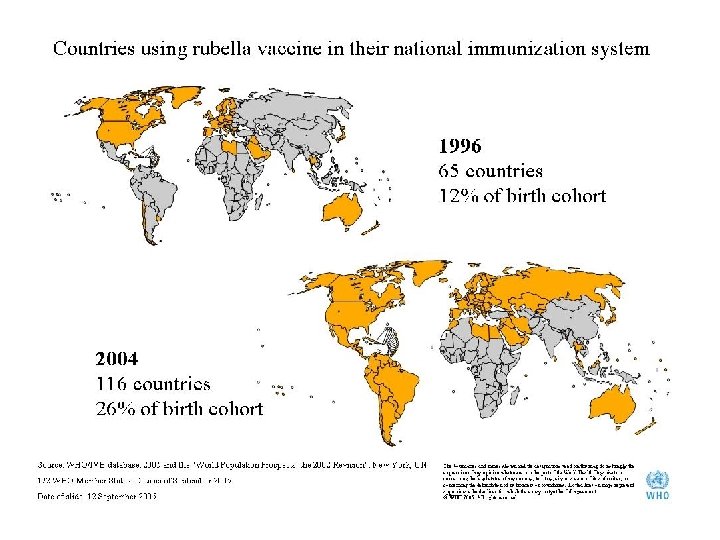
New and Underutilized Vaccines § § § Hepatitis B vaccine Hib vaccine Rubella vaccine Rotavirus vaccine Pneumococcal conjugate HPV vaccine

Hib Disease – The Global Burden ( WHO Estimates - Children < 5 years old) § 3 million children with serious illness/ year § > 400, 000 deaths/year (>1, 000 preventable deaths each day) § A leading cause of infectious death in children under 5 years of age

Despite availability of an effective and safe vaccine for over 15 years, and availability of GAVI support for 6 years, 75% of the world’s children still don’t have access to Hib vaccine

Countries using Hib vaccine in their national infant immunization system 1997 Hib vaccine introduced Hib vaccine not introduced 2006 Hib vaccine in routine immunization schedule (outside GAVI support) Hib vaccine introduced or approved for GAVI support Hib vaccine not introduced Source: WHO/IVB database, May 2006

Estimated global distribution of the 600, 000 annual deaths caused by rotavirus 1 dot = 1000 deaths

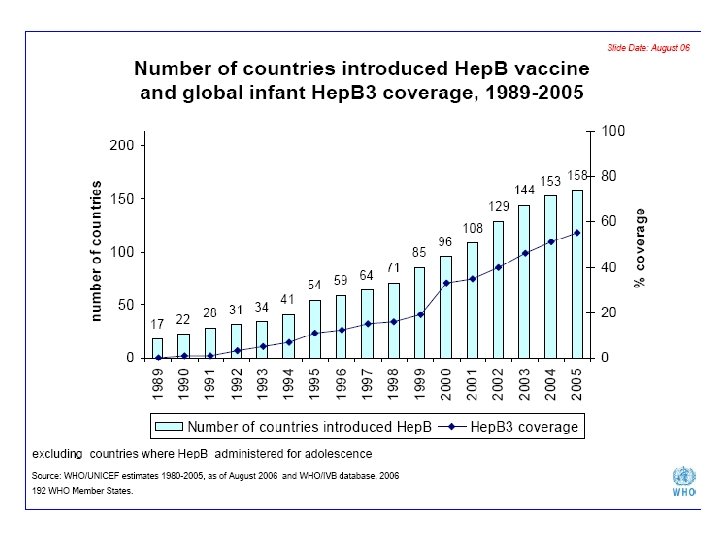
The Challenge: Avoid the time lag seen for hepatitis B and Hib vaccines Million doses 1 3 5 7 Hep. B -- all developing countries 9 11 13 15 17 19 21 23 Years from availability Hib -- all developing countries

Equity: Can we speed the time that vaccines get to children in greatest need?

The biggest challenge for live oral rotavirus vaccines today is whether they will work in the developing world !!
 3. 0 2.")
Leading infectious causes of mortality, 2000 estimates 3. 5 Deaths (millions) 3. 0 2. 5 2. 0 1. 5 < 5 yrs old > 5 years old 2. 7 2. 2 S. pneumoniae: ~1. 6 million deaths, 1. 7 including ~800, 000 child deaths* 1. 1 0. 9 1. 0 0. 5 0 Pneumonia AIDS Diarrhoea TB Source: WHO Malaria Measles *New estimates being made

Pneumococcal vaccine pipeline Development Stage Pre-clinical stage Clinical trial Phase III 9 -valent Multinational ~20 vaccines in research/ Pre-clinical stage (includes conjugate & protein-based vaccines) GSK 10 -valent Launched Prevnar (7 -valent) Expected launch 2008 11 -valent 7 -valent Emerging suppliers >5 mulit-valent conjugate vaccine projects Source: BCG Global Supply Strategy 2005 Pneumo. ADIP team analysis Wyeth 13 -valent Discontinued

HPV vaccine potential: Estimated numbers of new cancer cases and deaths in 2002 Cervical cancer is 2 nd most common cancer in women worldwide & 1 st cause of cancer-related deaths in women in developing countries Source: Parkin et al. , 2005, Global Cancer statistics 2002
 • Over 90% effective in preventing new")
The Potential of Human Papillomavirus Vaccines (HPV) • Over 90% effective in preventing new infections and precancerous cervical lesions caused by the HPV types that the vaccine covers * • The vaccine to be given before HPV infection is acquired (e. g. , 11 -12 year olds in US)* • Most needed in resource poor countries but initial price is unaffordable ($300)* • HPV will not eliminate need for screening, essential to detect cancers by other HPV types * BMJ, Editorial, 13 May 2006

Polio – the world in 1988 >350, 000 cases >125 polio-endemic countries 1988: World Health Assembly Voted to Eradicate Polio

Poliovirus spread, 2003 -2006 25 countries, 71 events Number of importations from India Viral origin: 13 (18%) Wild virus type 1 Wild virus type 3 Wild virus type 1 & 3 Endemic countries Case or outbreak following importation (last 6 months) Case or outbreak following importation (6 - 12 months) Number of importations from Nigeria viral origin: 58 (82%) Source: WHO, January 2007

Polio – the world at end-2006 1, 977 cases 4 endemic countries district with type 1 polio district with type 3 polio endemic areas

3 -Pronged Approach to Finish Polio Eradication § New Tools § New Standards to Reduce § International Spread New Approaches to Address Challenges in Last 4 Endemic Areas

New Polio Vaccines 2005 -2006 monovalent OPV types 1 & 3 (m. OPV 1 & m. OPV 3) 'monovalent' OPV protects 2 x greater New Trial Data, Egypt

New international standards for polio outbreak response FAST: start within 4 weeks VERY LARGE: 2 -5 million children. HIGH QUALITY: house-to-house. SUSTAINED: minimum 3 rounds. OPTIMAL VACCINE: m. OPV Adopted by the World Health Assembly, May 2006
 22 January 2007 'Standing Recommendation")
New Standards to Reduce Polio Exportations Executive Board (WHA) 22 January 2007 'Standing Recommendation under IHR (2005), requiring full OPV immunization of all travellers from infected areas' Saudi Arabia requires proof of OPV for entry visas.
 Strategy, Nigeria Fixed Sites: • 5 days • m.")
New 'Immunization Plus Days' (IPDs) Strategy, Nigeria Fixed Sites: • 5 days • m. OPV 1, measles, DPT • deworming meds, bednets, etc Mobile Teams (house-to-house): • 5 days • m. OPV 1, social mobilization.

Measles Building on Polio Eradication
 331 Prefecture Labs 15")
Global VPD Laboratory Network N=835 (Polio N=145 - Measles N=690) 331 Prefecture Labs 15 al on ati -N ub 4 S bs La Labs testing for: Polio and measles/rubella Measles/rubella only Measles/rubella and yellow fever Data as of Sept 2004 Polio, Measles/rubella and yellow fever

Major Global Measles Virus Transmission Pathways 2005 -06 Key B 2 B 3 D 4 D 6 D 8 H 1 D 6 D 4 H 1 D 4 D 8 B 3 B 2 Acknowledgement: Data provided by WHO Measles/Rubella Laboratory Network Transmission pathways with Epi links Suspected transmission pathways H 1

Strategy for sustainable measles mortality reduction 1. Strong routine immunization of > 90% 2. Provide second opportunity for measles immunization 3. Surveillance 4. Improved case management
, 44% of")
Measles 2 nd opportunity, 1999 and 2005 1999 125 member states (65%), 44% of birth cohort Activities 1999 -2005: • 46 Countries added • 603 mil vaccinated in SIAs 2005 171 member states (89%); 64% of birth cohort measles 2 nd opportunity no measles 2 nd opportunity
 Estimated")
Reducing Measles Mortality by >50% by 2005 (compared to 1999: 873, 000 deaths) Estimated Measles Mortality by Year Source: Measles Initiative. Lancet Jan 18, 2007
 2010 90%")
GIVS Goal: 90% Reduction in Global Measles Deaths by 2010 (vs. 2000) 2010 90% measles Enhanced measles mortality reduction case-based goal Surveillance 2005 50% measles mortality reduction building from goal achieved! Polio Eradication experience 90% Source: WHO/IVB measles deaths estimates, November 2006
 Strategy for Routine Immunization Strengthening · Re-establishment of outreach")
The Reach Every District (RED) Strategy for Routine Immunization Strengthening · Re-establishment of outreach services · Supportive supervision · Community links with service delivery · Monitoring and use of data for action · Planning & management of resources Launched in 2002, RED strategy was implemented in 53 countries by end of 2005

Impact of RED activities on districtlevel distribution of DPT 3 Coverage in 25 AFR countries implementing the RED strategy 2005 RED 2002 1865 districts 2041 districts District Performance: "Low"=<50%DTP 3; "Medium" = 50 -80% DTP 3; "High" = >80% DTP 3 - "RED implementatiion" is as of 2006; starting date may vary Source of data: WHO-UNICEF Joint Reporting Form – Analysis includes only countries with full reporting on district level coverage in 2002 and 2005

Countries with DTP 3 coverage <50%: 1990, 2005 1990 DTP 3 coverage < 50% (19 countries) 2000 DTP 3 coverage < 50% (20 countries) 2005 DTP 3 coverage < 50% (9 countries) Source: WHO/UNICEF estimates, 2006 192 WHO Member States. Data as of November 2006

Summary and Conclusions § Exciting progress on the global immunization front § Unprecedented financing for immunization is now available for lowincome countries § Introduction of “new” vaccines is proceeding but financing will be the major challenge § Strengthening weak immunization systems in poor countries is difficult and will require long-term investments

Thank you
- Slides: 48