Nasogastric Intubation GI Tract Oral cavity Pharynx Esophagus

Nasogastric Intubation

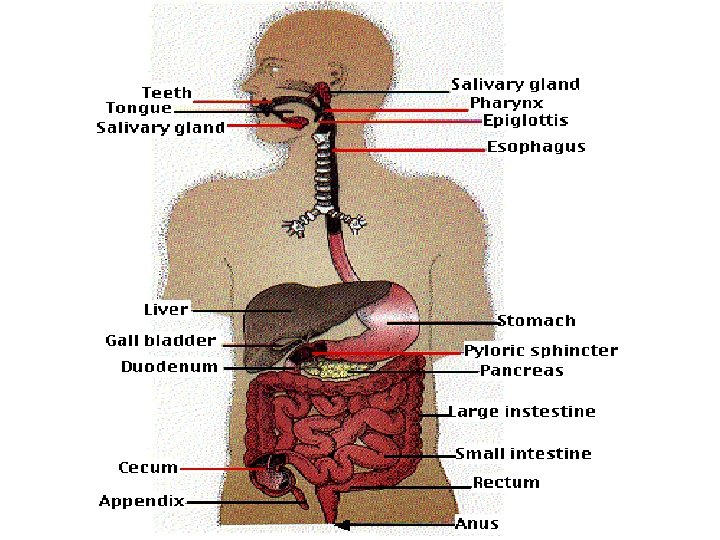
GI Tract • • Oral cavity Pharynx Esophagus Stomach • Small Intestine • Large Intestine • Accessory Structures

Gastrointestinal System • Provides body with: – Water – Electrolytes – Other nutrients used by cells

Gastrointestinal System • Function – Breaks down ingested food – Propels food through the GI tract – Absorbs nutrients across wall of lumen of GI tract – Absorbs water and salts – Eliminates waste

Oral Cavity • Chemical Digestion – Salivary glands produce saliva – Contains digestive enzyme • Salivary amylase • Begins chemical breakdown of carbohydrates

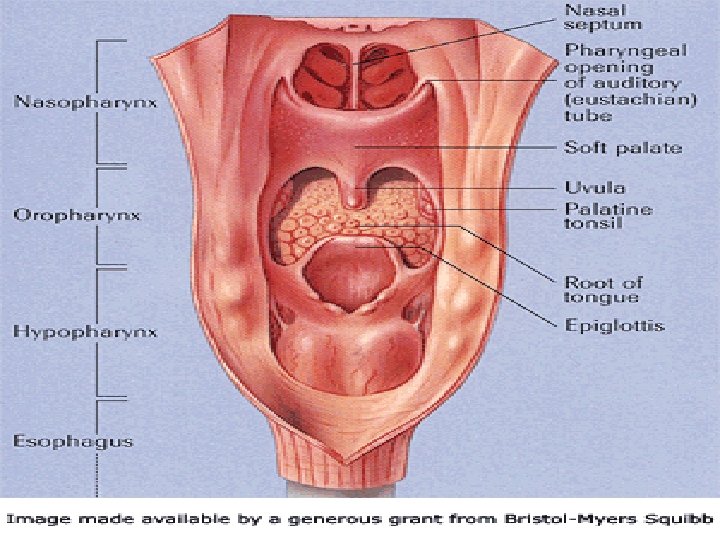
Oral Cavity • Mechanical Digestion – Mastication facilitates swallowing and processing of food – Food swallowed by voluntary and involuntary mechanisms – Pharynx elevates to receive food from mouth

Oral Cavity • Mechanical digestion – Esophageal sphincter relaxes, opening esophagus – Food is pushed into esophagus – Epiglottis closes airway to prevent aspiration

The Gastrointestinal System The Oral Cavity • Chemical digestion • Mechanical digestion Esophagus • Peristaltic waves
 • Extends from pharynx to stomach •")
Esophagus • Muscular canal (24 cm long) • Extends from pharynx to stomach • Begins below cricoid cartilage • Descends to sphincter of stomach

Esophagus: • Muscular canal • About 24 cm long • Extends from pharynx to stomach

Esophagus • Composition • Lined with mucous membrane • Peristaltic waves push food into stomach

Stomach Structure • Layered muscular tube • Lined with mucous membranes • Contains gastric glands

Stomach • Function – Storage and mixing chamber – Secretes HCl, intrinsic factor, gastrin, pepsinogen – Produces chyme – Moves chyme into duodenum

Small Intestine • Begins at pyloric sphincter • Coils through abdominal cavity • Opens into large intestine

Small Intestine • 10 ft divided into 3 segments – Duodenum – Jejunum – Ileum • Mixing and propulsion of chyme • Absorption of fluid and nutrients

Small Intestine • Peristaltic contractions – Chyme moves through ileocecal valve • Chyme enters cecum • Cecum distends – Sphincter closes – Prevents contents from returning to ileum
 long 6. 2 cm (2.")
Large Intestine • • 1. 2 m (5 ft) long 6. 2 cm (2. 2 in) in diameter Extends from ileum to anus Attached to abdominal cavity by mesocolon

Large Intestine • Divided into four principal regions – Cecum – Colon – Rectum – Anal canal

Large Intestine • • Absorbs water Absorbs salts Bacteria acts on undigested material Converts chyme into feces

Liver • Largest gland in body • Upper right quadrant • Vascular organ with 2 sources of blood supply – Hepatic artery – Portal vein Liver Hepatic Artery Portal vein

Liver Plays major role in: • Iron metabolism • Plasma-protein production • Detoxification

Liver • Secretes bile – 600 – 1000 ml each day – Dilutes stomach acid (no digestive enzymes) – Emulsifies fats • Bile salts – Reabsorbed in ileum – Carried back to liver in blood – Also lost in feces

Liver • Metabolism – Helps maintain blood glucose levels – Involved in fat and protein metabolism – Stores vitamins and minerals • Toxin Breakdown – Breaks down metabolism by-products – Can be toxic if accumulate in the body

Liver • Blood Protein Production – Albumin – Fibrinogen – Globulin – Clotting factors
 • Located")
Gallbladder • Pear shaped sac • 7 -10 cm long (3 -4”) • Located on posterior surface of liver • Hangs from anterior/inferior margin of liver

Gallbladder • Secretes and stores bile produced by the liver
 long 2. 2 cm")
Pancreas • • Gland 12 -15 cm (5 -6 in) long 2. 2 cm (1 in) thick Posterior to the stomach • Connected to duodenum by 2 ducts

Pancreas • Exocrine gland – Secretes pancreatic juice • Endocrine gland – Secretes hormones (insulin) into blood – Cells need insulin to process glucose

Pancreas • Pancreatic juice – Most important digestive juice – Contains digestive enzymes, sodium bicarbonate and alkaline substances – Neutralizes HCl in juices entering small intestine

Nasogastric Intubation

NG Tube Indications • Aspirate stomach contents – Diagnostic or therapeutic • Assessment of GI bleeding • Determine gastric acid content

NG Tube Indications • • • Treat paralytic ileus Treat intestinal obstruction Recurrent vomiting likely Trauma Overdose

NG Tube Contraindications • Esophageal strictures • Alkali ingestion, caustic ingestions, esophageal burns • Comatose patients

NG Tube Contraindications • Trauma patients with: – Cervical or intracranial bleeding – Increased intracranial pressure • Recent surgery of the following types: – Oropharyngeal – Nasal – Gastric

Inserting NG Tube • Explain procedure • Position patient – High Fowler if alert – Drape – Emesis basin – Water and straw

Inserting NG Tube • Unconscious patient – Left lateral position – Head turned to downward side – Gag and cough reflexes absent or suppressed – NG tube easily misplaced (lung) – Inability to swallow

Inserting NG Tube • Check nares for patency • Select appropriate tube size • Determine length of insertion – Tip of nose, to ear, to xiphoid process – Mark tube

Inserting NG Tube • Lubricate tube – Lubricant must be water-soluble – May use topical anesthetic if available (ie, lidocaine) • Coil tube to shape it into curve • Have patient hold water and straw to mouth

Inserting NG Tube • Insert tube – Along floor of nose – Straight back – Advance until resistance felt (nasopharynx)

Inserting NG Tube Ask patient to swallow sips of water and flex neck slightly. As patient swallows, advance tube into and down esophagus.

Inserting NG Tube • When tube is in the esophagus: – Advance rapidly to the pre-marked distance Excessive choking, gagging, coughing, change in voice or condensation inside the tube indicates possibility of placement in trachea. The tube should be withdrawn.

Confirm NG Tube Placement • X-ray – Most reliable if tube is radiopaque – Requires order from physician • Injecting air – 60 cc catheter syringe – Place stethoscope over LUQ of abdomen – Inject air into lumen of tube, NOT blue pigtail – Listen for “swoosh” sound

Confirm NG Tube Placement • Aspirate stomach contents – 60 cc catheter tip syringe – Pull back to check for gastric aspirate – Possibility for fluid to be from lungs or pleural space

Confirm NG Tube Placement • Test p. H of gastric aspirate – 60 cc catheter-tip syringe and p. H paper – p. H < 4 = 95% chance that tip is in stomach – p. H > 6 = may be in lung or pleural space; could be in stomach if patient takes antacids or some medications

Confirm NG Tube Placement • Non-radiopaque methods – Possibility of error – Use more than one method – Passage into lungs frequent; especially in comatose or demented patients – Aspiration of gastric contents more reliable • Especially if tested with p. H paper

Securing the Tube • Secure to patient’s nose – Tape to nose and coil around tube – Avoid pressure to nares – Secure to patient’s clothing near shoulder area – Blue pigtail must be above level of patient’s stomach

Complications Excessive coughing, motion, gagging may aggravate the following: • Neck injuries – Increased risk for C-spine injuries • Penetrating neck wounds – May increase hemorrhage • Tube misplacement – Pulmonary – Intracranial
 • Attach")
Removing NG Tube • Disconnect from drainage container and suction (if applicable) • Attach syringe-tip catheter to lumen of tube • Flush tube with 20 cc of air – Empties contents from tube to prevent aspiration into lungs

Removing NG Tube • Remove tape from patient’s nose • Unpin tube from gown • Have patient take deep breath and hold while tube is removed • Pull tube with quick and steady motion • Discard appropriately • Provide or instruct patient on oral and nasal care
- Slides: 52