Narcotics Safety Sean OMahony MB BCh BAO Stacie

Narcotics Safety Sean O’Mahony MB BCh BAO Stacie Levine MD Coleman Foundation Winter Conference February 28, 2014


Learning objectives 1. Incorporate recent regulatory changes in regard to the prescription of opioid medications into practice 2. Appropriately use opioid medications in patients with chronic pain “Universal Precautions” 3. Incorporate strategies for identifying and mitigating opioid misuse 4. Incorporate non-pharmaceutical modalities into the treatment of chronic pain
 • Boston University School")
Additional resource • SCOPE (Safe and Competent Opiate Prescribing Education) • Boston University School of Medicine http: //www. extendmed. com/scopeofpain/home. html

Case #1 • 40 year old female visits a primary care doctor after discharge from medical center following laminectomy and fusion. It’s her first appointment at this location. She brings a box of transdermal Fentanyl 100 mcg patches and requests that you refill her script as her pain is a “ 20 out of 10”. • The physician prescribes the patches assuming that her reports of having received a script for this is true. • 2 days later the provider receives a call from the ER that she was placed on a narcan (naloxone) infusion because of obtundation

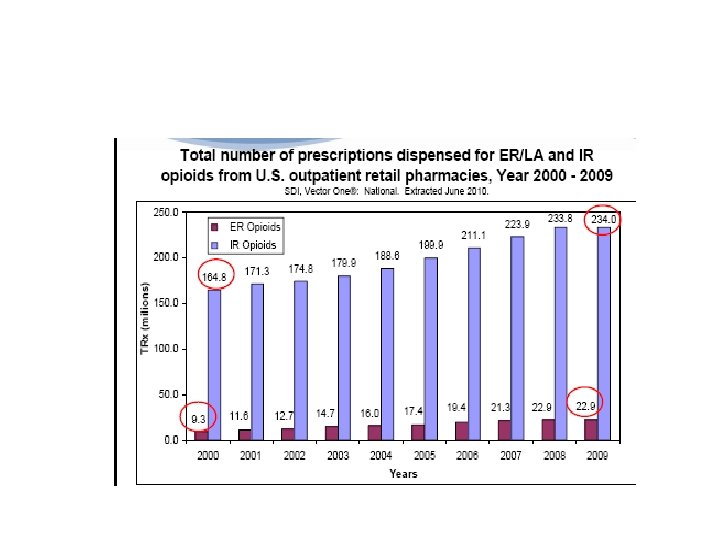
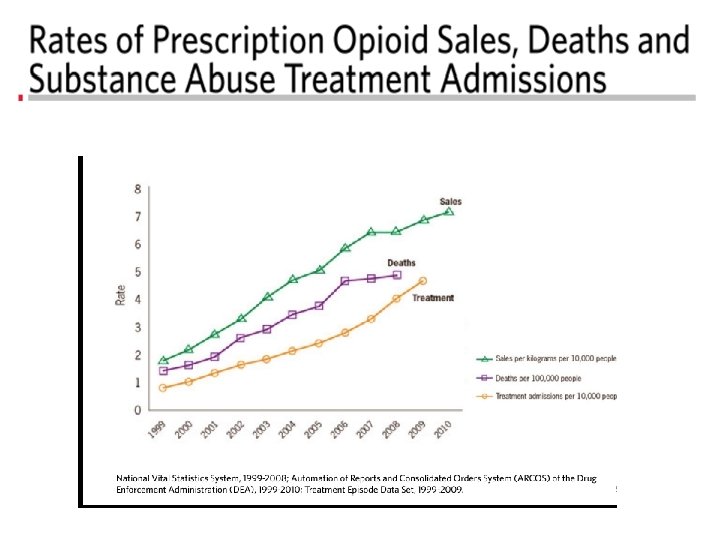
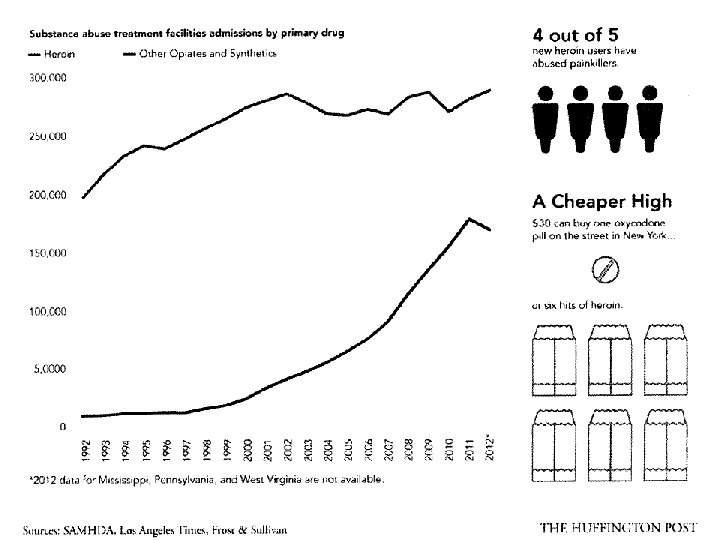
CDC Drug Mortality Data • 425, 000 visits to ER in 2009 -non medical or inappropriate use of opioid medications -15, 600 deaths attributed to opioid medications ->70% of prescription medication overdose related deaths -more than deaths from cocaine and heroin combined • This number has increased more than fivefold in the last 10 years.

Prescriptions Sold by State 2010 Drug Overdose Deaths 2008

Universal Precautions and Opioid Risk Assessment Questions: How often do you screen your patients for risk of misuse when prescribing opioids? Does your current health system have policies and procedures in place for safe prescribing?

Opioid regulations • The need to balance access for relief of suffering needs to be balanced by patient safety education and safeguards • 2012 FDA and the DEA released its final Risk Evaluation and Mitigation strategy for extended release opioids (REMS) • Prescription Drug Monitoring Programs (PDMPs)
 to the FDA in 2012 -Recommended")
Citizen’s petitions • Physicians for Responsible Prescribing (PROP) to the FDA in 2012 -Recommended restricting opioid use in non cancer pain to “severe pain” -For only 90 days or less -Limit of 100 mg/day for ambulatory patients • FDA response

State regulatory requirements • States with highest rates of adverse events have enacted strictest legislation (Washington 2013) • Medicaid and Workers’ compensation program -Any patient on>120 MG oral morphine equivalent/ day must see a pain specialist • Subsequent waiver for hospice and palliative medicine • Deaths and per capita opioid consumption are dropping but many chronic pain patients report being terminated from their PCP’s practices

Prescription Drug Monitoring Programs • All states except Missouri have passed legislation establishing PDMPs • Have been shown to reduce opioid prescription rates • Have not been shown to reduce prescription opioid abuse or overdoses https: //www. ilpmp. org/

Case #1 Patient visits a primary care doctor after discharge from medical center following laminectomy with fusion. It’s her first appointment at this location. She brings a box of transdermal Fentanyl 100 mcg patches and requests that you refill her script as her pain is a “ 20 out of 10”. -What is the preferred way to assess pain in this patient? -What measures should the provider take to ensure accuracy of information? -What safeguards should be put into place in regards to safe opioid prescribing?
, Visual Analog, Faces •")
Pain Assessment • Pros and cons: Numeric Rating (0 -10), Visual Analog, Faces • Mc. Gill, Brief Pain Inventory - not practical in primary care • Assessment that includes function gives much better information on effectiveness of treatment

Aligning pain rating to functioning probably safer way to assess
 Scale")
PEG (Pain, Enjoyment, General Activity) Scale

Risk of opioid misuse

Opioid misuse risk • Known risk factors -Age < 45 -Personal history substance abuse -Family history substance abuse -Legal history (i. e. DUI, incarceration) -Mental health problems -Sexual abuse

Case #1: Additional history No psychiatric history Denies illicit drugs Drinks 2 -3 beers every other day Former waitress, on disability for chronic back pain Medications – norco post-op 5/325 mg but ran out early • Was taking her friend’s fentanyl • • • -How do we assess her risk of misuse?

Opioid Risk Tool

Risk screening tools: how can these results be used? • Level of concern communicated to the patient • Level of monitoring should be implemented • Need for pain specialist or addiction consultant? • Some patient may be too risky for opioids, use nonopioid modalities as much as possible

Screen for unhealthy Etoh or drug use • Alcohol: do you sometimes drink wine or beer or other alcoholic beverages? • How many times in the past year have you had 5 (4 or more for a woman) in a day? • How many times in the past year have you used illegal drugs or prescription medications for non medical reasons?

Screen for mental health problems • Screen for mental health problems e. g. PHQ 2, PHQ 9 • Screen for self harm • Screening tool for addiction risk (e. g. COMM) • Screen for PTSD

Universal precautions for opioid prescribing • Consistent application takes pressure off provider • Reduces stigmatization of patients • Standardizes office policies • Concurs with national guidelines -American Pain Society, American Academy of Pain Medicine

Common universal precautions • Ensure there is a single prescriber, regular visits • Use multidimensional and nonpharm. approaches to pain management • Monitor for adherence, misuse, diversion -random pill counts, patient agreements, random urine drug testing • Enroll patient in a recovery program if evidence of addiction • Provide supportive counseling • Manage psychiatric co-morbidities

Patient Prescriber Agreement • Means of setting boundaries • Should not be used with the intent of getting rid of problematic patients • Should be readable, reasonable and flexible

Pill counts • Confirm adherence, minimize diversion • 28 days instead of 30 • Prescribe so patient has residual medications at appointments • Patient brings in medications at each visit • If concerned, can do random pill counts

Urine drug testing • Window of positivity is 1 -3 days • Specify to lab if you expect to find the presence of a particular substance • Take a history including over the counters, herbals and time of last use • Initial testing is done with class specific assay • Gas Chromatography will confirm the presence of an individual medication or its metabolites • Different labs different test menus and cut-offs

When using opioids – the Four “A’s” ü Document Analgesia ü Document Aberrant behaviors ü Document Adverse Events ü Document Activities of Daily Living ü Document the name and dose of all pain medications on admission note and at all clinic visits. ü Document the route of administration. ü Look for patient agreement ‘pain contract’ in EMR
 • Patient engagement")
Monitoring strategies during patient visits • Assess progress towards goals (function) • Patient engagement in self-care (exercise, stretching) • Use of non-pharmaceutical modalities (CAM, PT) • Psychiatric, emotional, social issues • How patient has been taking medications • Objective information: pill counts, urine test

When to refer to pain management/consultant? • Increased risk patient: in recovery/ family history but no current psychiatric or addictive disorder • Referral to a multidisciplinary pain management clinic for on-going pain management if uncontrolled pain or active chemical dependency, psychiatric problem • Communicate these concerns with the pain clinician when making the referral Gourlay 2004

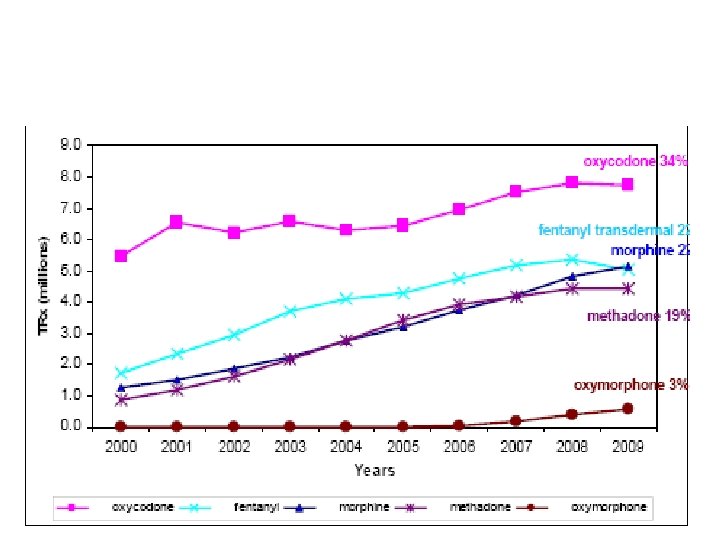
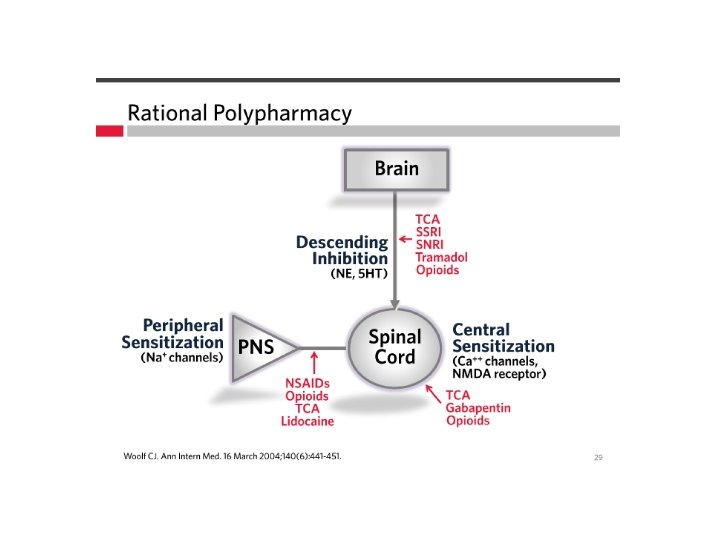
Rational opioid prescribing

Case #2 • 90 yo nursing home patient with dementia • PAD, s/p bilateral AKA with phantom pain • Hydrocodone/APAP 5/325 mg q 6 hours, worsening pain • Admitted to hospice • Switched to methadone 10 mg po TID • Patient found with decreased mental status and respirations, died within three days

Case #3 • 54 YO man with recurrent oral squamous cell carcinoma neuropathic neck pain • Pain is ‘electrical’ in the lateral neck area, severe for most of the day and interfering with sleep and mood • Transdermal fentanyl 100 MCG/72 + hydromorphone 12 MG q 3 hours, minimal relief • Also on gabapentin 600 mg p. Gtube TID, and lidoderm 5% patch • Tried other opioids: oxycodone, morphine • Should we try methadone?

Multidimensional approach to treatment • Opioids • Adjuvants • Neuralaugmentation • Ablative Surgery Suffering Pain Perception Nociception Loeser JD, Cousins MJ. Med J Aust. 1990; 153: 208 -12, 216. • Psychotropics • Anti-depressants/ • Cognitive therapies • Relaxation • Spiritual • NSAIDS • Radiation • Chemotherapy • Local blocks • Surgery • Physical modalities

Methadone – a special medication
 • Analgesic duration 6")
Methadone • Long and variable half-life (12 – 120 hours) • Analgesic duration 6 -8 hours • QTc prolongation, Torsades • Benefits -mu agonist, NMDA receptor antagonist -less tolerance, neuropathic pain -safe in renal disease -less street value -inexpensive

Methadone – many drug interactions

Methadone conversion caution Daily Morphine <100 mg 101 -300 mg 301 -600 mg 601 -800 mg 801 -1000 mg >1000 mg Methadone: Morphine (1: 3) (1: 5) (1: 10) (1: 12) (1: 15) (1: 20) Gazelle. Methadone for the treatment of pain. J Pall Med. 2003; 6(4): 620
 • Transdermal fentanyl 100 MCG/72 hours • Hydromorphone 12 MG q")
Case #3 (cont) • Transdermal fentanyl 100 MCG/72 hours • Hydromorphone 12 MG q 3 hours, using ATC Discuss at your table how you would switch to methadone What surveillance does this patient need to ensure safety?

When You Suspect Aberrant Behaviors

Case #4 • 51 yo woman with diffuse visceral, neuropathic pain brain and liver metastases on 4 th line chemotherapy for breast cancer • Medications: -Oxycodone IR 40 mg q 4 hours prn (using every dose) -Diphenhydramine 50 MG q 8 hrs prn itch (requesting dose increase) -Alprazolam 0. 5 MG BID prn (using every dose) • Runs out of medications early • Frequently sleepy when she comes in for chemotherapy
 • Depressed, not seeing a mental health provider • Condominium")
Case #4 (cont. ) • Depressed, not seeing a mental health provider • Condominium recently repossessed • You request involvement of her husband at her next visit so that he can help with monitoring of her prescription opioids • She is skeptical of this. Her husband ‘doesn’t understand her’. -Is she “addicted”? What do you do?
 • Risk factors -personal")
Abuse/addiction • Published rates in chronic pain population ~10% (3%-50%) • Risk factors -personal history of substance abuse -family history of substance abuse -co-morbid psychiatric condition -abuse as child

Opioid pharmacology and addiction Natural and Semisynthetics Synthetic

Why people become addicted to opioids • • Activate mu receptors in midbrain Dopaminergic pathways = euphoria Fast acting opioids most rewarding (IV) ER/LA are often adulterated for same effect (chewed) which has lead to overdose

Outpatient management of the chemically-dependent pain patient • Maximally structured approach includes: – – – – Frequent visits Pain agreement Limited supply of medications (weekly, monthly) Rotate from short acting agents to primarily long-acting opioids with low street value Ask pharmacy to run a profile of recently filled medications. Urine Point of Service toxicology and Mass Spectroscopy (MS)/Gas Chromatography (GC) Recovery program/psychotherapy Referral to addiction specialist

Case #5 • 51 YO woman with HIV, triple negative breast cancer HIV neuropathy, worsening pain • Use of alcohol, MJ and subsequently cocaine and heroin consistently from age 14 until age 49 • Incarceration in her 30 s for drug trafficking • Has 2 teenage daughters in the custody of her mother. • Lives alone, poor relationship with family • Gabapentin 600 MG TID, Topiramate 25 MG BID • New skeletal metastases – on oral chemo, XRT, NSAIDs -How would you manage this patient?
 • Meets weekly with a substance abuse counselor that you work")
Case #5 (cont) • Meets weekly with a substance abuse counselor that you work with in the HIV clinic • Meets monthly with you in the clinic • UDTs always positive for ‘opiates’ and nothing else • Participates in recovery groups and abstinence promotion groups • Comes to all of her primary care appointments • Getting acupuncture in the clinic • Excited to have recently had her 2 nd anniversary of being sober.

Non-Pharmacologic Modalities

Case #6 • 69 yo female with metastatic rectal cancer and chronic low back pain • Prior ETOH • Lives with boyfriend of 15 years, no longer a couple • Existential distress • Reluctant to take antidepressant • Escalating doses of opioids, states they are ineffective for somatic pain • Using melatonin and lavender baths for insomnia • Requesting alternative methods to control pain What do you do?

CAM – Malignant pain • 2007 National Health Interview Survey -65% diagnosed with cancer had used CAM -53% non-cancer -Cancer patients rated most likely to use CAM for general wellness, immune enhancement, and pain management. • Many people do not inform their healthcare providers of CAM use (15 -23% of users)

CAM – Non-malignant pain • 44% with painful neurologic conditions sought help from CAM practitioners. IOM (Institute of Medicine). 2011. Relieving Pain in America: A Blueprint for Transforming Prevention • 60% who used CAM for back pain perceived a “great deal” of benefit. Kanodia A 2010 Perceived Benefit of Complementary and Alternative Medicine (CAM) for Back Pain: A National Survey • Veterans with chronic non-cancer pain -80% tried CAM -all willing to try four CAM modalities being studied (massage, acupuncture, chiropractic, herbal medicine). Denneson L J Rehab Res & Dev. 2011; 48(9)1119: 1128
 -Decrease 1. 4")
Acupuncture and malignant pain • Surgical oncology (Peri-operative acupuncture and massage) -Decrease 1. 4 points on a 0 -10 pain scale vs 0. 6 in the control group (P=0. 038) -Decrease depressive mood J Pain Symptom Manage 2007 Mar; 33(3): 258 -66 • Breast Cancer RCT Traditional Acupuncture vs. Sham Acupuncture -efficacy for joint pain in patients receiving aromatase inhibitors J Clin Oncol 28: 7 2010

Acupuncture and malignant pain • Auricular acupuncture ->30 MM VAS after analgesic therapy for>1 month -Treatment: Pain intensity decreased by 36% at 2 months -Placebo (2%). -(P <. 0001). Journal of Clinical Oncology, Vol 21, Issue 22 (November), 2003: 4120 -4126

CAM – other • Integration of cognitive behavioral therapies into management of pain targeted to specific symptoms such as pain and fatigue can significantly reduce pain severity Level of Evidence I Given B 2002, Anderson KO 2007 • Art Therapy and Music Therapy have been shown to be helpful for procedural pain in pediatric cancer patients • J of Pediatric Oncol Nursing 2010 May-Jun; 27(3): 146 -55 • RCTs have also shown benefits for hypnosis on procedural and peri operative pain J of the National Cancer Institute 99: 17 2007

Acupuncture and non-malignant pain • There are promising findings in some conditions, such as chronic low-back pain and osteoarthritis of the knee • Acupuncture appears to be effective for a variety of pain conditions, including carpal tunnel syndrome, fibromyalgia, headache/migraine, low-back pain, menstrual cramps, myofascial pain, neck pain, osteoarthritis pain and postoperative dental pain. http: //nccam. nih. gov/health/acupuncture-for-pain. html

Biofeedback and non-malignant pain • Meta-analysis over 100 empirical studies -50 % reduction in headache symptoms following biofeedback/relaxation therapy with stress management training Mc. Grady, Andrasik, Davies, et al, 1999

Mindfulness based stress reduction • Systematic review of 3 RCTs with 119 adults effective for short and long term relief of chronic low back pain in younger adults • Negative results in older adults Cramer H BMC Complement Altern Med. 2012 8 week RCT trial of MBSR vs. a multidisciplinary pain clinic -MBSR was as effective at reducing pain intensity and lessening pain distress at 6 months • Wong SY Clin J Pain 2011

Yoga • A systematic review of 10 RCTs for pain syndrome • 9 of the 10 reported significant reduction in pain Posadzki Complement Ther Med. 2011 Oct; 19(5): 281 -7

Homeopathy • No studies have shown effectiveness specifically for pain: studies of the most popular homeopathic remedy for tissue inflammation, arnica, have failed to show its effectiveness over placebo.

Conclusions • Opioid prescriptions and misuse are on the rise • Universal precautions and safe opioid prescribing should be integrated into everyday palliative medicine practices • Consider additional non-pharmacological modalities (i. e. CAM) for patients with pain syndromes
- Slides: 67