Name of presentation by Mr X Endocrine Part

Name of presentation by Mr X Endocrine Part Three Thyroid Disorders 2016

Specific Disorders of the Thyroid • Hyperthyroidism- Grave’s Disease – Excessive secretion of thyroid hormones, T 3 and T 4 – Increased metabolic processes – Overactivity and changes in thyroid gland may be present – Most often in women 30 -50 – Symptoms called “Thyrotoxicosis”

Specific Disorders of the Thyroid • Hyperthyroidism- Grave’s Disease – Graves’ disease, thyroiditis, or iatrogenic hyperthyroidism • Graves disease – most common, associated with goiter and exophthalmos. Considered to be autoimmune disorder • Thyroiditis – amalgamation of thyroid gland causing increase in thyroid hormone • Iatrogenic hyperthyroidism – cause by ingestion of exogenous thyroid hormone
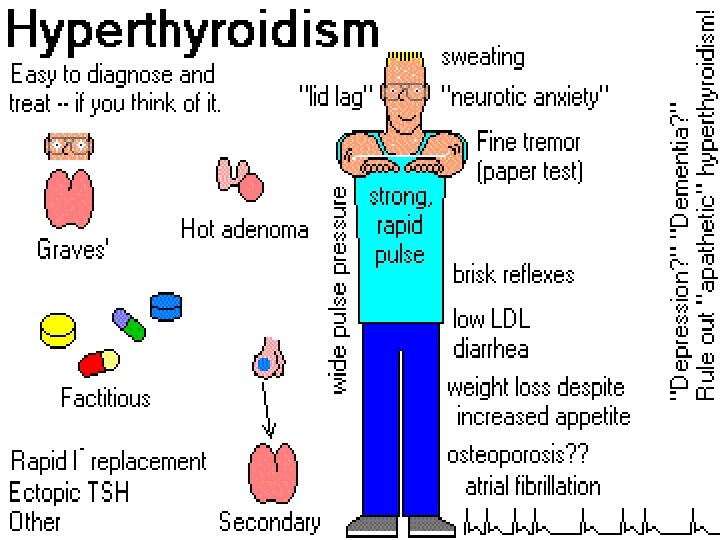

Hyperthyroidism- Grave’s Disease • Clinical Manifestations – Nervous, irritable, and excitable – increase in appetite with progressive weight loss – Heat intolerance with frequent perspiration and flushing occur – Exophthalmos and enlarged thyroid gland or goiter – Dyspnea – Tachycardia – Palpitations – Insomnia

Hyperthyroidism- Grave’s Disease • Diagnostic Studies – Serum T 3 and T 4 levels elevated – RAIU Increased

Hyperthyroidism- Grave’s Disease • Management – Treatment directly affected by cause of hyperthyroidism – Pharmacologic therapy • Antithyroid drugs, such as propylthiouracil or methimazole. Drugs help block synthesis of thyroid hormone Toxic effects could be agranulocytosis • Adrenergic blocking agents – Porpranolol (Inderal) to control symptomssympathetic activity such as tachycardia

Hyperthyroidism- Grave’s Disease • Radioactive iodine Therapy – Decreases secretion of T 4 – Decreases actual gland size – Euthyroid state 3 to 6 months – Frequently causes hypothyroidism • Thyroidectomy – Holds risk of permanent need for replacement therapy of thyroid hormones – Possible hypoparathyroidism

Hyperthyroidism- Grave’s Disease • Nursing interventions – Monitor vital signs, daily weights – Administer Antithyroid medications as ordered – Provide for periods of uninterrupted rest • Assign to a private room away from excessive activity • Administer medications to promote sleep as ordered – – Provide a cool environment Minimize stress in the environment Encourage quiet, relaxing diversional activities Provide a diet high in carbohydrates, protein, calories, vitamins, and minerals with supplemental feedings between meals and at bedtime; omit stimulants

Hyperthyroidism- Grave’s Disease • Nursing interventions – Observe and prevent complications • Exophthalmos; protect eyes with dark glasses and artificial tears as ordered • Watch for Thyroid Storm (next lecture) – Provide for patient teaching and discharge planning concerning: • Need to recognize and report signs and symptoms of agranulocytosis (fever, sore throat, skin rash) if taking antithyroid drugs • Signs and symptoms of hyper/ hypothyroidism

What is Agranulocytosis? • Agranulocytosis can result in a dangerous reduction in the number of white blood cells within the body. • A large number of drugs have been associated with agranulocytosis, including antiepileptics, antithyroid drugs and some antipsychotics (the atypical antipsychotic clozapine). • Although the reaction is generally idiosyncratic rather than proportional, experts recommend that patients be told about the symptoms of agranulocytosis (generally starting with a sore throat and a fever).

Thyroid Storm • Uncontrolled and potentially life-threatening hyperthyroidism • Caused by sudden and excessive release of thyroid hormone into the bloodstream • Precipitated by: stress, infection, unprepared thyroid surgery • Now quite rare • Assessment – – Apprehensive patient, restlessness Extreme high temperature Tachycardia, CHF, respiratory distress Delirium, coma

• Figure 1. Electrocardiograms obtained in a 34 -year-old woman who was brought to the emergency department because of sudden loss of consciousness. A, electrocardiogram showing ventricular tachycardia immediately on arrival at the emergency department. B, electrocardiogram showing ventricular fibrillation after a few minutes.

Thyroid Storm • Nursing Interventions – – Maintain patent airway and adequate ventilation Administer oxygenation as ordered Administer IV therapy as ordered Administer medications as ordered • • Antithyroid drugs Corticosteroids Sedatives Cardiac drugs

Thyroidectomy • Partial or total removal of the Thyroid gland – Subtotal thyroidectomy: Hyperthyroidism – Total thyroidectomy: thyroid cancer

Thyroidectomy • Nursing Interventions: Preoperative – Ensure the patient is adequately prepared for surgery • Cardiac status is stable • Weight and nutritional status is normal – Administer antithyroid drugs as ordered to suppress the production and secretion of thyroid hormone and to prevent thyroid storm – Administer iodine preparations (Lugol’s or potassium iodine solution) to reduce the size and vascularity of the gland prevent hemorrhage

Thyroidectomy • Nursing Interventions: Postoperative – Monitor Vital signs and I and O – Check dressings for signs and symptoms of hemorrhage; check for wetness behind neck – Place patient in semi-Fowler’s position and support head with pillows

Thyroidectomy – When getting OOB put your hand behind neck! – Observe for respiratory distress secondary to hemorrhage, edema of the glottis, laryngeal nerve damage, or tetany – Keep tracheostomy set, oxygen, and suction nearby – Assess for signs of tetany due to hypocalcemia secondary to accidental removal of parathyroid glands – Keep calcium gluconate available – Encourage patient to rest voice • Some hoarseness is common • Check every 30 -60 minutes for extreme hoarseness or any accompanying respiratory distress

Thyroidectomy – Observe for thyroid storm due to release of excessive amounts of thyroid hormone during surgery – Administer IV fluids as ordered until patient is tolerating fluids by mouth – Administer analgesics as ordered for Incisional pain – Relieve discomfort from sore throat • Cool mist humidifier to thin secretions • Administer analgesic throat lozenges before meals and PRN as ordered • Encourage fluids – Encourage coughing and deep breathing every hour – Assist patient with ambulation: instruct patient to place hands behind neck to decrease stress on suture line if added support is necessary

Thyroidectomy – Provide client teaching and discharge planning concerning: • Signs and symptoms of hypo/hyperthyroidism • Self-administration of thyroid hormones if total thyroidectomy performed • Application of lubricant to the incision once sutures are removed • Performance of ROM neck exercises 3 -4 times a day • Importance of regular follow-up care
 – Decrease in secretion of thyroid hormone causing hypofunction")
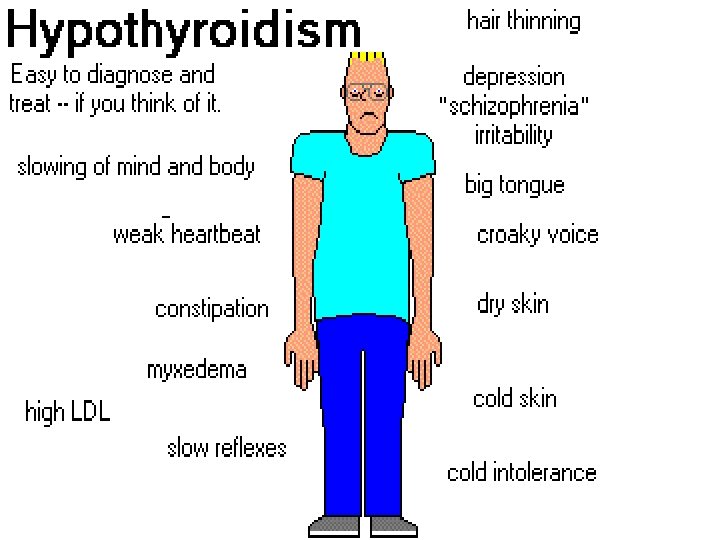
Thyroid Gland • Hypothyroidism (Myxedema) – Decrease in secretion of thyroid hormone causing hypofunction of thyroid gland – Causes • Interference with thyroid hormone • Reduction in thyroid tissue mass Occurs in women between 30 -60 Primary: atrophy Secondary: decreased stimulation from pituitary TSH Iatrogenic: surgical removal of the gland or over treatment of hyperthyroidism with drugs or radioactive iodine – Severe Case: Myxedema Coma – – – Types • Myxedema, juvenile cretinism • Hasimoto’s thyroiditis
 Fatigue, weight gain, anorexia Intolerance to cold")
• • • Symptoms Hypothyroidism (Myxedema) Fatigue, weight gain, anorexia Intolerance to cold Constipation Brittle nails, swollen eyelids Intolerance to cold Dry, scaly skin dry skin Menstrual irregularities Generalized non-pitting edema Bradycardia, CAD, angina pectoris, MI, CHF Increased sensitivity to sedatives, narcotics and anesthetics Exaggeration of these findings in myxedema coma: weakness, lethargy, syncope, bradycardia, hypotension, hypoventilation, subnormal body temperature

RISK FACTORS of Hypothyroidism • Age. Older adults are more likely to develop hypothyroidism. • Female gender. Women are 3 to 4 times more likely to develop hypothyroidism than men. • Family history. People who have close relatives with thyroid disorders are more likely to develop this condition. • Previous thyroid problems. Thyroid disease, goiter, and surgery or radiation therapy to treat thyroid problems increase the likelihood of developing hypothyroidism in the future.

RISK FACTORS of Hypothyroidism • Having an autoimmune disease, such as Addison's disease, type 1 diabetes, rheumatoid arthritis, or pernicious anemia. An autoimmune disease that causes patches of light skin (vitiligo), and premature gray hear (leukotrichia) are seen more often in people with hypothyroidism. • Iodine deficiency. This is rare in the United States but common in areas where iodine is not added to salt, food, and water. • Medications. Some medications can interfere with normal thyroid function, particularly lithium carbonate (used to treat bipolar disorder), amiodarone hydrochloride (such as Amiodarone, Cordarone, and Pacerone), and interferon-alfa (such as Infergen, Rebetron, Wellferon).

Myxedema Coma • Diagnostic tests – Serum T 3 and T 4 level low – Serum cholesterol level elevated – RAIU decreased

Test Result Interferences: Many medications can interfere with thyroid function test results, including: • Corticosteroids and hormones such as estrogen, progesterone, and birth control pills. • Large doses of aspirin. • Warfarin (Coumadin), diphenylhydantoin (Dilantin), carbamazepine (such as Tegretol), amiodarone (Cordarone), lithium (such as Eskalith, Lithonate), clofibrate (Atromid-S, Abitrate), phenytoin (Dilantin)
, and phenylbutazone. •")
Test Result Interferences: • heparin, propranolol (such as Corgard, Inderal, Tenormin), and phenylbutazone. • Contrast material used for certain X-ray imaging tests may affect T 4 results. • Pregnancy can affect thyroid function tests results. • Rough handling, contamination, or inadequate refrigeration of the blood sample can cause inaccurate test results.

Thyroid Gland • Management – Thyroid replacement – Several weeks – Treatment of underlying cause

Myxedema • Nursing Interventions – Monitor vital signs, I&O, daily weights – Observe for edema and S/S of CV complications • Administer thyroid hormone replacement therapy as ordered and monitor effects – Observe for signs of Thyrotoxicosis (tachycardia, palpitations, nausea, vomiting, diarrhea, sweating, tremors, agitation, dyspnea – Increase dosage gradually, especially in patients with cardiac problems

Myxedema • Nursing Interventions • Provide a comfortable, warm environment • Provide a low-calorie diet • Avoid use of sedatives; reduce dose of any sedative, narcotic, or anesthetic agent by half as ordered • Institute measures to prevent skin breakdown • Provide increased fluids and foods high in fiber to prevent constipation • Administer stool softeners as ordered

Myxedema • Observe for S/S of myxedema coma and provide appropriate nursing care – Administer medications as ordered – Maintain vital functions: correct hypothermia, maintain adequate ventilation

Myxedema • Provide patient teaching and discharge planning concerning: – Thyroid hormone replacement • Take daily dose in the morning to prevent insomnia • Self-monitor for signs of thyrotoxicosis • Importance of regular follow-up care • Need for additional protection in cold weather • Measures to prevent constipation
 thyroglobulin (Proloid),")
Thyroid Gland • Myxedema Coma- Medical Management – Drug Therapy: levothyroxine (Synthroid) thyroglobulin (Proloid), dessicated thyroid, liothyronine (Cytomel) – Myxedema coma is a medical emergency • • IV thyroid hormones Correction of hypothermia Maintenance of vital functions Treatment of precipitating causes

Thyroid Gland • Myxedema Coma – – – – – Critical state-high mortality rate-early recognition essential Loss of Consciousness Hypotension Hypothermia Possible respiratory failure From: failure to take meds Infection Trauma Exposure to cold Use of sedatives, narcotics, or anesthetics

Specific Disorders of the Thyroid Gland • Enlargement of the thyroid gland not caused by inflammation or neoplasm – Endemic • Nutritional iodine deficiency • Areas where soil and water deficient of iodine • Most frequently in older children and in pregnancy

Specific Disorders of the Thyroid Gland Goiter – Sporadic • Ingestion of large amounts of goitrogenic foods – Cabbage (Oh God! It St. Patrick’s Day!) – Soybeans (There goes my low fat diet!) – Peanuts, peaches, peas, strawberries, spinach (I give up!) • Use of goitrogenic drugs – Propylthiouricil (PTU) – Cobalt, lithium – Genetic defect preventing synthesis

Specific Disorders of the Thyroid Gland Goiter • Low levels of thyroid hormone stimulate increased secretion of TSH by pituitary; under TSH stimulation the thyroid increases in size to compensate and produces more thyroid hormone • Medical Management – Drug therapy • Hormone replacement with levothyroxine (Synthroid) • T 4 • • • Desiccated thyroid (Not Kosher!) Lithyronine (Cytomel) Small doses of iodine (lugol’s solution) or potassium iodide Avoidance of goirogenic foods or drugs Surgery: subtotal thyroidectomy to relieve pressure symptoms and cosmetic reasons

Specific Disorders of the Thyroid Gland Goiter – Assessment Findings • Dysphagia, enlarged thyroid, respiratory distress – Diagnostic tests • Serum T 4 level low-normal or normal • RAIU uptake normal or increased

Goiter Nursing Interventions • Administer replacement therapy as ordered • Provide care for patient with subtotal thyroidectomy if indicated • Provide patient teaching and discharge planning concerning: – Use of iodized salt in preventing and treating endemic goiter – Thyroid hormone replacement

Thyroiditis • • • Inflammation of the thyroid gland Acute Subacute Chronic Inflammation Fibrosis Lymphocytic infiltration Autoimmune damage to the thyroid Can cause thyrotoxicosis (Thyroid Storm)
 • A) Normal • (B) Graves disease: diffuse increased")
Thyroid Uptake Scans (Technetium 99) • A) Normal • (B) Graves disease: diffuse increased uptake in both thyroid lobes. • (C) Toxic multinodular goiter (TMNG): “hot” and “cold” areas of uneven uptake. • (D) Toxic adenoma: increased uptake in a single nodule with suppression of the surrounding thyroid. • (E) Thyroiditis: decreased or absent uptake.

• Acute Thyroiditis – Caused by infection • Bacteria – Staphlococcus aureus • Fungi • Mycobacteria • Parasites – – – – Edema, fever, dysphagia Dysphonia Pharyngitis / pharyngeal pain Warmth, erythema, tenderness Antimicrobial agent Fluid replacement Surgical incision and drainage Thyroiditis

Thyroiditis • Subacute Thyroiditis – Lasts for 1 to 2 months – Disappears spontaneously without residual effects – Often follows respiratory infection – Females – Painful swelling – Without pain-autoimmune – Treatment aims at decreasing inflammation – NSAIDS-corticosteroids – Beta-blockers to control symptoms (Inderal) – Symptoms of hyperthyroidism

Hashimoto's Disease • Hashimoto's thyroiditis is the most common form of autoimmune thyroid disease. It develops when the body's natural defense system (immune system) makes antibodies that attack and eventually destroy the thyroid gland. This results in a gradual loss of thyroid tissue and thyroid gland function. Hashimoto's thyroiditis is also associated with other conditions, including diabetes, Addison's disease, rheumatoid arthritis, pernicious anemia, and premature menopause. Hashimoto's thyroiditis occurs most often in women and older adults. The disease does not cause any pain and often goes unnoticed for years.

Chronic Thyroiditis • Hashimoto’s Disease – Women 30 -50 years – Not painful – No pressure – Activity level normal or even low – Cell-mediated immunity – Leads eventually to Hypothyroidism – Hormone therapy
")
Hashimoto's Disease • Treatment may be needed if symptoms of low thyroid production (hypothyroidism) develop or if the thyroid gland becomes inflamed and enlarged. If the disease does not cause these problems, treatment may not be necessary. • Although rare, hypothyroidism is seen in infants and children. In infants, if hypothyroidism is treated within the first month of life, the child grows and develops normally. • Untreated hypothyroidism in infants can cause brain damage, leading to mental retardation and developmental delays. Every state in the United States tests newborns for hypothyroidism.

Thyroid Cancer • 20, 000 new cases of thyroid cancer each year in the United States. • Females are more likely to have thyroid cancer at a ratio of three to one. • Thyroid cancer can occur in any age group, although it is most common after age 30 and its aggressiveness increases significantly in older patients. • The majority of patients present with a nodule on their thyroid which typically does not cause symptoms. • Remember, over 99% of thyroid nodules are not cancer! But, when a thyroid cancer does begin to grow within a thyroid gland, it almost always does so within a discrete nodule within the thyroid.

Symptoms of Thyroid cancer • Hoarseness, neck pain, and enlarged lymph nodes • Although as much as 75 % of the population will have thyroid nodules, the vast majority are benign. • Young people usually don't have thyroid nodules, but as we get older, more and more of us will develop a nodule. • By the time we are 80, 90% of us will have at least one nodule. • Far less than 1% of all thyroid nodules are malignant. • A nodule which is cold on scan (shown in photo outlined in red and yellow) is more likely to be malignant, nevertheless, the majority of these are benign as well.

Thyroid cancer • Needle biopsy • papillary, follicular, mixed papilofollicuar, medullary, or anaplastic • Thyroidectomy • possibility of a tracheostomy. • About 4 -6 weeks after the thyroid has been removed, the patient will undergo radioactive iodine treatment. – This is very simple and consists of taking a single pill. The pill will contain the radioactive iodine in the dose that has been calculated for that individual. The patient goes home, avoids contact with other people for a couple of days (so they are not exposed to the radioactive materials)

Thyroid cancer • 1 to 2 weeks after the radioactive iodine treatment the patient is started on a thyroid hormone medication (Synthroid, Levoxyl, Armour Thyroid, etc). • Every 6 -12 months the patient returns to his endocrinologist for blood tests to determine if the dose of daily thyroid hormone is correct and to make sure that the thyroid tumor is not coming back. •

Thyroid Cancer • Fairly common form of cancer • 90% survival rate • Radiation-induced thyroid cancer (nonradioactive potassium iodide inhibits thyroid absorption of radioactive iodide)
- Slides: 52