N Engl J Med 1812 Lancet 1823 BMJ


刊名 创刊年 N Engl J Med 1812 Lancet 1823 BMJ 1840 JAMA 1883 Arch Intern Med 1908 Ann Intern Med 1927 Chest 1935 Chin Med J 1887
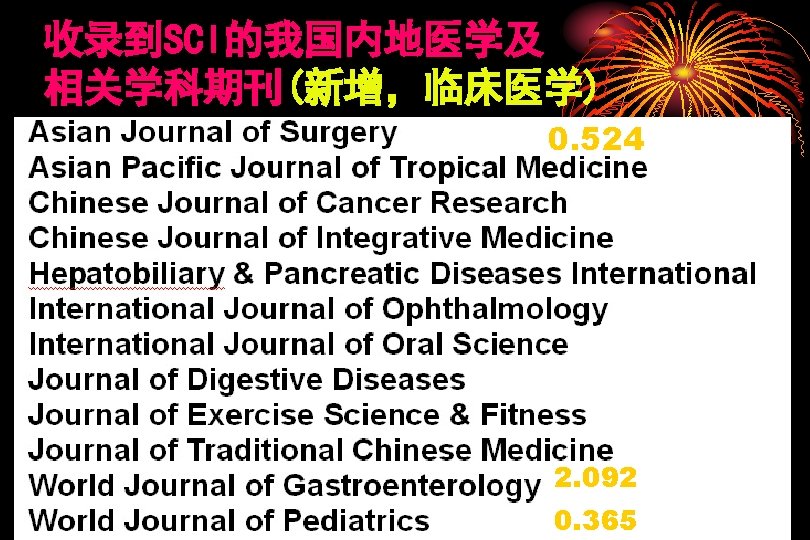
 Journal Titles • • Impact factor Chinese Medical Journal (中华医学杂志 英文版) Acta")
收录到SCI的我国内地医学及 相关学科期刊(原有) Journal Titles • • Impact factor Chinese Medical Journal (中华医学杂志 英文版) Acta Pharmacol Sin (中国药理学报) Cell Res (细胞研究) Acta Biochim Biophys Sin (中国生物化学生物物理学报) Asian J Androl (亚洲男性学) Fungal Diversity (真菌多样性) Science in China – Series C, Life Sciences 0. 858 1. 397 3. 426 0. 931 1. 737 2. 297 0. 533

Reviewer: 1 In this article, the authors present the data on a randomized but not blinded study of oseltamivir, a Chinese herbal combination (CHC), a combination of the two, or placebo in treatment of. . . The authors found similar clinical outcomes with oseltamivir or the CHC compared to placebo but no benefit of the combination. Despite the fact that this is both an interesting finding and a novel approach, there are significant challenges that must be addressed by the authors - either by providing additional details or by discussing why they were not done. Specifically:

1. Introduction - some detail about the CHC needs to be included as well as some background data why was this combination of herbs picked over others (esp since the authors cite other studies of other combinations later)? 2. Methods: A. There were a lot of sites involved - was one IRB approval sufficient? B. How, specifically, was the CHC prepared - how was the solution standardized so that there were comparable amounts of active compounds in each dose? C. Why were the individuals hospitalized? This is not typical for influenza studies in high school students with mild disease?

D. How were symptom scores and symptom alleviation defined? Since one of the most important endpoints is symptom alleviation, why was this only done at discharge instead of when the patients felt better? E. Was no virology, other than initial swabbing, performed? Virologic outcomes are a critical component and failure to assess this significantly limits the value of this study. F. I am surprised that you had such a round number for two different sample size calculations. G. Symptom score is not standardized and definitions are also not consistent with prior flu studies making comparisons challenging.

3. Results - there's little more than what is presented in the abstract - more - including details about changes in symptom scores over time; clearly virology is needed as well. 4. Discussion: A. Need to discuss better how this compound was picked and why the simpler compound wasn't assessed? What is felt to be the active ingredient? Are there studies planned to define this? B. Since the CHC functions with several proposed mechanisms, why do the authors hypothesize that there was no benefit to the combination? C. There are far more limitations than are listed

Reviewer: 2 Summary 1. Double-blind method is not used, although it was randomized controlled trial. 2. Combination therapy of oseltamivir and other CNS stimulating drugs is potentially harmful and is not recommended as routine therapy for influenza especially otherwise healthy teenagers. 3. It is difficult to understand the reasons why you included patients who presented more than 48 hours (but within 72 hours) after the onset of symptoms. 4. Efficacy primary end point (time to resolution of fever) is not appropriate to evaluate the efficacy of oseltamivir.

5. Medication information other than the study drugs was not available except for acetaminophen and antibiotics. Especially NSAIDs and cough medicines affect the outcome but were not described. 6. there seems some bias in the degree of fever and time from onset of illness to intervention 7. However, proportion of participants with complete recovery at discharge was not significantly different in each study group compared control group. 8. Moreover that of M-MXSGT group (62. 4%) is rather lower than control group (69. 6%). 9. Reported adverse events are extremely few. Is it the real figure?

Details 1. Double-blind method is not used, although it was randomized controlled trial. This is stated in your discussion in the manuscript. Further explanation may be unnecessary. 2. Combination therapy of oseltamivir and other CNS stimulating drugs is potentially harmful and is not recommended as routine therapy for influenza especially otherwise healthy teenagers. Teenagers are thought susceptible to serious abnormal behaviours leading to accidents even with fatal outcome[1]. . Other neuropsychiatric adverse reactions to oseltamivir including sudden death especially during sleep are reported [1]. 1) Hama R. 2008 b Fatal neuropsychiatric adverse reactions to oseltamivir: case series and overview of causal relationship. Int J Risk Safety Med: 20: 5 -36 [11]

Several animal experiments are also suggesting the causality, especially used in combination with CNSstimulant such as ephedrine [2, 3] (main ingredient of MMXSGT is ephedra which is the mixture of ephedrine like substances). 2) Izumi Y, Tokuda K, O'dell KA, Zorumski CF, Narahashi T. 2007. Neuroexcitatory actions of Tamiflu and its carboxylate metabolite. Neurosci Lett. 426(1): 54 -8. Epub 2007 Sep 1. 3) Izumi Y, Tokuda K, O'Dell K, Zorumski C, Narahashi T. 2008. Synaptic and behavioral interactions of oseltamivir (Tamiflu) with neurostimulants. Hum Exp Toxicol. 27(12): 911 -7.

3. The reason why you included patients who presented more than 48 hours (but within 72 hours) after the onset of symptoms is not understandable. There has been no proof based on the randomized controlled trials that show the efficacy in reducing time to resolution of symptoms by oseltamivir if it is given after more than 48 hours from the onset of symptoms. So if they include those presented more than 48 hours after the onset of flu symptoms and claim the treatment efficacy of oseltamivir, it is misleading. 4. Efficacy primary end point (time to resolution of fever) is not appropriate to evaluate the efficacy of oseltamivir.
 and has")
Because unchanged oseltamivir that easily enter the brain through blood brain-barrier (BBB) and has CNS depressing action which lower body temperature [3, 4], decreased time to resolution of fever could easily proved without true efficacy against flu. 4) Ono H, Nagano Y, Matsunami N, Sugiyama S, Yamamoto S, Tanabe M. 2008. Oseltamivir, an anti-influenza virus drug, produces hypothermia in mice. Biol Pharm Bull. 31(4): 638 -42. 5. Medication information other than the study drugs was not available except acetaminophen and antibiotics. Especially NSAIDs and medicines for the improvement of cough affect the outcome [4, 5] but were not described.

M-MXSGT has antipyretic action like NSAIDs. it means in the acute phase it decreased body temperature but in the later phase, it disturb the recovery of flu symptoms. This adverse effect may explain lower tendency in proportion of full recovery in the M-MXSGT arm, though the fever resolution was faster than control arm. 5) Hama R. A/H 1 N 1 flu. NSAIDs and flu. BMJ. 2009 Jun 15; 338: b 2345. doi: 10. 1136/bmj. b 2345. 6. There seems some bias in the degree of fever and time from onset of illness to intervention a) Degree of fever: rather lower in control group: per cent of >39 C: 14. 0 % in control arm vs 23. 5 % in oseltamivir arm, 21, 4 % in M-MXSGT arm and 24. 5 % in combination arm. Flu patients with high fever tend to recover faster than those with low fever.
 Time from onset of illness to intervention: rather shorter in control arm (30")
b) Time from onset of illness to intervention: rather shorter in control arm (30 hours) than in the study arms (35, 32 respectively). late presenting may recover earlier, so the baseline factor is more favorable in the study arms than the control arm. 7. However, proportion of participants with complete recovery at discharge was not significantly different in each study group compared control group. Proportions of complete recovery were 69. 6 %, 72. 5 %, 62. 1 and 70. 6 % respectively. 8. Moreover that of M-MXSGT group (62. 4%) is rather lower than control group (69. 6%). Considering the favourable baseline factors, this is more noted and seriously considered and discussed. 9. Reported adverse events are extremely few. It’s unbelievable.

In the RCTs of oseltamivir for treatment of seasonal flu done in the western countries or in Japan, percent of participants who had at least one adverse event were report about 40 to 50 %. 10. Please refer the papers which were published recently on the systematic review on neuraminidase inhibitor especially on oseltamivir: as bellow: http: //www. bmj. com/cgi/content/full/339/dec 07_2/b 5106 http: //www. bmj. com/cgi/content/full/339/dec 10_2/b 5405 http: //www. bmj. com/cgi/content/full/339/dec 08_3/b 5351 http: //www. bmj. com/cgi/content/full/339/dec 08_3/b 5387 http: //www. bmj. com/cgi/content/full/339/dec 07_2/b 5164 http: //www. bmj. com/cgi/content/full/339/dec 07_2/b 5248 http: //www. bmj. com/cgi/content/full/339/dec 08_3/b 5364


- Slides: 34