Myringotomy Page 634 Relevant Anatomy The Tympanic membrane

Myringotomy Page 634

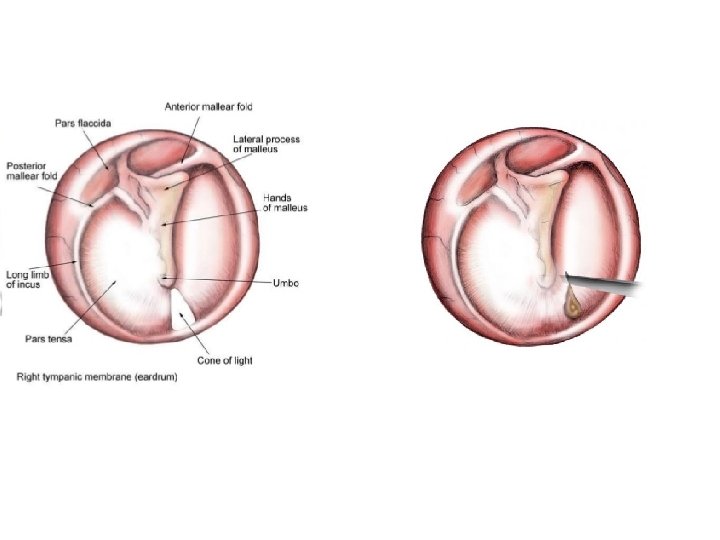
Relevant Anatomy • The Tympanic membrane is the separation between the outer and middle ear. It consists of three layers: outer epithelial, fibrous connective tissue, and mucous membrane. • Concave disk-shaped pearly gray in color, translucent and with a shiny appearance. The fibrous ring surrounding the tympanic membrane is the annulus. The major portion of the membrane is fibrous tissue called the pars tensa. • The superior portion is called the pars flaccida because it lacks the central fibrous connective tissue. The umbo is the point of maximum concavity • A branch of the facial nerve that carries taste impulses from the tongue passes along the inner surface of the membrane. The tympanic membrane can easily rupture. The perforation can be caused by either external trauma or excess pressure from within the middle ear

Pathophysiology • Otitis media is a very common acute inflammation of the middle ear usually caused by blockage of the Eustachian tube causing an accumulation of fluid that normally drains into the nasopharynx. The primary symptom of otitis media is severe ear pain. The main sign observed through the otoscope is an inflamed tympanic membrane. • The infection may require a Myringotomy to remove the accumulated fluid and insertion of a pressure-equalizing (PE) tube to allow for additional drainage and maintain the pressure equalization
")
Preoperative Diagnostics • History and physical exam (Otoscope Exam)

Equipment • • • Hydrogen peroxide to loosen cerumen in ear Pressure-equalizing tubes of various sizes Disposable Myringotomy knife Curette Speculum

Prep • Supine position • A skin prep solution will be used to swab the ear canal, and an anesthetic will be swabbed on the eardrum • Fenestrated Drape

Practical Considerations • The PE tubes are considered implants and must be documented in the patient chart according to health care facility policy as well as federal regulations for medical devices • Myringotomy is not a sterile procedure, but best sterile technique should be maintained like any other procedure. Sterile gloves are donned using the open glove technique, but a sterile gown is not worn. • Only a mayo stand is needed for the procedure • Assess the diameter of the patient’s ear canal and present the surgeon with the appropriate-size speculum. The surgical technologist should be prepared to clean the wax curette with gauze between uses • Fluid may be collected after incision for culture and sensitivity. Suction will be used to remove excess fluid. Keep the suction apparatus patent by suctioning water through it or using the stylet. The fluid from the middle ear is thick.

Surgical Intervention • Following placement of a fenestrated drape, a speculum is placed in the external auditory canal. Any visible wax accumulation will be removed with a curette. • An incision is made in the inferior posterior portion of the tympanic membrane with a disposable Myringotomy knife • A PE tube is placed into the tympanic incision • Final positioning of the tube is achieved. • The speculum is removed. If desired, antibiotic/anti-inflammatory solution or suspension, such as Cortisporin, may be placed in the canal and the canal may then be packed with cotton • If the procedure is planned to be bilateral, the patient’s head will be repositioned, the surgical team members will switch sides, and the sequence is repeated

Post Op • PACU discharged within an hour • Ear canal must be kept dry until PE tubes fall out or are removed and tympanic membrane has healed

Prognosis • Class II • No complications – Hearing returned to normal in a short period of time • Complications: Recurrent infection; occasionally a patient may require a second procedure to remove a retained tube. Death

Tympanoplasty 637

Relevant Anatomy • The middle ear is an air-filled chamber located within the temporal bone the cavity is lined with mucous membrane, which is a continuation of the inner layer of the tympanic membrane. There are two openings in the wall of the middle ear: tympanic antrum that opens into the mastoid sinus; Eustachian tube that connects the middle ear to the nasopharynx • The auditory ossicles are located in the middle ear, lateral to medial: malleus incus and stapes. The ossicles are synovial joints and ligaments connect them to the wall of the middle ear and two tiny skeletal muscles control their movement. The short process of the malleus rests against the tympanic membrane and the head articulates with the body of the incus. The incus is connected to the head of the stapes and the footplate of the stapes rests against the oval window

Pathophysiology • Tympanoplasty is performed to treat conditions affecting the tympanic membrane and the ossicular chain. There are five classifications for Tympanoplasty, arranged by extent of damage to the tympanic membrane and middle ear • I: Limited to tympanic membrane. Soft tissue graft used to replace or repair the ruptured tympanic membrane • II: Includes the malleus either partial or complete • III: Malleus and Incus • IV: All ossicles affected, only remaining natural structure of the middle ear is the intact and mobile footplate of the stapes • V: Remaining footplate is immobile

Diagnostics • CT and MRI

Equipment • Ear drill if mastoidectomy is planned • Any ENT specialty Instrumentation

Preop • General Anesthesia • Supine position • A skin prep solution will be used to swab the ear canal, and an anesthetic will be swabbed on the eardrum • Fenestrated Drape • Local W/ Epi for vasoconstriction and postop pain

Procedural Steps • The surgeon may choose either a transaural or retroauricular approach. If a mastoidectomy is also planned, or the possibility of a temporalis fascia graft exists, the retroauricuar approach is preferred • If the surgeon is planning to use an autograft, the specimen is taken at the beginning of the procedure, so that the sometimes-lengthy graft prep process can begin • The tympanic membrane and the ossicular chain are assessed. A variety of micro instruments may be necessary for the exploration and dissection • Diseased tissues and damaged ossicles are removed • If necessary, the mastoidectomy would be performed at this point • Ossicular reconstruction using materials of the surgeons choice is performed (In a class V a window is made into the horizontal semicircular canal and the tympanic graft seals off the middle ear and provides protection for the oval window)

Continued • Small gelfoam pledgets may be packed into the tympanic cavity to temporarily stabilize the contents of the middle ear and to make a bed on which the new tympanic membrane may rest • The graft is placed under the remnant of the existing eardrum. Additional packing of gelfoam or Vaseline gauze may be placed in the external auditory canal. The retroauricular wound, if used, is sutured • Protective dressing applied
")
Post op • PACU • No forceful nose blowing until healed • Keep ear(s) dry

Prognosis • Class I • No complications – regain full hearing • Complications: Post op SSI hemorrhage Failure to restore full hearing Death

Practical Considerations • The graft will be fragile, handle with caution • If seated remain so
- Slides: 22