Myocardial infarction Lecture 5 Infarction The process by

Myocardial infarction Lecture 5

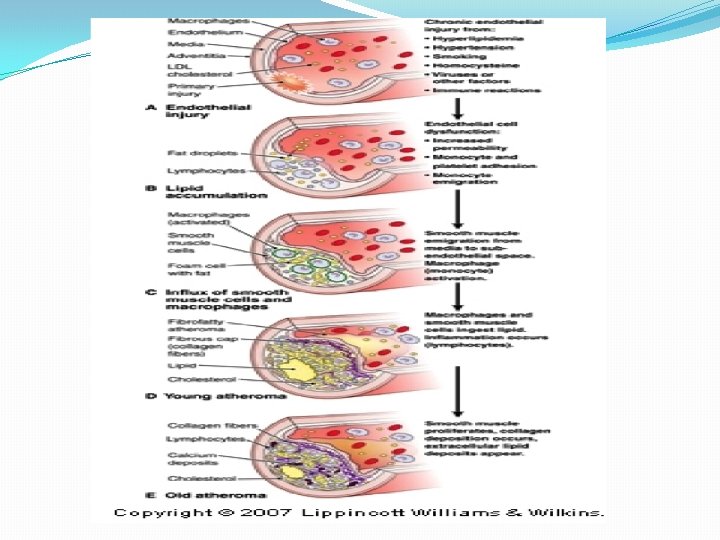
Infarction �The process by which necrosis results from ischemia is called infarction �Ischemic necrosis of myocardial cells is one of the commonest cause of death in industrialized countries.

Pathology �Atherosclerosis �Narrowing of arterial lumen �Reduced coronary blood supply �Clinical manifestations �Chest pain


Diagnosis �History �ECG �Biomarkers

WHO classification of MI 2/3 these criteria: ü Ischemic symptoms ü EKG changes. ü Increased serum markers.

ECG
 � Lactate Dehydrogenase(LDH 1 and 2)")
CARDIAC PROFILE TEST �ENZYMES � Creatinine Kinase –MB(CK-MB) � Lactate Dehydrogenase(LDH 1 and 2) � Aspartate Aminotransferase(AST)/Serum Glutamate Oxaloacetate Transaminase(SGOT) � Alanine Aminotransferase(ALT)/ Serum Pyruvate Transaminase(SGPT) • PROTEINS � Myoglobin � Troponin �LIPID PROFILE � CHOLESTEROL � TRIGLYCERIDE � HDL � LDL

AST found in all tissue, especially the heart, liver, and skeletal muscles It catalyzes the transfer of the amino group of aspartic acid to alpha-ketoglutaric acid to form oxaloacetic acid and glutamic acid Reference range: < 35 U/L in male and < 31 in female Considerations in AST assays -Serum is the best specimen -Hemolyzed samples must be avoided -Muscle trauma like intramuscular injections, exercise, or surgical operation can significantly increase AST levels

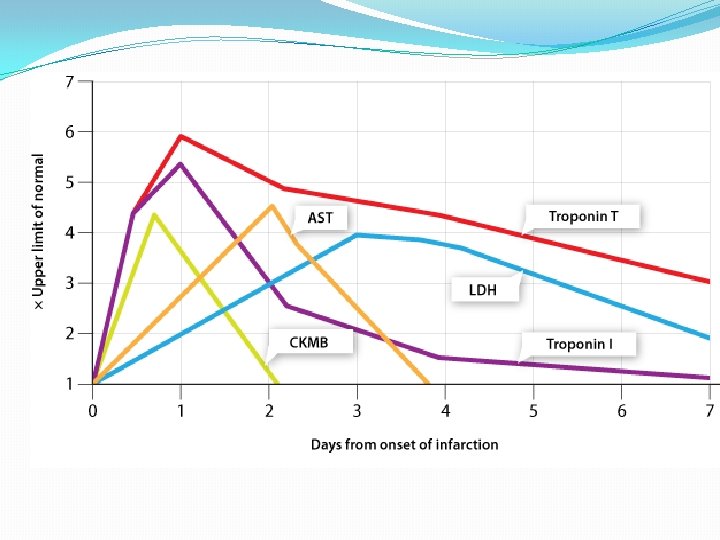
Clinical significance Ø Myocardial infarction q In myocardial infarction, AST levels are usually 4 -10 times the upper limit of normal q These develop within 4 -6 hours after the onset of pain q Peak on the 24 th – 36 th hour q Usually normalize on the 4 th or 5 th day Ø Muscular dystrophy Ø Hepatocellular disorders Ø Skeletal muscle disorders
 �Catalyzes the reversible oxidation of lactate to pyruvate �Used to indicate")
LACTATE DEHYDROGENASE (LDH) �Catalyzes the reversible oxidation of lactate to pyruvate �Used to indicate AMI �Is a cytoplasmic enzyme found in most cells of the body, including the heart �Not specific for the diagnosis of cardiac disease
 �Fast moving fractions")
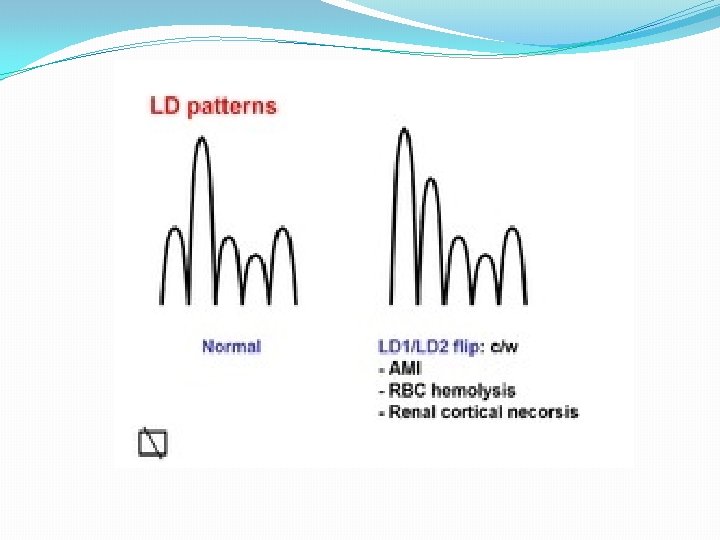
Distribution of LD isoenzymes �LD 1 and LD 2 (HHHH, HHHM) �Fast moving fractions and are heat-stable �Found mostly in the myocardium and erythrocytes �Also found in the renal cortex �LD 3 (HHMM) �Found in a number of tissues, predominantly in the white blood cells and brain �LD 4 and LD 5 (HMMM, MMMM) �Slow moving and are heat labile �Found mostly in the liver and skeletal muscle

Considerations in LD assays �Red cells contain 150 times more LDH than serum, therefore hemolysis must be avoided �LDH has its poorest stability at 0°C Clinical Significance �In myocardial infarction, LD increases 3 -12 hours after the onset of pain �Peaks at 48 -60 hours and remain elevated for 10 -14 days �In MI, LD 1 is higher than LD 2, thus called “flipped” LD pattern

flipped LDH An inversion of the ratio of LD isoenzymes LD 1 and LD 2; LD 1 is a tetramer of 4 H–heart subunits, and is the predominant cardiac LD isoenzyme; Normally the LD 1 peak is less than that of the LD 2, a ratio that is inverted–flipped in 80% of MIs within the first 48 hrs Diff. Dx. LD flips also occur in renal infarcts, hemolysis, hypothyroidism, and gastric CA

Increased levels of LD �Trauma �Megaloblastic anemia �Pulmonary infarction �Granulocyte leukemia �Hemolytic anemia �Progressive muscular dystrophy (PMD)
 �Is a cytosolic enzyme involved in the transfer of energy in")
CREATINE KINASE (CK) �Is a cytosolic enzyme involved in the transfer of energy in muscle metabolism �Catalyzes the reversible phosphorylation of creatine by ATP �-Is a dimer comprised of two subunits, resulting in three CK isoenzymes �The B, or brain form �The M, or muscle form
 isoenzyme � Is of brain origin and only found")
isoenzymes � CK-BB (CK 1) isoenzyme � Is of brain origin and only found in the blood if the blood-brain barrier has been breached � CK-MM (CK 3) isoenzyme � Accounts for most of the CK activity in skeletal muscle � CK-MB (CK 2) isoenzyme � Has the most specificity for cardiac muscle � It accounts for only 3 -20% of total CK activity in the heart � Is a valuable tool for the diagnosis of AMI because of its relatively high specificity for cardiac injury � Established as the benchmark and gold standard for other cardiac markers

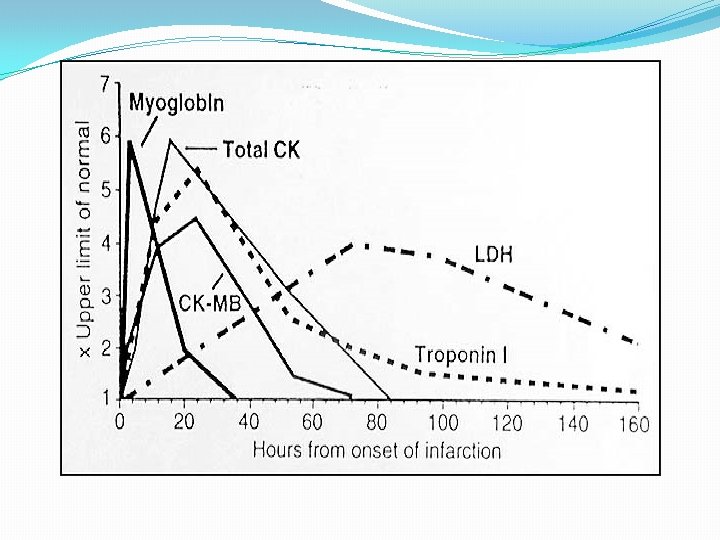
Clinical Significance �-In myocardial infarction, CK will rise 1 -3 hours after the onset of pain �-Peaks at 18 -30 hours and returns to normal on the third day �-CK is the most specific indicator for myocardial infarction (MI) �Ratio of CK-MB/ total CK activity (specificity) �CK-MB mass instead of activity (sensitivity)

Raised levels of CK �Progressive muscular dystrophy �Polymyositis �Acute psychosis �Alcoholic myopathy �Hypothyroidism �Malignant hyperthermia �Acute cerebrovascular disease �Trichinosis and dermatomyositis �Exercise and intramuscular injections causes CK elevations Normal Value: �a. Male – 25 -90 IU/m. L �b. Female – 10 -70 IU/m. L

Myoglobin �Non specific marker �Frequently elevated in other conditions �Most useful when not detected �Can not be used alone for the diagnosis of MI.

Troponins �Proteins that regulate muscle contraction �T & I are specific for cardiac muscles

Cardiac troponins: 1. Troponin C: binds with calcium. 2. Troponin T: binds with tropomyosin. 3. Troponin I: inhibits contraction.

Troponin T & I § Require myocardial necrosis for release from sarcomere. § Early rise (4 -12 hours after symptom). § Peak 12 -24 hours (sensitivity is 100%). § Continuous release up to 10 -14 days
 § Negative troponin")
§ Myocardial infarction: elevation of serum troponin T/I >0. 1. (AHA) § Negative troponin and normal EKG, mortality 1%. § Negative troponin and ischemic EKG: mortatity 4% at 1 month. § Troponin and EKG changes complementary. § Problems with Tn. I: variability of assays. § Complement clinical risk factors and EKG changes.
- Slides: 28