Myeloproliferative Neoplasms overview and treatment Dr Beverley Robertson

Myeloproliferative Neoplasms overview and treatment Dr. Beverley Robertson

Normal blood • Red cells • White cells • Platelets • All floating in clear plasma
 • Polycythaemia Rubra Vera (PRV) • Essential thrombocythaemia (ET) • Myelofibrosis")
Myeloproliferative Neoplasms (MPNs) • Polycythaemia Rubra Vera (PRV) • Essential thrombocythaemia (ET) • Myelofibrosis (IMF) • CML, CNL, Mastocytosis

What are MPNs? • Myeloproliferative diseases - WHO reclassified as Myeloproliferative neoplasms “MPN” in 2008 • PRV, ET • • Bone marrow makes too many red cells, white cells or platelets • Blood becomes too viscous • Problems with blood flow and risk of clots IMF • scarring in the bone marrow - anaemia

What causes MPNs? • We don’t know why an individual is affected. • Single stem cell “transforms” • • Acquired mutations in genes that code for a “kinase” • • grows out-with normal controls JAK 2, CALR, MPL All MPNs can transform to acute myeloid leukaemia or myelofibrosis

Symptoms of MPNs • Many people have no symptoms - incidental finding • Fatigue, Bone pain, Itch or Sweats • Symptoms of sluggish blood flow (PRV/ET) • Discolouration or pain in fingers/toes, thrombosis • Headaches, dizziness, visual disturbance, stroke • Chest pain, breathlessness, angina/MI • Symptoms of anaemia (IMF) • Enlarged spleen and liver - abdominal distension

Why do we treat MPNs? • To reduce symptoms • To reduce the risk of clots • To improve anaemia (IMF) • Treatments do not alter the risk of transformation to AML or IMF

How do we treat MPNs? • Depends on the individual patient, their symptoms and their risk of clots • Reduce clot risk (PRV and ET) • Venesection (Aim for HCT <0. 45) • Anti platelet medication (aspirin, clopidogrel) • Blood thinners if had a clot (warfarin, rivaroxaban) • Drugs that reduce cell numbers

Venesection • Target HCT <0. 45 • Cardiovascular Events and Intensity of Treatment in Polycythemia Vera (Marchioli et al NEJM 2013) • Each venesection –usually approx. 450 mls • At initial presentation - 1 -2 weekly procedure • Limited by patient tolerance • Maintenance usually 2 -3 monthly venesection • Works by haemodilution and iron depletion

How do we treat MPNs • Not everyone needs drugs to reduce cell numbers • “High risk” - >60 yrs, other cardiovascular risk factors eg. hypertension, smoking, diabetes, previous clots, very high platelet count • “Low risk” ET patients can be monitored (watch and wait) • IMF - Blood transfusion and/or drugs to improve Hb and reduce size of spleen

Drugs for MPNs • All drugs control the diseases NOT cure • All drugs require regular blood monitoring (FBC) • Can reduce red cells, white cells and platelets

Hydroxycarbamide • First line treatment -daily capsules • Usually very well tolerated • Side effects • • Diarrhoea, abdo pain • Leg ulcers • Long term use - increased incidence of non-melanoma skin cancers - use sunblock! Avoid pregnancy when on this drug!
 • Side effects")
Anagrelide • Twice daily tablets • Works mostly on platelets (ET) • Side effects • Headaches • Palpitations • Fluid retention • GI effects -diarrhoea, nausea • Rash
 • Side effects • Flu-like symptoms •")
Peg-interferon alpha • Weekly subcutaneous injection (Pegasys) • Side effects • Flu-like symptoms • Dizziness • Diarrhoea, nausea, abdo pain • Rash • Depression • Monitor thyroid function • Safe in pregnancy • Can induce molecular responses
")
JAK 2 Inhibitors • Licensed for IMF and PRV (Intolerant or resistant to hydroxycarbamide) • Ruxolitinib - twice daily tablet • Good at treating symptoms of MPNs Sweats, itch • • Side effects • Dizziness, headache • GI symptoms, monitor liver tests • Worsening of blood counts – infections (UTIs)
 • Anaemia and hepatosplenomegaly • Symptoms of weight loss, fatigue, sweats •")
Myelofibrosis (IMF) • Anaemia and hepatosplenomegaly • Symptoms of weight loss, fatigue, sweats • Anaemia • • • Blood transfusion • Erythropoietin (EPO) • Thalidomide/danazol/prednisolone/peg-interferon Splenomegaly • Hydroxycarbamide/ JAK 2 inhibitors • Splenectomy Bone marrow transplant can be curative

MPNs • PRV/ET/IMF • Treatment individualised to each patient • Aims to reduce MPD symptoms and risk of clots • Treatments control but don’t cure diseases • Risk of transformation to acute leukaemia or myelofibrosis
 • Average diet contains 10 -20 mg iron • Absorbed in")
Haemochromatosis (Iron metabolism) • Average diet contains 10 -20 mg iron • Absorbed in the proximal duodenum • Only 1 -2% of non-haem iron is absorbed - by DMT 1 • About 20% of heme iron (from blood) absorbed - mechanism uncertain

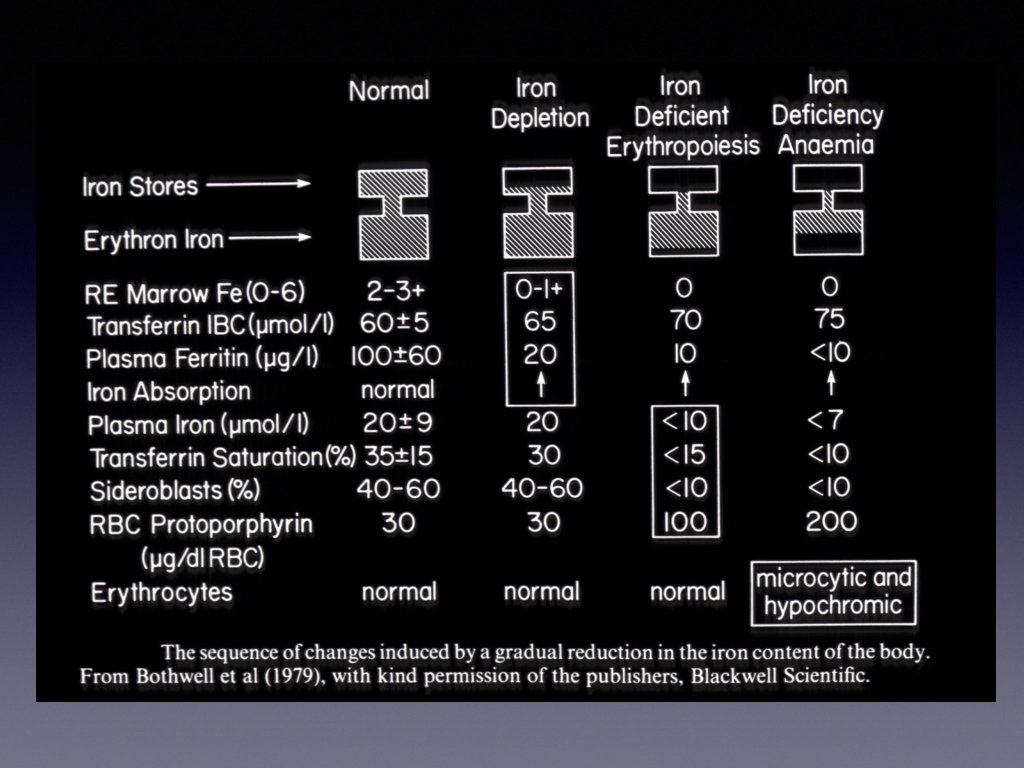
Absorbed iron – bound to mucosal ferritin and sloughed off Or - transported across the basement membrane by ferroportin Then - bound to transferrin (2030% saturated) Transferrin production increases in iron deficiency and decreases in iron excess

Iron metabolism • Stored as ferritin - high concentration in liver, spleen and marrow macrophages (or haemosiderin) • Haemosiderin is denatured, insoluble ferritin • Serum ferritin – only a tiny amount in serum • Proportional to body iron stores • Doesn’t contain or transport iron

Iron metabolism Most of the body’s iron is in Haemoglobin and is “recycled” Normally, dietary intake balanced by loss – shedding of intestinal cells

Iron Overload • Hereditary Haemochromatosis: excessive absorption of iron from GI tract • • Leading to iron overload of the liver, endocrine organs, heart, skin, arthropathy Most common gene: HFE

Hereditary Haemochromatosis • Type 1 • Mutations in HFE gene - C 282 Y, H 63 D, S 65 C • C 282 Y heterozygotes -10 -15% of Caucasian population • C 282 Y Homozygotes- 90% of cases • C 282 Y/H 63 D compound heterozygotes may iron load

Treatment - venesection Each unit 450 -500 ml venesected removes 200 -250 mg iron American and European guidelines only recommend keeping ferritin <50 ug/l and don’t measure transferrin saturation UK guideline – serum ferritin<50 %transferrin saturation<50

Venesection in haemochromatosis • Initially 1 -2 weekly to get elevated ferritin to target <50 ug/l • Limited by patient tolerance and development of anaemia • Monitor progress with FBC and ferritin check every month in initial phase (more often if patient has symptoms suggestive of anaemia) • Maintenance –to keep ferritin >50, %TFsat <50% • Usually approx. 3 monthly venesection • Can be blood donors (referral form for SNBTS)

If in doubt – feel free to ask! louise. forrest 2@nhs. net beverley. robertson@nhs. net donnaj. donaldson@nhs. net
- Slides: 27