Mycology By D Mohammed Sayed Mohammed Ass Prof


Mycology By D/ Mohammed Sayed Mohammed. Ass. Prof. of microbiology and immunology. Faculty of Medicine- Minia University.

l The fungi are very large number, there are more 50. 000 species , only few hundred that can cause disease to human. l The infection may be exogenous or endogenous with lowering of immunity as candidiasis. l The study of fungi called mycology while disease caused by it called mycoses.
 According to growth. 2) According to clinical")
Classification: It can be classified into 1) According to growth. 2) According to clinical manifestation. 3) Medically important fungi.
 According to growth : It can grow into 3 basic forms: l (A)")
1) According to growth : It can grow into 3 basic forms: l (A) Mold: - growth in mold form produce multicellular filamentous colonies. l The colonies formed of hyphae (branched cyclindes tubules), the mass of interwind hyphae are called mycelium. l Some hyphae divided into cell by septa at regular interval at their growth and some species are not sepetated as zygomycetes. l

Vegetative or substrate hyphae penetrate the medium and absorb nutrients while aerial hyphae project above the surface of mycelium and bear the reproductive structure of mold. l (B) Yeast: It is single cell, reproduce by budding, sometimes the buds can not detached and then elongated and when the process continue, peudohyphae will produced. Yeast colonies is cream coloured, soft and opaque. l (C)Dimorphic : Grow as hyphae at 25 and Yeast at 37 l

In addition to their growth as vegetative, the fungi can grow as spore that may be sexual or asexual. l The sexual spores are genetically identified, the fungi can produce two major asexual spore that are: l 1 - Conidia l 2 - Sporangiospore. l

Pseudohyphae
 According to clinical manifestation Types of mycosis Causative agents Mycosis Superficial Malassazia Furfur")
2) According to clinical manifestation Types of mycosis Causative agents Mycosis Superficial Malassazia Furfur Exophiala Werneckii Pityriasis versicolor Tinea nigra Cutanaeous Microporum species Trichophyton species Candida species Dermatophytes Subcutaneous Candidiasis Sporothrix Schenckii Sporotrichosis Phialophora Verrucosa Chromoblastomycosis Pseudollescheria Mycetoma

Cont. Systemic Coccidiodies Immitis Histoplasma Capsulatum Blastomyces Dermatitis Coccidioidomycosis Histoplasmosis Blastomycosis Opportunistic Candidia species Cryptococcus neoformans Aspergilles fumigatus Systemic candidiasis Cryptococcosis Apergillosis But, these classification show some overlap because systemic mycosis may show subcutaneous manifestation and usually systemic and opportunistic mycosis occur in immunocomprised patients.

Diagnosis: 1 - Sample: that is according to the site of infection. Skin, hair or nail scrapings suspected to contain dermatophytes or pus from a lesion can be mounted in KOH to dissolve keratin and examined directly under the microscope

2 - Staining: Gram stain or fungal stain 3 - Culture: grown on Sabouraud dextrose agar cyclohexamide, penicillin, streptomycin or other inhibitory antibiotics are often added to prevent bacterial contamination and overgrowth

4 - Skin test 5 - Serology : The most common serological tests for fungi are based on latex agglutination, double immunodiffusion, complement fixation and enzyme immunoassays. 6 -Histopathology 7 -PCR may be used

Treatment: l l l Amphertcin B Flucytosine Azoles Griseofulvin Topical antifungal as nystatin.
 l l Cutaneous Mycoses It is superficial infection of keratinized tissues as hair,")
I) l l Cutaneous Mycoses It is superficial infection of keratinized tissues as hair, skin or nails Morphology: It is classified into 3 genera ( Microsporum, Trichophyton and Epidermophyton) and on their growth it produce hyphae.

l Pathogenesis: It is usually chronic infection and enhanced by certain conditions. l C/P: 1 - It differ according to the site of infection ( tinea pedis, tinea corporis, tinea capitis, favus) 2 - In case of infection of the scalp, in case of microsporum, called ectothrix, while in case of Trichophyton, called endothrix.

 Specimen: Hair, skin or nails. 2) microscopic examination : with 10%")
l Diagnosis: 1) Specimen: Hair, skin or nails. 2) microscopic examination : with 10% KOH to help the diagnosis by digesting keratin 3) culture: on sabourad dextrose agar at room temperature and the growth take about 1 - 3 weeks. l Treatment: Removal of the hair or nail topical antifungal drugs and systemic antifungal may be used.

II Opportunistic Mycoses l Usually the infection occur when the immunity is lowered and some of the fungi that cause opportunistic infection are endogenous and present as normal flora as in case of candidia while some infection is acquired from the outside.
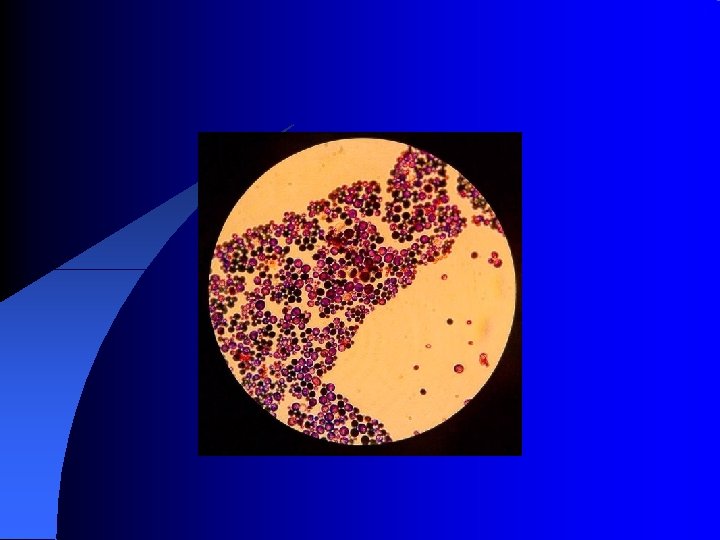
 candida and related yeasts: l It is yeast budding cells with bud fail")
A) candida and related yeasts: l It is yeast budding cells with bud fail to detach give what is called pseudohyphae. l There are many species as Candida Tropic, Candida Kruse. Candida globrata and Candida albicans. l There are 3 tests differentiate Candida albicans: 1) Germ tube test. 2) On nutritionally deficient media, it produces chylamdospore. 3) Sugar fermentation test.
 Cutaneous and mucosal candidiasis: - as oral thrush , vulvovaginal")
l C/P: - 1) Cutaneous and mucosal candidiasis: - as oral thrush , vulvovaginal candidiasis, cutaneous candidiasis and cutaneous candidiasis 2) systemic candidiasis: 3) Chronic mucocutaneous candidacies: -
 Specimen: According to the site of infection. 2) Microscopic examination")
l Laboratory diagnosis: 1) Specimen: According to the site of infection. 2) Microscopic examination : 3) Culture: On sabourad dextrose agar 4) Serology : limited use Treatment: 1 - For cutaneous : topical nystatin, ketaconazole or flucocgnazale 2 - For systemic : Amphthercin B is effective or oral flucocystine 3 - For chronic mucocutaneous: ketaconazole is effective
 Cryptococcus neoformans l This is yeast budding cell with capsular polysaccharides, the reservoir")
B) Cryptococcus neoformans l This is yeast budding cell with capsular polysaccharides, the reservoir is pigeon Morphology: - It is yeast budding cell surround by thick capsule. l Pathogenesis: - Following inhalation, pulmonary infection may be: - Asymptomatic - flu like disease - spread to other organs as C. N. S.

C/P: The main and major clinical presentation is Cryptococcus meningo-encephalitis in which there are elevation of pressure, proteins, cell count and sugar is low or normal Diagnosis: 1) Specimen: According to the site of infection (sputum, urine, C. N. S. ). 2) Microscopic examination: 3) Culture: On sabourad dextrose agar. 4) Serology: test for capsular polysaccharide by latex agglutination
 Aspergillosis It is caused by variety of aspergillus that are of many strain,")
C) Aspergillosis It is caused by variety of aspergillus that are of many strain, but A. fumigatus is the commenst but there also A. flavus, A. niger and A. terrus usually the infection occur after inhalation of conidia. Pathogenesis: l Follow inhalation, conidia germinate to hyphae if the immunity is lowered and hyphae invade the pre exiting pulmonary cavity or blood vessels. l
 Allergy 2) Aspergilloma 3) Invasive aspergillosis l Invasion of blood vessels")
l. C/P: 1) Allergy 2) Aspergilloma 3) Invasive aspergillosis l Invasion of blood vessels lead to thrombosis and infraction. l From lung, infection may spread to distant organs as GIT, kidney , brain or liver. l Usually the predisposing factors are immunosuppressions
 Specimen: According to the site of infection. 2) Microscopic examination")
l Diagnosis: - 1) Specimen: According to the site of infection. 2) Microscopic examination 3) Culture: On most fungal media within few days with the characteristic conidia. 4) Serology: ID of precipitin is positive in 85% of case with allergy. l Treatment: - Usually combination of amphertcin B and surgery in aspergilloma

Actinomycetes l It is gram positive bacilli arranged in chain or filament related to Corynebacterium, mycobacterium as well as streptomycetes. l It is saprophytic and tend to cause 3 disease : - Actinomycetoma - Actinomycosis - Nocardiosis
 Actinomycosis l Chronic suppurative and granulomatous lesion. l The lesion formed of sinus")
A) Actinomycosis l Chronic suppurative and granulomatous lesion. l The lesion formed of sinus tract that contain granules. The granules composed of bacteria embedded in tissue. The most common causative organisms are: - A. Israeli. - A. naeslandii Pathogenesis : l Bacteria induce inflammatory reaction and spread may occur by sinus formation and contain granules.
 cervicofacial: - in jaw region")
l C/P: - Usually there are 4 C/P: 1) cervicofacial: - in jaw region that become fluctuant and fistula may formed 2) thoracic 3) abdominal 4) genital: - rare and can occur in female with IUD
 By demonstration of silver granules that is hard and club shaped")
l Diagnosis: 1) By demonstration of silver granules that is hard and club shaped from pus or exudates of sinus. 2) Culture anaerobically on thicoglycallate or brain heart infusion. 3) The main pathogenic agent of actinomycosis is catalase negative while other actinomycetes are catalase positive Treatment: Prolonged treatment with penicillin is useful, clindamycin and erythromycin may be effective.
 It is a chronic granulomatous lesion that")
l l l Mycetoma ( Madura foot) It is a chronic granulomatous lesion that affect the subcutaneous and deep tissues and the foots and hands are commonly affected This result from trauma that introduce the organism into the tissues. The lesion composed from supporting abscess, granulomata and draining sinus that full of exudates that are characteristic to the etiological agents.

l Etiology: 1 - Fungi: as Madurella mycetomatis and Madurella grisea 2 - Actinomycetes as Nocardia Brasiliensis l Diagnosis: 1 –Examination of the granules in which the black granules are common in fungus while in bacterial cause the granules are red and yellow 2 –Microscopic examination for fungal hyphae 3 - Culture on brain heart infusion agar. Treatment: Fungal cause respond to antifungal drugs while the bacterial cause respond to antibiotic

- Slides: 35