Mushroom Poisoning Myth History and Medicine John D


 marries his niece Agrippina who serves him Amanita")


 was")
 for food and")

 ate")








, glutinous (slimy), dry, smooth, scaly, fibrillose or")













































- Slides: 64
Mushroom Poisoning Myth, History and Medicine John D. Halamka MD
Goals • How to consult a mycologist • Recognizing the symptoms of mushroom poisoning • Current treatment strategies • Recognizing selected mushroom species
Roman History • Claudius (AD 54) marries his niece Agrippina who serves him Amanita Phaloides, Nero ascends to the throne • Pope Clement VII excommunicates Henry VIII. Pope is fed Amanita Phaloides and dies
Indo-European History • First written record of mushroom use. Of 1028 Hindu Vedas (1500 -1200 BC), 120 mention Amanita Muscaria to visualize the gods and improve spiritual vitality
Mesoamerican History • Over 400 religious mushroom stones have been found in Mayan excavations. • Use of Psilocybe species by Chignahuapan Indians first described in Life Magazine in 1957 and inspired the fascination with psychedelics in the 1960’s
Japanese History • Japanese were first to agriculturally propagate fungi. Lentinus edodes (Shitake) was domesticated in 100 BC • Haiku - “I forgot falling off a horse with the happiness of finding Mushrooms” Anon 2000 BC
Chinese History • The Chinese have used Ganoderma species (polypore mushroom) for food and medicine for 5000 years
Russian History • The Siberians of the 1415 th Century collected Amanita Muscaria as the intoxicant of choice until Vodka was invented in the 16 th Century. Siberian peasants also invented mushroom “recycling”
Russian History • Tsar Alexis and his wife (parents of Peter the Great) ate Amanita Phalloides and died on January 25, 1694. Peter ascended to the throne and changed the course of history.
European History • German Emperor Charles VI was fatally poisoned by Amanita Phalloides • Mushroom propagation was invented in the Western world by Louis XIV’s agronomists in the 17 th Century
English History • Sir Arthur Conan Doyle wrote “the fields were spotted with monstrous fungi of a size and color never matched beforesarlet and mauve and black- it was as though the sick earth has burst into foul pustules. ”
English History • Emily Dickinson wrote “Had nature any outcast face, could she a son condemn, had nature an Iscariot, the mushroom - it is him. ”
The New American Attitude • The Boonville Times reports “Deputy Mason responded to reports of a woman screaming near the Branscomb Road turnoff. The distressed woman turned out to be a mushroom hunter, screaming with delight at each new find. ”
Mushroom cuisine • Soak one dozen morels in 3/4 cup cream and a tablespoon of dry sherry. Saute a shallot, a clove of garlic and 1/2 cup chopped pecans. Mix in 4 oz goat cheese, fresh nutmeg and stuff the morels. Serve over paste
Typical Mushroom Hunter • Eastern European expert taught by oral tradition who gathers mushrooms to eat • Harvard scientist interested in the ethnobotany of fungi • Tie-dye shirt wearer asking “Do those mushrooms grow around here. . . ”
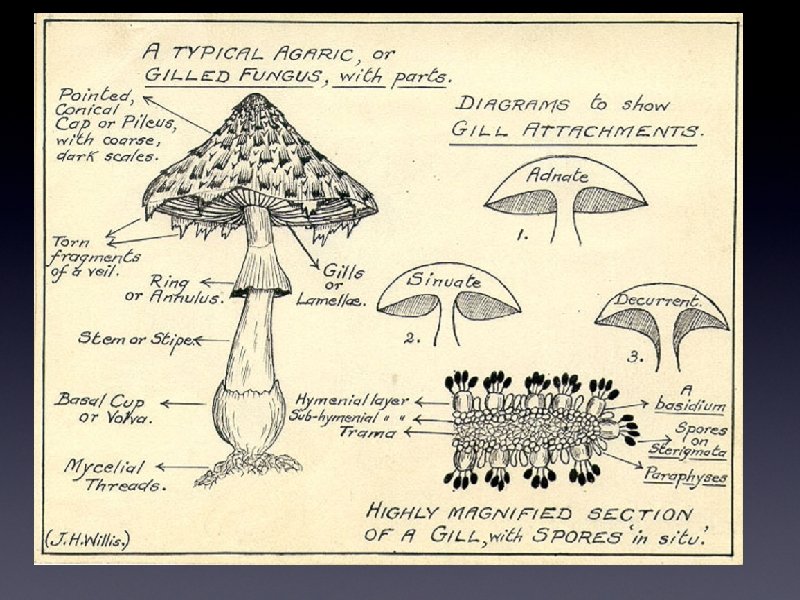
There is no such thing as a Toad Stool
General Morphology • Mushrooms are described by Size, color changes, texture, order, taste, gap, gills, stem/stipe, veil, annulus, volva, mycelium, and spore prints
Cap • Cap descriptions include viscid (sticky), glutinous (slimy), dry, smooth, scaly, fibrillose or warty • Cap margins may be inrolled, incurved, straight, uplifted or striate
Gills • Gills are described by the attachment pattern to the stalk and by spacing, thickness, depth and forking pattern
Stem/Stipe • Stipe features include size, color changes, shape, position, structure, and surface characteristics
Veils and Volva • A veil is residual tissue from mushroom development that is left on the stalk and varies from a few remnants to a complete annulus • A volva is a sack that is found at the base of the stalk
Spore Prints • Spore prints are a very powerful way to identify species of mushrooms. They are created by leaving a mushroom on top of a piece of paper for 2 -6 hours
Consulting a Mycologist • How many people ate the mushroom? • What are their ages and genders? • What was the time from ingestion to symptoms? • Did all the individuals get sick? • Was alcohol consumed? • Were the mushrooms cooked or raw? • Were the mushrooms in good condition?
Habitat Questions • Where were the mushrooms growing? • Were they in a yard, lawn or wild area? • Had pesticides or herbicides been applied? • If trees were nearby, what were they? • Was the mushroom growing on wood, ground or other material? • If wood, was the wood living or dead?
Cap Questions • How big is the cap? • What is the cap color? • Is it smooth, scaly, hairy or sticky? • What is the shape of the cap? • How thick is the cap? • Does the cap change color when it is • cut? What is the total height of the mushroom?
Stem Questions • What is the thickness of the step? • Is it curved or straight? • Is there a ring or veil? • Is there any material at the base of the stem? • Is the surface smooth, scaly or hairy? • Is it hollow? • Does the color change when exposed to air?
Gill Questions • Are there gills on the underside of the cap? • What is the color of the gills? • Are they attached to the stem? • Is there a fine powder on the gills and if so, what color? • If no gills are present, what is the color and texture of the underside of the cap?
Group 1 - Amatoxins • Most difficult to treat. 90% of all deaths due to mushroom poisoning • Species include Amanita Phalloides, Amanita Ocreata, Gallerina Autumnalis • Toxin is stable to cooking, pickling, salting and is not hydrolyzed by digestion • Toxins include amanitins and phallotoxin which inhibit RNA polymerase II • Toxins are resorbed by the distal tubule
Amatoxin Clinical • Delay of 6 to. Effects 12 hours before initial symptoms is common • Sudden onset of sharp, colicky abdominal pain, nausea, vomiting, thirst, bloody stools • Latent period of web being lasting 3 to 5 days • Recurrence of abdominal pain with jaundice, renal shutdown, seizures, coma and death
Amatoxins Treatment • Toxin elimination via repeat dose charcoal • Supportive care with fluids, electrolytes • Penicillin G may displace amanitin from plasma binding sites 300 k-1000 k u/kg/d • Silymarin (from milk thistle) may compete for membrane transport • Liver Transplant
Amanita Phalloides
Amanita Ocreata
Group 1 A - Orellanine • Cortinarius species - over 1000 in the US • Causes severe renal tubular damage resulting in reduced GFR, decreased absorption of water/NA/K, proteinuria, glucosuria • Inhibits RNA and DNA synthesis in kidney cells
Orellanine Clinical Effects • Initial mild gastroenteritis • Long latent period of 36 hours to 17 days • Symptoms include severe thirst, abdominal or flank pain, chills and fever • Progresses to acute renal failure. Chronic failure occurs in 50% of cases • Recovery takes weeks to months
Orellanine Treatment • Standard decontamination • Hemodialysis • Renal transplant • Steroids, hemoperfusion, and forced diuresis do not improve outcome
Group II Muscimol/Ibotenic • Amanita Muscaria, Amanita Pantherina, Acid Amanita Gemmata • Toxin is Ibotenic acid which is metabolized to Muscimol • Muscimol is a false neurotransmitter which acts on GABA receptors and affects brain levels of serotinin, dopamine and noradrenalin. Usually results in anticholinergic symptoms • May present with cholinergic symptoms
Muscimol/Ibotenic Acid • Onset within 30 to 90 minutes, most Clinical Effects marked at 2 to 3 hours • Drowsiness, confusion resembling alcohol intoxication, dizziness, ataxia, euphoria, muscle cramps and spasms, delirium, visual disturbances, hallucinations • Vomiting is rare • Deep sleep or coma terminates the episode which usually lasts from 4 to 8 hours
Musicmol/Ibotenic Acid • Standard. Treatment decontamination measures • Support airway and hemodynamics with standard measures • With life threatening anticholinergic signs, consider physostigmine. 5 to 2 mg slow IVP over 5 minutes • With life threatening cholinergic signs consider atropine
Amanita Muscaria
Amanita Pantherina
Group III Monomethylhydrazine • Gyromitra and Helvella • Toxin is Gyrometrin which is hydrolyzed to MMH at 87. 5 C and only affects the person cooking the mushroom • Toxin chelates pyridoxal phosphate and inhibits reactions where B 6 is a cofactor
Monomethylhydrazine Clinical Effecs • Relatively long latent period of 6 to 12 hours followed by vomiting, watery diarrhea, abdominal pain, weakness and headache. • Severe cases notable for jaundice, tachycardia, hyperreflexia, vertigo, loss of muscle coordination, seizures and coma • Recovery in 2 to 6 days
Monomethylhydrazine Treatment • Standard decontamination measures • For seizures, give B 6 at 25 mg/kg over 15 to 30 minutes IVP. • For methemoglobin levels which are greater than 30% or patients who present with symptomatic hypoxia, give methylene blue 1% solution. 1 -. 2 ml/kg IV over 5 minutes IVP
Group IV - Muscarine • Clitocybe, Omphalotus • Toxin is muscarine which stimulates postganglion parasympathic fibers • Muscarine is very slowly hydrolyzed by acetylcholinesterase
Muscarine Clinical Effects • Onset within 30 to 120 minutes • Excessive perspiration, salivation, lacrimation (PSL symptoms), bradycardia, miosis, blurred vision, increased peristalsis, abdominal pain, and watery stools • Severe cases notable for hypotension, bronchorrhea and wheezing • Recovery in 6 to 24 hours
Muscarine Treatment • Standard decontamination methods • In severely symptomatic presentations consider atropine 1 mg to 2 mg for adults and children • 0 to 2 years. 2 mg • 3 to 4 years. 3 mg • 5 to 10 years. 4 mg
Group V - Coprine • Coprinus atramentarius • Toxin is coprine, the metabolite of which inhibits aldehyde dehydrogenase • Ingestion is asymptomatic unless ethanol is consumed in the following 2 hours to 5 days
Coprine Clinical Effects • Onset of symptoms within 20 minutes to 2 hours after ingestion of alcohol • Symptoms include flushing of the face and neck, swelling an parathesias in the hands and feet, metallic taste, and tachycardia • Late symptoms include nausea, vomiting and sweating • Severe cases include vertigo, weakness, confusion, hypotension and arrhythmias
Coprine Treatment • Decontamination measures if mushroom recently ingested • Symptomatic treatment • B-blockers or sedatives for anxiety and tachycardia • Fluids for hypotension
Group VI - Psilocybin • Psilocybe, Panaeolus, Gymnopolis • Toxins are Psilocybin and its metabolite psilocin • Effects are serotonin and norepinephrine mediated • Blue staining reaction aids identification
Psilocybin Clinical Effects • Onset of symptoms within 30 to 60 minutes, occassionally as late as 3 hours after ingestion of 5 to 15 mg of psyilocybin (10 to 30 g fresh weight of mushrooms) • Symptoms include hallucination, impaired judgement, hyperkinesis, laughter, vertigo, ataxia, muscle weakness and drowsiness
Psilocybin Treatment • Decontamination not recommended as this may increase agitation • Rest and reassurance in a dark, quiet room • Consider benzodiazepines for severe anxiety
Group VII - GI Irritants • Chlorophyllum • Molybdites, Agaricus Xanthodermis, Russula Emetica No specific toxins identified • Most mushrooms cause more symptoms when eaten raw
GI Irritants Clinical Effects • Onset of symptoms within 30 minutes to 2 hours after ingestion • Symptoms include nausea, vomiting, diarrhea and abdominal pain • In severe cases electrolyte disturbances may occur
GI Irritants Treatment • Standard decontamination measures • Be wary of antiemetics and antidiarrheals as these may have unpredictable interactions with mushroom toxins
Epidemoiology • American Association of Poison Control Centers = 9208 cases/year • Group I - Cyclopeptide 61 cases/year • Group III - MMH 57 cases/year • Group VI - Hallucinogens 330 cases/year • Group VII - GI Irritants 202 cases • Minimal effect 10, % moderate 5%, major 1%, death in 3 cases
5 year old • Ingestion of red mushroom • Nausea and vomiting within 2 hours • Given charcoal in local Emergency Department • Now appears well
Russula Emetica
30 year old male • Chardonnay and Shaggy Manes • Nausea/Vomiting 2 hours after dinner • Tachycardia • Hydrated and back to baseline after 6 hours
Coprinus Atramentarius
16 year old male • Magic mushrooms • Unsure of dose • Ate one pound • Required sedation and intubation
Psilocybe Cubensis
Questions • jhalamka@hms. harvard. edu • http: //geekdoctor. blogspot. com