Muscular System BELLRINGER 2315 n What are the

Muscular System

BELLRINGER 2/3/15 n What are the functions of muscles?

Muscles

Types of Muscle Skeletal – Striated – Voluntary – Multinucleated n Smooth – Nonstriated – Involuntary n Cardiac – Striated – Involuntary – Intercalated disks n ~ 50% of body weight Work in groups to perform a function

General Functions of Muscular System n Movement – Skeletal muscle contractions move body in whole or part n Heat Production – Muscle cells produce heat via catabolism to maintain temperature homeostasis n Posture – Continued partial contraction of muscle in order to perform many functions

Characteristics of all Muscle n n Excitability – Respond to stimuli Contractility – Actively shorten to exert a pull – Tension that can be harnessed by CT Extensibility – Continue to contract over range of resting lengths – Ex: smooth muscle can be stretched to several times its original length and still contract on stimulation Elasticity – Return to original length after contraction

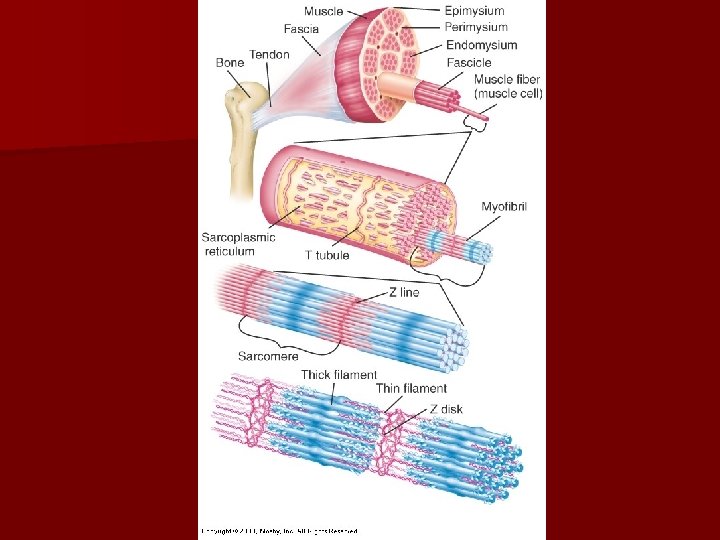
-mysium=CT membrane and tendon sheath

Muscle Fiber Arrangement Parallel Convergent Pennate Bipennate Sphincter

Muscle Attachment Does NOT move when muscle contracts hen w ove racts m t s Doe cle con mus

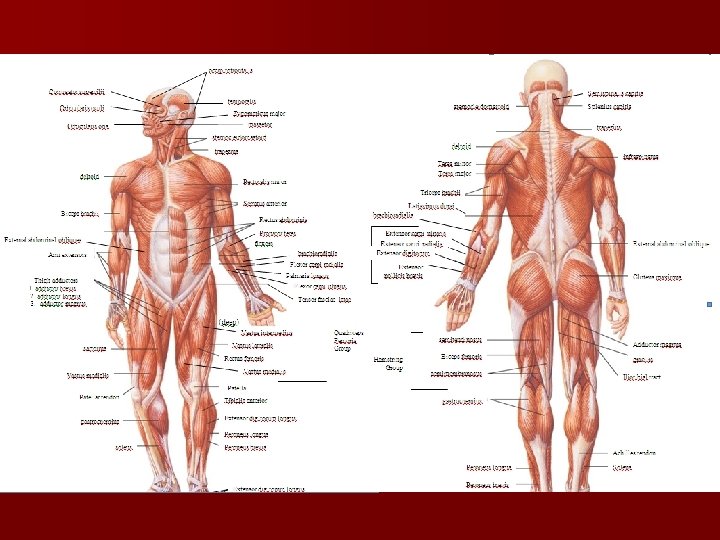
Naming Muscles n Location n Function n Shape n Fiber direction n Number of heads/divisions n Points of attachment n Muscle size

Location Function Frontalis Frontal bone Abductor Moves part away from body Femoris Femur Adductor Moves part toward body Gluteus Posterior of hip/thigh Depressor Lowers a part Oculi Eye Extensor Extends a part Oris Mouth Flexor Flexes a part Radialis Radius Levator Elevates a part Ulnaris Ulna Rotator Rotates a part Brachialis Arm Shape Fiber Direction Oblique Diagonal to midline Deltoid Shaped like delta ∆ Rectus Parallel to midline Orbicularis Circular Sphincter Circling an opening Platy Flattened; platelike Transversus Right angle to midline Quadratus Square Rhomboideus Diamond-shaped Trapezius Trapezoidal

Number of divisions Bicep Two heads Tricep Three heads Quadricep Four heads Size Brevis Short Longus Long Magnus Large Maximus Largest Medius Moderately sized Minimus Smaller

Raises eyebrows Frowning Mastication Blinking Laughing Whistling, smiling Puckering Mastication Flexes head

Moves head Flexes head

Superficial Back Muscles • Large, fan-shaped muscles provide force in a wide range of body positions -EX: leaning back to straight vertical and all points in between. Shrugging, pulling scapulas together and down Shoulder movement Pull the arm down, Stabilize torso during many movements (EX: bench press) Rotator cuff muscles Stabilize shoulder joint, pull arm back

Trunk Muscles - Thorax Elevate ribs

Trunk Muscles Abdomen Flexes trunk Rotates abdomen Stabilizes Lower back

Upper Arm Extends forearm Flexes Upper arm

Flexors

Extensors

Upper Leg Deep muscle Vastus intermedius Biceps femoris Quadricep Femoris Semimembranosus Semitendinosus

Lower Leg Plantar flexion

Foot

Anal and Urogenital Muscles

Posture n Good Posture – body alignment that favors function with least work – Standing Position § § Head and chest held high Chin, abdomen, buttocks pulled in Knees slightly bent Feet firmly on ground 6 in. apart n Poor Posture - puts abnormal strain on ligaments and bones n Maintenance – Tonicity (muscle tone): muscles exert a pull against gravity § Continuous and passive partial contraction of muscles
: 1. Prime mover")
Bellringer 2/24/15 Define the following (p. 200 in textbook or notes): 1. Prime mover (agonist) 2. Antagonist 3. Synergist 4. Fixator FYI-Disease Diary Due Monday. Test next Wednesday (3/4/15)
 – Muscle most responsible for movement")
Classification of Muscle Group Actions Agonist (Prime Mover) – Muscle most responsible for movement n Antagonist – Opposes prime mover – Provides precision and control during prime mover contraction – Relaxes when prime mover contracts n Synergist – Aid prime mover – Contract at same time as prime mover n Fixator – Joint stabilizer – Maintains posture/balance during prime mover contraction n

n https: //www. youtube. com/watch? v=4 t 2 X 2 Iv. Gy. UE

L e v e r S y st e m s 1 st Class 2 nd Class 3 rd Class P = Force (push or pull) Contracting Muscle F = Fulcrum Joint L = Load Weights, etc

Get to know the muscles n Using your textbook, label the muscles on the handout.

Muscles & Age n Infancy & Childhood – Muscle coordination and control allows developmental sequences to occur n Aging – Muscles degenerate with age § Replaced with CT

Bellringer 2/4/15 n What is the name of the large superficial calf muscle? n What is the name of the muscle that raises your eyebrows? n What is the name of the muscle that allows you to blink? HW CHECK

Muscle Contraction n https: //www. youtube. com/watch? v=BMT 4 Pt. XRCVA
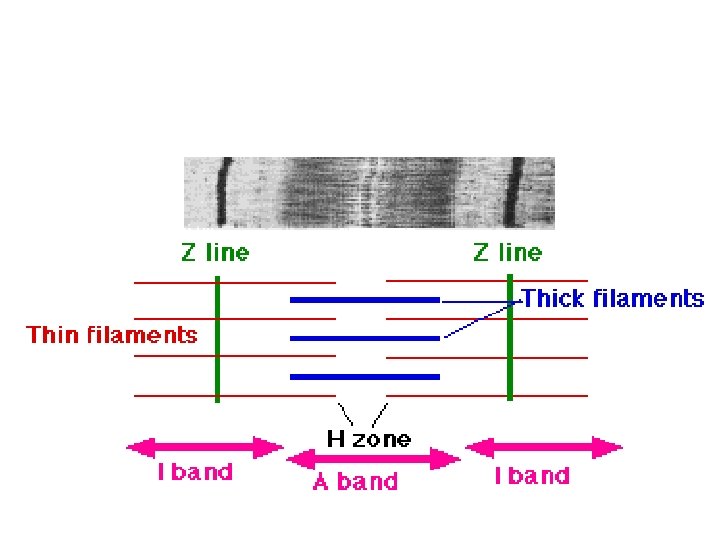
 cytoplasm Basic contractile unit of muscle fiber H zone Space between")
Muscle cell (fiber) cytoplasm Basic contractile unit of muscle fiber H zone Space between actin Sarcoplasm Z line Muscle fiber membrane I band Z line A band Bundle of microfilaments; almost fill sarcoplasm Length of myosin heads (wide, dark stripes) Allows impulses to travel along sarcolemma deeper into muscle cell (fiber) Length of actin (thin, light stripes) Network of tubules and sacs: pumps calcium ions in from sarcoplasm to store in sacs Allows impulse traveling down T tubule to stimulate adjacent sacs

http: //highered. mcgrawhill. com/sites/0072495855/student_view 0/chapter 10/animation__sarcomere_c ontraction. html

Myofilaments protein molecules Holds tropomyosin in place Covers active site on actin Attracted to actin and forms crossbridge http: //highered. mcgraw-hill. com/sites/0072495855/student_view 0/chapter 10/animation__breakdown_of_atp_and_crossbridge_movement_during_muscle_contraction. html

Contraction http: //highered. mcgrawhill. com/sites/0072495855/student_view 0/chapter 10/animation__action_potentials_an d_muscle_contraction. html tropomyosin 1. 2. 3. 4. 5. 6. 7. 8. 9. troponin Synaptic vesicle travels down motor neuron and binds to motor endplate Acetylcholine released into synaptic cleft Ach binds to receptor on sarcolemma Impulse travels along sarcolemma and down t-tubules Calcium released from sarcoplasmic reticulum Calcium binds to troponin causing conformation change tropomyosin shifts to expose active site on actin myosin heads bind to actin filaments are pulled past the myosin head; head unattaches and reattaches to a new site…. repeat Sliding Filament Theory - sliding of thin filaments toward center of each sarcomere shortens the myofibril and muscle fiber.

Excitation & Contraction Impulse sent to muscle fiber Muscle fiber creates movement Synaptic cleft Motor endplate Synaptic vesicle Neuromuscular junction (neurotransmitter) http: //highered. mcgrawhill. com/sites/0072495855/student_view 0/chapter 10/animation__function_of_the_neuromuscular_junction __quiz_1_. html

Motor Unit Smaller # fibers – more precise movement Larger # fibers – more powerful contraction

SR releasing Ca+2 bind to troponin; Cross-bridging All or NONE • Quick jerk due to brief threshold stimulus • One twitch – 1/10 sec • Rarely occur • Gradual, step-like increase in contraction strength • Series of twitch contractions 1 sec apart • Muscle contracts more forcefully after it has contracted a few times, then when it first contracts • Warm-up before exercise • Smooth, sustained contractions • Coordinated contractions of different motor units • Multiple twitch waves add together to sustain muscle tension for longer time • Very short periods of relaxation between peaks of tension • Twitch waves fused into a single, sustained peak

Tonicity n Continual, partial contraction of a muscle n Flaccid – Muscles with less tone than normal n Spastic – Muscles with more tone than normal

Length-tension Relationship Optimal length Strongest max contraction possible Overstretched Sarcomere compressed Muscle can’t develop tension due to filaments too far apart

Energy Sources ATP – Hydrolysis into ADP yields energy required for contraction – ATP binds to myosin head in order to pull actin – Fibers continually resynthesize ATP from breaking down creatine phosphate (requires glucose and oxygen) n Glucose & oxygen – Hemoglobin transfers O 2 to muscle fiber – Fiber stores glucose as glycogen – At rest: Excess O 2 in sarcoplasm is bound to myoglobin temporarily – Exercise: O 2 concen. Decreases in muscle, so myoglobin resupplies muscle with O 2 n

Respiration n Aerobic Respiration n Anaerobic Respiration – Requires O 2 – Produces max amount of energy available from each glucose molecule – Occurs when lack of O 2 – Forms lactic acid § During exercise § Muscles “burn” – O 2 debt § Heavy breathing during exercise in order to process lactic acid

Muscle Fatigue n Muscles loses ability to contract due to lack of ATP n Suspected imbalance of ions n Problems at the neuromuscular junction n Lactic acid build up n Cramp – muscle contracts spasmodically, but does not relax completely

Most body movements are a result of both types

Change in Muscle Size n Atrophy – decrease in muscle size – Bed Rest: lose 1% muscle strength/day n Hypertrophy – increase in muscle size

Myopathies n n n Myalgia - muscle pain due to overstretching/tearing of muscle fibers Fibromyalgia – widespread muscle and CT pain Strain – caused by overexertion/trauma and can lead to muscle tear Myositis - any muscle inflammation Fibromyositis - tendon inflammation along with myositis Cramps – Painful muscle spasms – Due to mild myositis, fibromyositis, irritation, iron, and water imbalance – Charley Horse § Intense muscle spasms § Last few seconds to few hours § Caused by injury or overuse – Dehydration – Low K+ or Ca+2 – Nerve irritated § Treatment – Stop activity – Stretch and massage – Heat to relax muscle – Ice when spasm is over
 n Muscular Dystrophy n Myasthenia Gravis – Muscle")
Myopathies n Contusion n Poliomyelitis (Poilio) n Muscular Dystrophy n Myasthenia Gravis – Muscle bruise, local internal bleeding and inflammation – Crush injury: severe trauma to muscle, releasing fibers into bloodstream (life threatening) – – – Viral infection of nerves controlling skeletal movement Causes partial or full paralysis and death Vaccine created in US in 1950 s, but not everywhere – – – Genetic disease caused by muscle atrophy Some forms are fatal Most common form is Duchenne Muscular Dystrophy (DMD) – – Autoimmune disease that attacks muscle cells at NM junction Muscle weakness Can become a crisis and affect all four limbs Could die of respiratory failure

n Hernias – – – Myopathies “protrusion” Reducible – can manipulate protruding organ back into abdominal cavity Strangulated – blood flow to organ is stopped; obstruction, gangrene, pain. Vomiting, emergency surgery – Types § Inguinal – hernia extends into inguinal canal into scrotum or labia; affects more males § Femoral – affects more women below groin area due to pregnancy

Classwork n P. 223 #16 -24
- Slides: 54