Multivessel Stenting With Anomalously Arising Culprit Vessel Tackled










- Slides: 13
Multi-vessel Stenting With Anomalously Arising Culprit Vessel Tackled Successfully in ACS Dr. Arvind Kandoria Professor, Department of Cardiology, Indira Gandhi Medical College, Shimla.
• Mr. LS, 50 yrs/Male, k/c/o HTN, CAD, AOE-II, DVD, smoker, dyslipidemic, non diabetic, no FHO CAD, presented with ACS/NSTEMI(Inferior wall MI) X 1 day duration with ongoing pain chest in spite of maximum anti anginal therapy. • BP 110/84 mm Hg. Pulse Rate 76/min. , regular, APPP • Blood biochemistry including lipid profile – WNL • Troponin I – Positive • Echo – RWMA in RCA territory with EF around 55%.
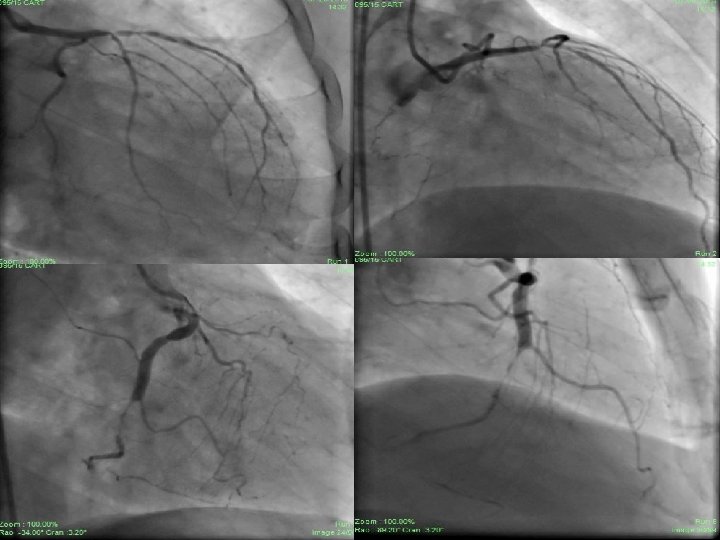
• CART done prior to ACS suggestive of DVD – Anomalous RCA from non-coronary sinus with oval orifice with acute angulation, proximal RCA – 40% stenosis and distal RCA – 99% stenosis with grade III inter coronary collaterals. • LAD having bifurcation lesion (1, 1, 1) with maximum 95% stenosis involving proximal, mid LAD and D 1. Distal LAD – 60% stenosis with grade I collaterals from RCA. • Right dominant circulation.
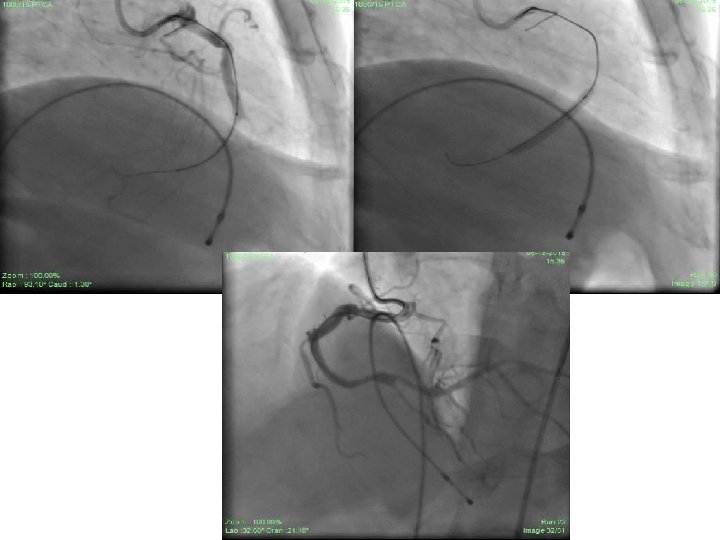
• Patient was taken up for PCI to RCA and LAD through RFA access under TPI. • RCA hooked initially with JR 3. 5/6 F guiding catheter then AL 1/6 F guiding catheter. • Lesion finally crossed with Miracle-3 wire using balloon support. • Lesion dilated with 1. 25 X 8 mm CTO balloon and 2. 0 X 15 mm Sprinter Legend balloon. • Xience-V 2. 75 X 28 mm stent deployed successfully in distal RCA with normal flow through and beyond stent. • TIMI – III flow achieved. • 50% residual stenosis remained distal to stent at crux and PLV.
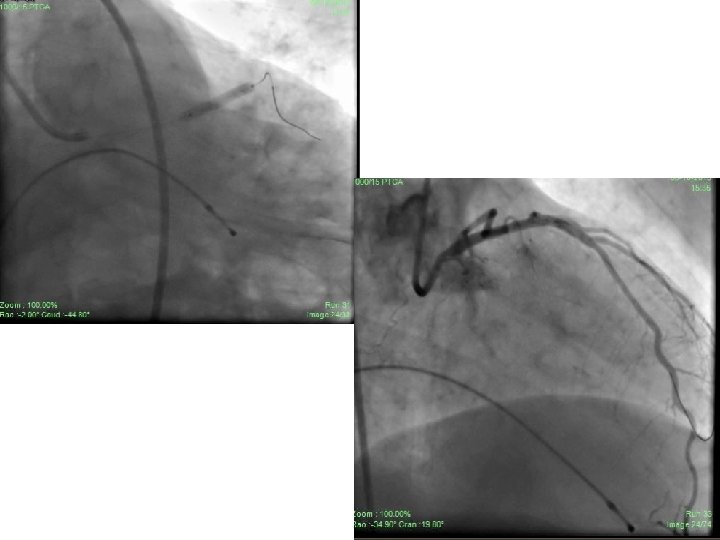
• In the same sitting, bifurcation lesion in LAD was tackled. • Using JL 3. 5/6 F guiding catheter, lesion crossed with BMW guide wire in LAD (D 1 could not be entered in spite of repeated attempts). • Angioplasty to LAD done with 2. 0 X 15 mm S. L. balloon. • Xience-V, 2. 75 X 23 mm was deployed in LAD. • D 1 was pinched with TIMI – I flow though there was normal flow through and beyond stent in LAD with TIMI –III flow. • Intra- coronary bolus and i. v. infusion of Tirofiban was used. • Patient was pain free and no ECG changes were seen. • Discharged on day 3 from hospital and continued on conventional anti anginal therapy.
• Check angiography done after 2 months showed normal flow through and beyond stents with TIMI – III flow (both RCA and LAD stents). • Proximal RCA – 40% stenosis, Crux and PLV - 50% stenosis with D 1 showing TIMI – III flow.
Take Home Message • Anomalously arising coronary arteries, if have slit like orifice, or acute angulation, or if they run between aorta and RVOT definitely have more malignant outcome. • These are more prone to atherosclerosis than normally arising coronaries. (CASS Registry) • The possibility of anomalous coronaries should always be kept in mind while performing PCI and necessary hardware must be available in dealing such situations. • If small caliber side branch gets compromised without signs and symptoms during PCI, it should be managed conservatively.