Multiple ORAL Dosing Objectives Calculate Concentrations following multiple

Multiple ORAL Dosing Objectives Calculate Concentrations following multiple doses Evaluate methods of predicting conc. at SS following oral doses Evaluate changes in Tmax as SS approaches Evaluate Sustain Release formulations

Multiple Dosing Summary … so far – IV dosing We have seen that: 1. [ ] following single doses can be Summed to create MD profile (Additivity of [ ]) 2. At Steady State In (Dose) = Out (elimination) 3. MAF, predicts the degree of accumulation (K and τ) 4. (1/1 -e(-Kτ)), converts a single dose equation to multiple dose 5. (1 -e(-n. Kτ))/(1 -e(-Kτ)) allows Calculation of [ ] at any time 6. Time to Reach steady state determine by K (Cl/V) -3. 3 T½ 7. AUC(0 -τ) over a dosing interval @ SS = AUC(0 - ) 1 st dose. 8. Just as AUC(0 - ) 1 st dose can be use to estimate bioequiavalence so can AUC(0 -τ), as long as you are at steady state (min 3 T½ dosing). 9. Using MAF we can design an IV dosing regimen that will achieve desired peak and trough concentrations at SS. 10. At Steady state all other parameters remain unchanged (Cl. R, Cl. H, proportion metabolised. )
 0 0.")
Multiple ORAL Dosing – through addition of single dose concentrations Time (hr) 0 0. 5 1 1. 5 2 4 6 8 16 24 32 40 Conc (mg/L) 0. 00 61. 6 81. 7 86. 6 86. 0 73. 9 62. 1 52. 3 26. 1 13. 1 6. 5 1. 6 Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; T½=8 hr; F=1

Multiple ORAL Dosing – through addition of single dose concentrations SD MD Time Conc (hr) (mg/L) 0 0. 5 61. 6 61. 5 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 + 0. 0 = 52. 3 16 26. 1 + 52. 3 = 78. 4

Multiple ORAL Dosing – through addition of single dose concentrations SD MD Time Conc (hr) (mg/L) 0 0. 5 61. 6 61. 5 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 + 0. 0 = 52. 3 16 26. 1 + 52. 3 = 78. 4 24 13. 1 +26. 1 + 52. 3 = 91. 5

Multiple ORAL Dosing – through addition of single dose concentrations SD MD Time Conc (hr) (mg/L) 0 0. 5 61. 6 61. 5 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 + 0. 0 = 52. 3 16 26. 1 + 52. 3 = 78. 4 24 13. 1 +26. 1 + 52. 3 = 91. 5 32 6. 5 + 13. 1 + 26. 1 + 52. 3 = 98. 0

Multiple ORAL Dosing – through addition of single dose concentrations SD MD Time Conc (hr) (mg/L) 0 0. 5 61. 6 61. 5 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 + 0. 0 = 52. 3 16 26. 1 + 52. 3 = 78. 4 24 13. 1 +26. 1 + 52. 3 = 91. 5 32 6. 5 + 13. 1 + 26. 1 + 52. 3 = 98. 0 40 1. 6 + 6. 5 + 13. 1 + 26. 1 + 52. 3 = 99. 6 mg/L

Multiple ORAL Dosing – using the equation Recall that MAF was able to convert the single dose equation to a multiple dose equation Cmax ss 1 ---- = MAF = ------k Cmax 1 1 -e

Multiple ORAL Dosing – using the equation Recall that MAF was able to convert the single dose equation to a multiple dose equation 1 MAF = -----1 - e -K Dose Ct = ----- e-Kt V First Dose Conc. … predicts accumulation 1 x ------ 1 – e -K Accumulation Steady State Equation

Multiple ORAL Dosing – using the equation However, the single oral dosing equation has two exponentials (K and ka) and each will have its own MAF. 1 MAF = ------k 1 -e MAF for ka?

Multiple ORAL Dosing – using the equation, Predicting SS Predicts Concentration-time @ SS

Multiple ORAL Dosing – using the equation, all concentrations Predicts Concentration-time at ANY time following an ORAL dose
 (mg/L) 0 0.")
Multiple ORAL Dosing – using the equation SD Time Conc (hr) (mg/L) 0 0. 5 61. 6 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 16 26. 1 24 13. 1 32 6. 5 40 1. 6 MD Verify 24 hour concentration [Cmin dose 3] Conc Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; (mg/L) T½=8 hr; F=1 0. 0 Dosing Interval 8 hrs and t = 8 hrs. 61. 5 81. 7 86. 6 86. 0 -3*0. 086*8) 2*1*1000 (1 -e 0. 086*8 e 73. 9 Ct= 10*(2 -0. 086) (1 -e-0. 086*8) 62. 1 52. 3 (1 -e-3*2*8) e-2*8 78. 4 -2*8 (1 -e ) 91. 5 98. 0 99. 6
 (mg/L) 0 0.")
Multiple ORAL Dosing – using the equation SD Time Conc (hr) (mg/L) 0 0. 5 61. 6 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 16 26. 1 24 13. 1 32 6. 5 40 1. 6 MD Verify 24 hour concentration [Cmin dose 3] Conc Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; (mg/L) T½=8 hr; F=1 0. 0 Dosing Interval 8 hrs and t = 8 hrs. 61. 5 81. 7 86. 6 86. 0 -3*0. 086*8) 2*1*1000 (1 -e 0. 086*8 e 73. 9 Ct= 10*(2 -0. 086) (1 -e-0. 086*8) 62. 1 52. 3 (1 -e-3*2*8) e-2*8 78. 4 -2*8 (1 -e ) 91. 5 0. 875 1 - 1. 4 x 10 -21 98. 0 Ct = 104. 53 0. 5 - 1 - 1. 1 x 10 -7 0. 499 99. 6
 (mg/L) 0 0.")
Multiple ORAL Dosing – using the equation SD Time Conc (hr) (mg/L) 0 0. 5 61. 6 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 16 26. 1 24 13. 1 32 6. 5 40 1. 6 MD Verify 24 hour concentration [Cmin dose 3] Conc Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; (mg/L) T½=8 hr; F=1 0. 0 Dosing Interval 8 hrs. 61. 5 81. 7 86. 6 86. 0 -3*0. 086*8) 2*1*1000 (1 -e 0. 086*8 -2*8 e 73. 9 Ct= e -0. 086*8 10*(2 -0. 086) (1 -e ) 62. 1 52. 3 Ct = 104. 53 0. 875 0. 50 - 1. 0 0. 000000113 78. 4 0. 499 91. 5 = 104. 53[(1. 75)(0. 5) – (0. 000000113)] 98. 0 = 104. 53 [0. 875 – 0. 000000113] 99. 6 = 91. 46 mg/L
 (mg/L) 0 0.")
Multiple ORAL Dosing – using the equation SD Time Conc (hr) (mg/L) 0 0. 5 61. 6 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 16 26. 1 24 13. 1 32 6. 5 40 1. 6 MD Conc (mg/L) 0. 0 61. 5 81. 7 86. 6 86. 0 73. 9 62. 1 52. 3 78. 4 91. 5 98. 0 99. 6 Calculate Cmin at steady state Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; T½=8 hr; F=1 Dosing Interval 8 hrs. Cdose 3 - 8 hr = 91. 46 mg/L
 (mg/L) 0 0.")
Multiple ORAL Dosing – using the equation SD Time Conc (hr) (mg/L) 0 0. 5 61. 6 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 16 26. 1 24 13. 1 32 6. 5 40 1. 6 Calculate Cmin at steady state MD Conc Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; (mg/L) T½=8 hr; F=1 0. 0 Dosing Interval 8 hrs. and t = 8 hrs 61. 5 81. 7 86. 6 86. 0 2*1*1000 (1) 0. 086*8 -2*8 C = e 73. 9 t 1 e -0. 086*8 10*(2 -0. 086) (1 -e ) 62. 1 52. 3 1 0. 50 - 1. 00 0. 000000113 Ct = 104. 53 78. 4 0. 499 91. 5 = 104. 53[1 – (0. 000000113)] 98. 0 = 104. 53 [1 – 0. 000000113] 99. 6 = 104. 45 mg/L
 (mg/L) 0 0.")
Multiple ORAL Dosing – using the equation SD Time Conc (hr) (mg/L) 0 0. 5 61. 6 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 16 26. 1 24 13. 1 32 6. 5 40 1. 6 MD Conc (mg/L) 0. 0 61. 5 81. 7 86. 6 86. 0 73. 9 62. 1 52. 3 78. 4 91. 5 98. 0 99. 6 Calculate Cmin at steady state Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; T½=8 hr; F=1 Dosing Interval 8 hrs. Cmin. SS = 104. 45 mg/L
 (mg/L) 0 0.")
Multiple ORAL Dosing – using the equation SD Time Conc (hr) (mg/L) 0 0. 5 61. 6 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 16 26. 1 24 13. 1 32 6. 5 40 1. 6 Calculate Cmin at steady state MD Conc Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; (mg/L) T½=8 hr; F=1 0. 0 Dosing Interval 8 hrs. 61. 5 81. 7 86. 6 86. 0 73. 9 62. 1 52. 3 78. 4 91. 5 Cmin. SS = 104. 45 mg/L MAF = 1. 997 98. 0 Cmin 1 = 52. 3 mg/L 99. 6

Multiple ORAL Dosing but will MAF always work following oral absorption? Cmax ss 1 ---- = MAF = ------k Cmax 1 1 -e MAF does not consider ka … could this cause error in the estimation of accumulation? Evaluate initial conditions of: Dose =200; V = 20 L; half-life = 8 hr; ka is varied from 0. 029 to 10 and dosing interval is 8 hours. Cmax and Cmin is calculated for each dose.
 0 0.")
Multiple ORAL Dosing – through addition of single dose concentrations Time (hr) 0 0. 5 1 1. 5 2 4 6 8 16 24 32 40 Conc (mg/L) 0. 00 61. 6 81. 7 86. 6 86. 0 73. 9 62. 1 52. 3 26. 1 13. 1 6. 5 1. 6 Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; T½=8 hr; F=1

Multiple ORAL Dosing – through addition of single dose concentrations SD MD Time Conc (hr) (mg/L) 0 0. 5 61. 6 61. 5 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 + 0. 0 = 52. 3 16 26. 1 + 52. 3 = 78. 4

Multiple ORAL Dosing – through addition of single dose concentrations SD MD Time Conc (hr) (mg/L) 0 0. 5 61. 6 61. 5 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 + 0. 0 = 52. 3 16 26. 1 + 52. 3 = 78. 4 24 13. 1 +26. 1 + 52. 3 = 91. 5

Multiple ORAL Dosing – through addition of single dose concentrations SD MD Time Conc (hr) (mg/L) 0 0. 5 61. 6 61. 5 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 + 0. 0 = 52. 3 16 26. 1 + 52. 3 = 78. 4 24 13. 1 +26. 1 + 52. 3 = 91. 5 32 6. 5 + 13. 1 + 26. 1 + 52. 3 = 98. 0

Multiple ORAL Dosing – through addition of single dose concentrations SD MD Time Conc (hr) (mg/L) 0 0. 5 61. 6 61. 5 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 + 0. 0 = 52. 3 16 26. 1 + 52. 3 = 78. 4 24 13. 1 +26. 1 + 52. 3 = 91. 5 32 6. 5 + 13. 1 + 26. 1 + 52. 3 = 98. 0 40 1. 6 + 6. 5 + 13. 1 + 26. 1 + 52. 3 = 99. 6 mg/L

Multiple ORAL Dosing – using the equation Recall that MAF was able to convert the single dose equation to a multiple dose equation Cmax ss 1 ---- = MAF = ------k Cmax 1 1 -e

Multiple ORAL Dosing – using the equation Recall that MAF was able to convert the single dose equation to a multiple dose equation 1 MAF = -----1 - e -K Dose Ct = ----- e-Kt V First Dose Conc. … predicts accumulation 1 x ------ 1 – e -K Accumulation Steady State Equation

Multiple ORAL Dosing – using the equation However, the single oral dosing equation has two exponentials (K and ka) and each will have its own MAF. 1 MAF = ------k 1 -e MAF for ka?

Multiple ORAL Dosing – using the equation, Predicting SS Predicts Concentration-time @ SS

Multiple ORAL Dosing – using the equation, all concentrations Predicts Concentration-time at ANY time following an ORAL dose
 (mg/L) 0 0.")
Multiple ORAL Dosing – using the equation SD Time Conc (hr) (mg/L) 0 0. 5 61. 6 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 16 26. 1 24 13. 1 32 6. 5 40 1. 6 MD Verify 24 hour concentration [Cmin dose 3] Conc Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; (mg/L) T½=8 hr; F=1 0. 0 Dosing Interval 8 hrs and t = 8 hrs. 61. 5 81. 7 86. 6 86. 0 -3*0. 086*8) 2*1*1000 (1 -e 0. 086*8 e 73. 9 Ct= 10*(2 -0. 086) (1 -e-0. 086*8) 62. 1 52. 3 (1 -e-3*2*8) e-2*8 78. 4 -2*8 (1 -e ) 91. 5 98. 0 99. 6
 (mg/L) 0 0.")
Multiple ORAL Dosing – using the equation SD Time Conc (hr) (mg/L) 0 0. 5 61. 6 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 16 26. 1 24 13. 1 32 6. 5 40 1. 6 MD Verify 24 hour concentration [Cmin dose 3] Conc Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; (mg/L) T½=8 hr; F=1 0. 0 Dosing Interval 8 hrs and t = 8 hrs. 61. 5 81. 7 86. 6 86. 0 -3*0. 086*8) 2*1*1000 (1 -e 0. 086*8 e 73. 9 Ct= 10*(2 -0. 086) (1 -e-0. 086*8) 62. 1 52. 3 (1 -e-3*2*8) e-2*8 78. 4 -2*8 (1 -e ) 91. 5 0. 875 1 - 1. 4 x 10 -21 98. 0 Ct = 104. 53 0. 5 - 1 - 1. 1 x 10 -7 0. 499 99. 6
 (mg/L) 0 0.")
Multiple ORAL Dosing – using the equation SD Time Conc (hr) (mg/L) 0 0. 5 61. 6 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 16 26. 1 24 13. 1 32 6. 5 40 1. 6 MD Verify 24 hour concentration [Cmin dose 3] Conc Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; (mg/L) T½=8 hr; F=1 0. 0 Dosing Interval 8 hrs. 61. 5 81. 7 86. 6 86. 0 -3*0. 086*8) 2*1*1000 (1 -e 0. 086*8 -2*8 e 73. 9 Ct= e -0. 086*8 10*(2 -0. 086) (1 -e ) 62. 1 52. 3 Ct = 104. 53 0. 875 0. 50 - 1. 0 0. 000000113 78. 4 0. 499 91. 5 = 104. 53[(1. 75)(0. 5) – (0. 000000113)] 98. 0 = 104. 53 [0. 875 – 0. 000000113] 99. 6 = 91. 46 mg/L
 (mg/L) 0 0.")
Multiple ORAL Dosing – using the equation SD Time Conc (hr) (mg/L) 0 0. 5 61. 6 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 16 26. 1 24 13. 1 32 6. 5 40 1. 6 MD Conc (mg/L) 0. 0 61. 5 81. 7 86. 6 86. 0 73. 9 62. 1 52. 3 78. 4 91. 5 98. 0 99. 6 Calculate Cmin at steady state Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; T½=8 hr; F=1 Dosing Interval 8 hrs. Cdose 3 - 8 hr = 91. 46 mg/L
 (mg/L) 0 0.")
Multiple ORAL Dosing – using the equation SD Time Conc (hr) (mg/L) 0 0. 5 61. 6 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 16 26. 1 24 13. 1 32 6. 5 40 1. 6 Calculate Cmin at steady state MD Conc Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; (mg/L) T½=8 hr; F=1 0. 0 Dosing Interval 8 hrs. and t = 8 hrs 61. 5 81. 7 86. 6 86. 0 2*1*1000 (1) 0. 086*8 -2*8 C = e 73. 9 t 1 e -0. 086*8 10*(2 -0. 086) (1 -e ) 62. 1 52. 3 1 0. 50 - 1. 00 0. 000000113 Ct = 104. 53 78. 4 0. 499 91. 5 = 104. 53[1 – (0. 000000113)] 98. 0 = 104. 53 [1 – 0. 000000113] 99. 6 = 104. 45 mg/L
 (mg/L) 0 0.")
Multiple ORAL Dosing – using the equation SD Time Conc (hr) (mg/L) 0 0. 5 61. 6 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 16 26. 1 24 13. 1 32 6. 5 40 1. 6 MD Conc (mg/L) 0. 0 61. 5 81. 7 86. 6 86. 0 73. 9 62. 1 52. 3 78. 4 91. 5 98. 0 99. 6 Calculate Cmin at steady state Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; T½=8 hr; F=1 Dosing Interval 8 hrs. Cmin. SS = 104. 45 mg/L
 (mg/L) 0 0.")
Multiple ORAL Dosing – using the equation SD Time Conc (hr) (mg/L) 0 0. 5 61. 6 1 81. 7 1. 5 86. 6 2 86. 0 4 73. 9 6 62. 1 8 52. 3 16 26. 1 24 13. 1 32 6. 5 40 1. 6 Calculate Cmin at steady state MD Conc Dose=1000 mg, V=10 L ka=2 hr-1; K=0. 0863 hr-1; (mg/L) T½=8 hr; F=1 0. 0 Dosing Interval 8 hrs. 61. 5 81. 7 86. 6 86. 0 73. 9 62. 1 52. 3 78. 4 91. 5 Cmin. SS = 104. 45 mg/L MAF = 1. 997 98. 0 Cmin 1 = 52. 3 mg/L 99. 6

Multiple ORAL Dosing but will MAF always work following oral absorption? Cmax ss 1 ---- = MAF = ------k Cmax 1 1 -e MAF does not consider ka … could this cause error in the estimation of accumulation? Evaluate initial conditions of: Dose =200; V = 20 L; half-life = 8 hr; ka is varied from 0. 029 to 10 and dosing interval is 8 hours. Cmax and Cmin is calculated for each dose.
 Tmax ka dose")
10 “formulations” are shown here, each with different absorption rates (ka) Tmax ka dose 1 (hr-1) Slow (hr)absorption 19. 0 0. 029 11. 55 0. 087 8. 00 0. 173 4. 65 0. 433 4. 14 0. 519 3. 43 0. 693 2. 95 0. 866 2. 02 1. 50 1. 22 3. 00 0. 48 10. 0 Fast absorption ka/K Cmax 1 0. 33 1. 0 2. 0 5. 0 6. 0 8. 0 10. 0 17. 3 34. 6 115. 4 [1. 92]1. 47 [3. 68]3. 47 5. 00 6. 69 6. 99 7. 43 7. 74 8. 40 9. 00 9. 59 Cmax. SS (actual) 14. 26 14. 68 14. 99 15. 78 16. 00 16. 39 16. 72 17. 52 18. 37 19. 25 K = 0. 08663 hr-1 T½= 8 hr = 8 hours; D=200 mg V= 20 L; F=1; ka is varied Cmax. SS (predicted) 2. 88 7. 36 10. 00 13. 38 13. 98 14. 86 15. 49 16. 80 18. 00 19. 19 Error (%) 273 99. 55 50. 00 17. 95 14. 46 10. 33 7. 95 4. 31 2. 05 0. 34
 produces different first dose Tmax ka dose 1 (hr-1) (hr)")
Different absorption rates (ka) produces different first dose Tmax ka dose 1 (hr-1) (hr) 19. 0 11. 55 8. 00 4. 65 4. 14 3. 43 2. 95 2. 02 1. 22 0. 48 0. 029 0. 087 0. 173 0. 433 0. 519 0. 693 0. 866 1. 50 3. 00 10. 0 ka/K Cmax 1 0. 33 1. 0 2. 0 5. 0 6. 0 8. 0 10. 0 17. 3 34. 6 115. 4 [1. 92]1. 47 [3. 68]3. 47 5. 00 6. 69 6. 99 7. 43 7. 74 8. 40 9. 00 9. 59 Cmax. SS (actual) 14. 26 14. 68 14. 99 15. 78 16. 00 16. 39 16. 72 17. 52 18. 37 19. 25 K = 0. 08663 hr-1 T½= 8 hr = 8 hours; D=200 mg V= 20 L; F=1; ka is varied Cmax. SS (predicted) 2. 88 7. 36 10. 00 13. 38 13. 98 14. 86 15. 49 16. 80 18. 00 19. 19 Error (%) 273 99. 55 50. 00 17. 95 14. 46 10. 33 7. 95 4. 31 2. 05 0. 34
 Tmax ka dose")
10 “formulations” are shown here, each with different absorption rates (ka) Tmax ka dose 1 (hr-1) Slow (hr)absorption 19. 0 0. 029 11. 55 0. 087 8. 00 0. 173 4. 65 0. 433 4. 14 0. 519 3. 43 0. 693 2. 95 0. 866 2. 02 1. 50 1. 22 3. 00 0. 48 10. 0 Fast absorption ka/K Cmax 1 0. 33 1. 0 2. 0 5. 0 6. 0 8. 0 10. 0 17. 3 34. 6 115. 4 [1. 92]1. 47 [3. 68]3. 47 5. 00 6. 69 6. 99 7. 43 7. 74 8. 40 9. 00 9. 59 Cmax. SS (actual) 14. 26 14. 68 14. 99 15. 78 16. 00 16. 39 16. 72 17. 52 18. 37 19. 25 K = 0. 08663 hr-1 T½= 8 hr = 8 hours; D=200 mg V= 20 L; F=1; ka is varied Cmax. SS (predicted) 2. 88 7. 36 10. 00 13. 38 13. 98 14. 86 15. 49 16. 80 18. 00 19. 19 Error (%) 273 99. 55 50. 00 17. 95 14. 46 10. 33 7. 95 4. 31 2. 05 0. 34
 produces different first dose Tmax ka dose 1 (hr-1) (hr)")
Different absorption rates (ka) produces different first dose Tmax ka dose 1 (hr-1) (hr) 19. 0 11. 55 8. 00 4. 65 4. 14 3. 43 2. 95 2. 02 1. 22 0. 48 0. 029 0. 087 0. 173 0. 433 0. 519 0. 693 0. 866 1. 50 3. 00 10. 0 ka/K Cmax 1 0. 33 1. 0 2. 0 5. 0 6. 0 8. 0 10. 0 17. 3 34. 6 115. 4 [1. 92]1. 47 [3. 68]3. 47 5. 00 6. 69 6. 99 7. 43 7. 74 8. 40 9. 00 9. 59 Cmax. SS (actual) 14. 26 14. 68 14. 99 15. 78 16. 00 16. 39 16. 72 17. 52 18. 37 19. 25 K = 0. 08663 hr-1 T½= 8 hr = 8 hours; D=200 mg V= 20 L; F=1; ka is varied Cmax. SS (predicted) 2. 88 7. 36 10. 00 13. 38 13. 98 14. 86 15. 49 16. 80 18. 00 19. 19 Error (%) 273 99. 55 50. 00 17. 95 14. 46 10. 33 7. 95 4. 31 2. 05 0. 34

Using MAF, Cmax. SS is predicted from Cmax 1. K = 0. 08663 hr T½= 8 hr This prediction is reasonable in some cases, = 8 hours; D=200 mg very poor in others V= 20 L; F=1; ka is varied Tmax ka ka/K Cmax 1 Cmax. SS Error dose 1 (hr-1) (actual) (predicted) (%) (hr) -1 19. 0 11. 55 8. 00 4. 65 4. 14 3. 43 2. 95 2. 02 1. 22 0. 48 0. 029 0. 087 0. 173 0. 433 0. 519 0. 693 0. 866 1. 50 3. 00 10. 0 0. 33 1. 0 2. 0 5. 0 6. 0 8. 0 10. 0 17. 3 34. 6 115. 4 [1. 92]1. 47 [3. 68]3. 47 5. 00 6. 69 6. 99 7. 43 7. 74 8. 40 9. 00 9. 59 14. 26 14. 68 14. 99 15. 78 16. 00 16. 39 16. 72 17. 52 18. 37 19. 25 2. 88 7. 36 10. 00 13. 38 13. 98 14. 86 15. 49 16. 80 18. 00 19. 19 273 poor 99. 55 50. 00 17. 95 14. 46 10. 33 7. 95 close 4. 31 2. 05 Very 0. 34 close

If Error less than 10% is acceptable, K = 0. 08663 hr T½= 8 hr unacceptable deviations only occur = 8 hours; D=200 mg with slower releasing formulations V= 20 L; F=1; ka is varied Tmax ka ka/K Cmax 1 Cmax. SS Error dose 1 (hr-1) (actual) (predicted) (%) (hr) -1 19. 0 11. 55 8. 00 4. 65 4. 14 3. 43 2. 95 2. 02 1. 22 0. 48 0. 029 0. 087 0. 173 0. 433 0. 519 0. 693 0. 866 1. 50 3. 00 10. 0 0. 33 1. 0 2. 0 5. 0 6. 0 8. 0 10. 0 17. 3 34. 6 115. 4 [1. 92]1. 47 [3. 68]3. 47 5. 00 6. 69 6. 99 7. 43 7. 74 8. 40 9. 00 9. 59 14. 26 14. 68 14. 99 15. 78 16. 00 16. 39 16. 72 17. 52 18. 37 19. 25 2. 88 7. 36 10. 00 13. 38 13. 98 14. 86 15. 49 16. 80 18. 00 19. 19 273 99. 55 50. 00 17. 95 14. 46 10. 33 7. 95 4. 31 2. 05 0. 34

MAF fails with oral absorption, primarily slow absorption K = 0. 08663 hr T½= 8 hr ? When does this occur (ka/K <10) = 8 hours; D=200 mg -1 Tmax ka dose 1 (hr-1) (hr) 19. 0 11. 55 8. 00 4. 65 4. 14 3. 43 2. 95 2. 02 1. 22 0. 48 0. 029 0. 087 0. 173 0. 433 0. 519 0. 693 0. 866 1. 50 3. 00 10. 0 ka/K Cmax 1 0. 33 1. 0 2. 0 5. 0 6. 0 8. 0 10. 0 17. 3 34. 6 115. 4 [1. 92]1. 47 [3. 68]3. 47 5. 00 6. 69 6. 99 7. 43 7. 74 8. 40 9. 00 9. 59 Cmax. SS (actual) 14. 26 14. 68 14. 99 15. 78 16. 00 16. 39 16. 72 17. 52 18. 37 19. 25 V= 20 L; F=1; ka is varied Cmax. SS (predicted) 2. 88 7. 36 10. 00 13. 38 13. 98 14. 86 15. 49 16. 80 18. 00 19. 19 Error (%) 273 99. 55 50. 00 17. 95 14. 46 10. 33 7. 95 4. 31 2. 05 0. 34
 with Cmin. Tmax ka dose 1 (hr-1) (hr) 19.")
MAF works better (less error) with Cmin. Tmax ka dose 1 (hr-1) (hr) 19. 0 11. 55 8. 00 4. 65 4. 14 3. 43 2. 95 2. 02 1. 22 0. 48 0. 029 0. 087 0. 173 0. 433 0. 519 0. 693 0. 866 1. 50 3. 00 10. 0 ka/K Cmin 1 0. 33 1. 0 2. 0 5. 0 6. 0 8. 0 10. 0 17. 3 34. 6 115. 4 1. 47 3. 47 5. 00 5. 86 5. 81 5. 67 5. 54 5. 31 5. 15 5. 04 Cmin. SS (actual) 14. 09 13. 87 13. 33 12. 10 11. 81 11. 39 11. 10 10. 61 10. 30 10. 09 K = 0. 08663 hr-1 T½= 8 hr = 8 hours; D=200 mg V= 20 L; F=1; ka is varied Cmin. SS (predicted) 2. 95 6. 93 10. 00 11. 72 11. 63 11. 34 11. 09 10. 62 10. 30 10. 09 Error (%) 380 100. 0 33. 4 3. 23 1. 59 0. 39 0. 1 0. 001 -----

MAF fails with oral absorption, primarily slow absorption K = 0. 08663 hr T½= 8 hr ? When does this occur = 8 hours; D=200 mg -1 Tmax ka dose 1 (hr-1) (hr) 19. 0 11. 55 8. 00 4. 65 4. 14 3. 43 2. 95 2. 02 1. 22 0. 48 0. 029 0. 087 0. 173 0. 433 0. 519 0. 693 0. 866 1. 50 3. 00 10. 0 ka/K Error Cmax (%) 0. 33 1. 0 2. 0 5. 0 6. 0 8. 0 10. 0 17. 3 34. 6 115. 4 273 99. 55 50. 00 17. 95 14. 66 10. 33 7. 95 4. 31 2. 05 0. 34 Error Cmin (%) V= 20 L; F=1; ka is varied Error is greater 380 in Cmax. 100 33. 4 Error 3. 23 is due to the failure 1. 59 to consider ka 0. 39 in MAF. 0. 1 When absorption 0. 001 has a greater effect ----on concentration, ----error is increased.

MAF fails with oral absorption, primarily slow absorption K = 0. 08663 hr T½= 8 hr ? When does this occur = 8 hours; D=200 mg -1 Tmax ka dose 1 (hr-1) (hr) 19. 0 11. 55 8. 00 4. 65 4. 14 3. 43 2. 95 2. 02 1. 22 0. 48 0. 029 0. 087 0. 173 0. 433 0. 519 0. 693 0. 866 1. 50 3. 00 10. 0 ka/K Error Cmax (%) 0. 33 1. 0 2. 0 5. 0 6. 0 8. 0 10. 0 17. 3 34. 6 115. 4 273 99. 55 50. 00 17. 95 14. 66 10. 33 7. 95 4. 31 2. 05 0. 34 Error Cmin (%) 380 100 33. 4 3. 23 1. 59 0. 39 0. 1 0. 001 ----- V= 20 L; F=1; ka is varied For immediate release formulations, error is generally ~ 10% or less. This occurs when absorption is faster than elimination ka/K > 5 -10.

MAF fails with oral absorption, primarily slow absorption K = 0. 08663 hr T½= 8 hr ? When does this occur = 8 hours; D=200 mg MAF can be used to predict SS concentrations, but error increases as you move -1 20 L; F=1; ka is varied from Cmin to Cmax, as ratio of T½: increases and ratio of. V= ka/K decreases. For immediate release formulations, error is generally ~ 10% or less. Red shaded area represent profiles with a Tmax occurring AFTER 4 hours. This occurs when absorption is slow (SR formulations) or ratio ka/K < 5 -10. T½: = 0. 5 T½: = 2

Multiple ORAL Dosing Time to Achieve Steady State is Determined By? Dose Half-life Dosing Interval Volume of Distribution

Multiple ORAL Dosing – time to steady state Time to Achieve Steady State is Determined By? Dose Half-life Dosing Interval Volume of Distribution Half-life Number Of Half-lives 1 2 3 4 5 6 7 Time to SS is determined entirely by the half-life of the drug While steady–state is never actually reached You approach SS 1/2 way each half-life, you reach 90% of true steady state after 3. 3 half-lives. Percent Of Steady State 50 75 87. 5 but sometimes … elimination of a drug is 93. 75 “rate-limited” by absorption. 96. 875 How does this affect the time to SS? 98. 4375 Is time to SS is determined by the 99. 21875 slowest exponential …?

Multiple ORAL Dosing – time to steady state Evaluate time to SS – look at Cmin for products with a different ka. Drug: T½ = 5 hr; = 8 hr, Dose = 100 mg; V= 10 L; F=1. MAF = 1. 492 ka = 0. 05 ka=0. 18 ka= 0. 693 ka =13. 86 ka/k=0. 36 ka/k=1. 3 ka/k=5 ka/k=100 MAF predicts Dose time [mg/L] well for Cmin. SS 1 0. 00 1. 54 2. 62 3. 35 4. 16 4. 04 0. 00 4. 63 6. 35 6. 68 5. 24 4. 08 0. 00 8. 97 7. 66 6. 66 4. 40 3. 33 0 1 2 3 6 8 0. 00 0. 46 0. 83 1. 13 1. 72 1. 92 3 8 5. 34 8 61. % ? ? ? 7. 32 92. 5% 5. 89 96. 4% 4. 80 when ka/K >5 -10 & or Tmax was less than 4 hr. So why does it not work with a ka of 0. 05 hr-1? 96. 6% 8 8. 22 7. 91 6. 11 4. 97 14 8 8. 67 7. 91 6. 11 4. 97 SS achieved

Multiple ORAL Dosing – time to steady state Evaluate time to SS – look at Cmin for products with a different ka. Drug: T½ = 5 hr; = 8 hr, Dose = 100 mg; V= 10 L; F=1. MAF = 1. 492 ka = 0. 05 ka=0. 18 ka= 0. 693 ka =13. 86 ka/k=0. 36 ka/k=1. 3 ka/k=5 ka/k=100 [mg/L] MAF predicts well for Cmin. SS when ka/K >5 -10 & or Tmax was less than 4 hr. 96% SS @ 24 hr 61% SS at 24 hr Cmin 1 = Cmax 1 So why does it not work with a ka of 0. 05 hr-1? ka/K = 0. 5 K > ka

Multiple ORAL Dosing – time to steady state Evaluate time to SS – look at Cmin for products with a different ka. Drug: T½ = 5 hr; = 8 hr, Dose = 100 mg; V= 10 L; F=1. MAF = 1. 492 ka = 0. 05 ka=0. 18 ka= 0. 693 ka =13. 86 K > ka ka/k=0. 36 ka/k=1. 3 ka/k=5 ka/k=100 so ka is the [mg/L]slowest exponential and appears in the terminal phase of the profile. 92% SS at 48 hr =3. 46 T½ 61% SS at 24 hr ka determines time to achieve Steady-State. T½ = 13. 86 hr. 3. 3 T½ = 45. 7 hr Cmin 48 hr = 8. 0 mg/L Cmin. SS = 8. 69 mg/L

How long does it take to get to steady state? When did SS occur? Steady State is considered to have been achieved when the Concentration is within 10% of the true steady state concentration. 90% of true steady state will occur at ~ 3. 3 half-lives. Number Percentage Sometimes, SS is not considered to have Of of Eventual been achieved until concentrations exceed T½ SS Achieved 95% of the true steady state concentrations. (%) This occurs between 4 and 5 half-lives. 1 50 This gives rise to the statement that 2 75 3 87. 5 steady state is achieved in 3 -5 half-lives. 4 93. 25 Each T½ reduces the gap between 5 96. 875 current concentrations and SS by half. 6 98. 4375 SS 100 Dosing interval (τ) does not affect time to SS

How long does it take to get to steady state? When did SS occur? Steady State is considered to have been achieved when the Concentration is within 10% of the true steady state concentration. 90% of true steady state will occur at ~ 3. 3 half-lives. Number Percentage Of of Eventual T½ SS Achieved (%) 1 50 2 75 3 87. 5 4 93. 25 5 96. 875 6 98. 4375 SS 100 When is 90% of true (eventual) Steady State Achieved? e-Kt determines proportion lost

How long does it take to get to steady state? When did SS occur? Steady State is considered to have been achieved when the Concentration is within 10% of the true steady state concentration. 90% of true steady state will occur at ~ 3. 3 half-lives. Number Percentage Of of Eventual T½ SS Achieved (%) 1 50 2 75 3 87. 5 4 93. 25 5 96. 875 6 98. 4375 SS 100 When is 90% of true (eventual) Steady State Achieved? e-Kt determines proportion lost e-K# determines proportion lost for a set number (#) of half-lives Example: If K = 0. 693 and # = 2 T½ = e (-0. 693 x 2) = 0. 25

How long does it take to get to steady state? When did SS occur? Steady State is considered to have been achieved when the Concentration is within 10% of the true steady state concentration. 90% of true steady state will occur at ~ 3. 3 half-lives. Number Percentage Of of Eventual T½ SS Achieved (%) 1 50 2 75 3 87. 5 4 93. 25 5 96. 875 6 98. 4375 SS 100 When is 90% of true (eventual) Steady State Achieved? e-K# determines proportion lost … then 1 - e-K# will determine proportion of steady-state achieved. Example: If K = 0. 693 and # = 2 T½ = 1 -e (-0. 693 x 2) = 0. 75 Or expressed as a % 75% of SS after 2 T½

How long does it take to get to steady state? When did SS occur? Steady State is considered to have been achieved when the Concentration is within 10% of the true steady state concentration. 90% of true steady state will occur at ~ 3. 3 half-lives. Number Percentage When is 90% of true (eventual) Of of Eventual Steady State Achieved? T½ SS Achieved e-K# determines proportion lost (%) 1 50 (-0. 693 x #) and … 1 e 2 75 determines proportion of steady-state achieved. 3 87. 5 4 93. 25 (-0. 693 x #) ) and … 100 x (1 e 5 96. 875 6 98. 4375 determines percent of steady-state achieved, where # is the number of half-lives. SS 100 % SS = 100 x (1 - e (-0. 693 x #) )

How long does it take to get to steady state? When did SS occur? Steady State is considered to have been achieved when the Concentration is within 10% of the true steady state concentration. 90% of true steady state will occur at ~ 3. 3 half-lives. Number Percentage When is 90% of true (eventual) Of of Eventual Steady State Achieved? T½ SS Achieved % SS = 100 x (1 - e (-0. 693 x #) ) (%) 1 50 Therefore, 90% of true SS is achieved… 2 75 90 = 100 x (1 - e (-0. 693 x #) ) 3 87. 5 (-0. 693 x #) 0. 9 = 1 e 4 93. 25 (-0. 693 x #) = 0. 1 e 5 96. 875 (-0. 693 x #) = ln(0. 1) ln(e 6 98. 4375 -0. 693 x # = -2. 30259 SS 100 # = 3. 322

How long does it take to get to steady state? When did SS occur? Steady State is considered to have been achieved when the Concentration is within 10% of the true steady state concentration. 90% of true steady state will occur at ~ 3. 3 half-lives. Number Percentage Of of Eventual T½ SS Achieved (%) 1 50 2 75 3 87. 5 4 93. 25 5 96. 875 6 98. 4375 SS 100 When is 90% of true (eventual) Steady State Achieved? After 3. 322 half-lives … frequently stated as 3. 3 half lives When is 95% of true (eventual) Steady State Achieved? ln(e (-0. 693 x #) = ln(0. 05) -0. 693 x # = -2. 9957 # = 4. 322

Multiple ORAL Dosing – Effect of ka. Absorption rate affects a number of things with multiple doses It can determine time to steady state It can affect the accuracy of MAF Can it affect anything else ? ka is the rate at which a drug is absorbed. ka and k are two determinants of Tmax = [ln(ka/k) / (ka-k)] This is the equation for Tmax after 1 dose What is the effect of ka on Tmax on the way to steady state?

Multiple ORAL Dosing – Effect of ka on Tmax. Steady State & the Effect on Tmax Consider a drug with a 5 hour half-life, administered every 8 hours Dose time # hr ka = 0. 05 ka/k=0. 36 [mg/L] 1 0 1 2 3 6 8 0. 00 0. 46 0. 83 1. 13 1. 72 1. 92 ka=0. 18 ka/k=1. 3 [mg/L] ka= 0. 693 ka/k=5 [mg/L] ka =13. 86 ka/k=100 [mg/L] 0. 00 1. 54 2. 62 3. 35 4. 16 4. 04 0. 00 4. 63 6. 35 6. 68 5. 24 4. 08 0. 00 8. 97 7. 66 6. 66 4. 40 3. 33 What will happen to TMAX in every case ?

Steady State & the Effect on Tmax Consider a drug with a 5 hour half-life, administered every 8 hours Dose time ka = 0. 05 ka=0. 18 ka= 0. 693 ka =13. 86 ka/k=0. 36 ka/k=1. 3 ka/k=5 ka/k=100 # hr [mg/L] 1 0 1 2 3 6 8 0. 00 0. 46 0. 83 1. 13 1. 72 1. 92 0. 00 1. 54 2. 62 3. 35 4. 16 4. 04 0. 00 4. 63 6. 35 6. 68 5. 24 4. 08 0. 00 8. 97 7. 66 6. 66 4. 40 3. 33 3 0 1 2 4 7 8 3. 84 4. 30 4. 67 5. 13 5. 35 5. 34 6. 34 7. 50 8. 19 8. 57 7. 76 7. 32 5. 44 9. 38 10. 49 9. 55 6. 72 5. 89 4. 43 12. 65 11. 01 8. 35 5. 51 4. 80

Steady State & the Effect on Tmax Consider a drug with a 5 hour half-life, administered every 8 hours Dose time ka = 0. 05 ka/k=0. 36 ka=0. 18 ka/k=1. 3 ka= 0. 693 ka/k=5 ka =13. 86 ka/k=100 1 0. 00 0. 46 0. 83 1. 13 1. 72 1. 92 0. 00 1. 54 2. 62 3. 35 4. 16 4. 04 0. 00 4. 63 6. 35 6. 68 5. 24 4. 08 0. 00 8. 97 7. 66 6. 66 4. 40 3. 33 0 1 2 3 6 8 peak occurs at…. . 1 st dose 11. 5 hr (8) 6. 31 hr 2. 9 hr 0. 336 hr 3 rd dose 7. 25 hr 3. 75 hr 2. 5 hr 0. 34 hr 14 th dose 3. 5 hr 3. 1 hr 2. 2 hr 0. 31 Steady migration of the Tmax to occur earlier most pronounced with SR products

Multiple ORAL Dosing – Effect of ka on Tmax. Does Tmax really move regardless of ka magnitude? ka (hr-1) ka/k 0. 0138 0. 01 0. 05 0. 36 0. 10 0. 72 0. 20 1. 44 0. 55 3. 97 1. 00 7. 22 2. 00 14. 43 4. 98 35. 93 100. 721. 0 Tmax (obs at SS) (hr) 3. 59 3. 50 3. 10 2. 40 1. 85 1. 22 0. 65 0. 062 Tmax after 1 dose Tmax Error (equation) (%) (hr) 18. 46 11. 50 8. 40 5. 85 3. 33 2. 29 1. 43 0. 74 0. 066 Equation predicts first dose … but Tmax at SS moves in! Movement is greatest for SR products … but also occurs with IV bolus when accumulation occurs. 18. 46 11. 50 8. 40 5. 85 3. 33 2. 29 1. 43 0. 74 0. 66 14. 87 8. 01 5. 30 3. 45 0. 93 0. 44 0. 21 0. 91 0. 004 K = 0. 1385 hr-1 T½= 5 hr = 8 hours ka is varied

Does a shifting Tmax have any relevance to the patient ? YES When does the Tmax actually occur? Do you really know? We commonly see single dose kinetic data. If we are told that the Tmax is (on average) 8 hours … what is it in an individual patient at SS? Subject Tmax 1 2 3 4 5 6 7 8 9 10 11 8. 5 12. 25 12. 16 8. 16 6. 58 4. 00 10. 33 12. 00 7. 66 6. 08 6. 28 Mean: 8. 55 hr Range: 4. 0 -12. 25 So … for TDM, is it reasonable to measure the concentration at Tmax ? toxicity ? ? dosage adjustment ? ? Recommend routine use of Cmin

FAQ 1. What is the purpose of and SR Product ? To reduce the peak-trough fluctuation …? Or allow the product to be given less frequently ?

FAQ 1. What is the purpose of and SR Product ? Smallest Peak / trough fluctuation provided by product with smallest Ka/K ratio [SR product]

FAQ 2. Mr BB requires 200 mg/day of morphine for chronic cancer pain. There are several morphine formulations available for use, but it is decided that a sustained release formulations would provide Mr. BB with convenience and a smooth concentration-time profile that should provide good pain control. Kadian® and MS Contin® are 2 sustained release formulations. Kadian® is recommended for Q 24 hr dosing and peaks at 10 hr. MS-Contin® is recommended for Q 12 hr dosing and peaks 4 -5 hr. Which formulation will yield the smallest peak-trough difference? Kadian® giving 200 mg q 24 hours (recommended) Kadian® giving 100 mg q 12 hours (100 mg/day) MS-Contin® giving 200 mg q 24 hours MS-Contin® giving 100 mg q 12 hours (recommended) What do we need to calculate? K, ka, AUC, F, V, Cmax, Tmax, Cl…?

FAQ 2. There are two modified release morphine formulations. Your patient requires 200 mg per day. Which formulation will yield the smallest peak-trough difference? Kadian® is recommended for Q 24 hr dosing and peaks at 10 hr. MS-Contin® is recommended for Q 12 hr dosing and peaks 4 -5 hr. We will answer this question assuming a 1 C model with first order absorption and first order elimination. The half-life of morphine should fall between 2 and 4 hours in most individuals with normal liver function. We will assume a half-life of 3 hours to solve our question. Half-life of 3 hr corresponds to a K value of … ? K = 0. 693/ 3 hr = 0. 231 hr-1

FAQ 2. There are two modified release morphine formulations. Your patient requires 200 mg per day. Which formulation will yield the smallest peak-trough difference? Kadian® is recommended for Q 24 hr dosing and peaks at 10 hr. MS-Contin® is recommended for Q 12 hr dosing and peaks 4 -5 hr. K = 0. 231 hr-1 for Kadian® and MS-Contin® formulations Estimate ka …! Using the 1 C single dose Excel® spread sheet, knowing that the Tmax for Kadian® is 10 hr and Tmax for MS-Contin® is 4. 5 hr. Volume for morphine is ~4 L/kg. Assume 280 L. ka for MS-Contin® = 0. 27011 hr-1 ka for Kadian® = 0. 031399 hr-1

FAQ 2. There are two modified release morphine formulations. Your patient requires 200 mg per day. Which formulation will yield the smallest peak-trough difference? Kadian® is recommended for Q 24 hr dosing and peaks at 10 hr. MS-Contin® is recommended for Q 12 hr dosing and peaks 4 -5 hr. ?

FAQ 2. There are two modified release morphine formulations. Your patient requires 200 mg per day. Which formulation will yield the smallest peak-trough difference? Kadian® is recommended for Q 24 hr dosing and peaks at 10 hr. MS-Contin® is recommended for Q 12 hr dosing and peaks 4 -5 hr. Kadian Single Dose Profile Tmax = 10 hr Cmax = 28 ng/m. L AUC = 1. 24 mg*hr/L V = 240 L F = 0. 4 MS-Contin Profile Tmax = 4. 5 hr Cmax = 113 ng/m. L AUC = 1. 24 mg*hr/L V = 240 L F = 0. 4 Which formulation will yield the smallest peak-trough difference?

FAQ 2. There are two modified release morphine formulations. Your patient requires 200 mg per day. Which formulation will yield the smallest peak-trough difference? Kadian® is recommended for Q 24 hr dosing and peaks at 10 hr. MS-Contin® is recommended for Q 12 hr dosing and peaks 4 -5 hr. Which formulation will yield the smallest peak-trough difference? Kadian® giving 200 mg q 24 hours (recommended) Kadian® giving 100 mg q 12 hours (100 mg/day) MS-Contin® giving 200 mg q 24 hours MS-Contin® giving 100 mg q 12 hours (recommended) Take the Kadian Single Dose Profile MS-Contin Profile single dose Tmax = 10 hr Tmax = 4. 5 hr kinetic parameters Cmax = 28 ng/m. L Cmax = 113 ng/m. L and move to AUC = 1. 24 mg*hr/L a multiple V = 240 L dose Excel® F = 0. 4 sheet

MS-Contin® 100 mg Q 12 H Peak = 70. 0 ng/m. L Trough = 25. 7 ng/m. L MS-Contin® 200 mg Q 24 H MS Contin® Recommended to be given every 12 hours. Peak = 115. 5 ng/m. L Trough = 4. 7 ng/m. L

Kadian® 100 mg Q 12 H Peak = 53. 4 ng/m. L Trough = 47. 4 ng/m. L Kadian® 200 mg Q 24 H Kadian® Recommended to be given every 24 hours. Peak = 58. 9 ng/m. L Trough = 39. 6 ng/m. L

Questions 2. There are two modified release morphine formulations. Your patient requires 200 mg per day. Which formulation will yield the smallest peak-trough difference? Kadian® is recommended for Q 24 hr dosing and peaks at 10 hr. MS-Contin® is recommended for Q 12 hr dosing and peaks 4 -5 hr. Which formulation will yield the smallest peak-trough difference? Regimen MS-Contin 100 q 12 H MS-Contin 200 q 24 H Kadian 100 q 12 H Kadian 200 q 24 H Peak Trough Range ng/m. L 70. 0 115. 5 53. 4 58. 9 25. 7 47. 4 39. 6 44. 3 [rec] 110. 8 6. 0 19. 3 [rec] For ANY formulation, giving a smaller dose more frequently will ALWAYS reduce peak-trough fluctuations

Questions 3. A patient receives a drug every 12 hours. The drug has a half-life of ~5. 7 hour the patient misses a dose … but remembers half way through the interval. Should the patient take the next scheduled dose (forget missed dose) or … take the missed dose immediately and resume normal dosing or … take two doses at the next scheduled time?
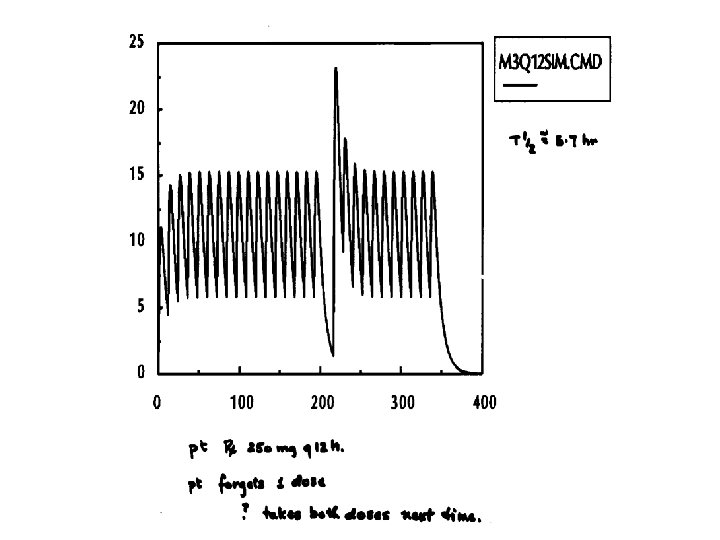

Correct Answer is drug dependant based on relationships between concentration & toxicity, risk of sub-therapeutic concentrations, half-life & dosing interval.
- Slides: 81