Multiple Myeloma Multiple Myeloma MM is a malignant

 is “a malignant disorder of the monoclonal plasma cells. ” •")






 and Female (XY)1 •")


![Patient Criteria M-protein Monoclonal plasma cells in bone marrow, % End-organ damage MGUS[1, 2]](https://slidetodoc.com/presentation_image_h/a1cf91353119e65c82004a9ba25b5905/image-15.jpg "Patient Criteria M-protein Monoclonal plasma cells in bone marrow, % End-organ damage MGUS[1, 2]")











- Slides: 29
Multiple Myeloma
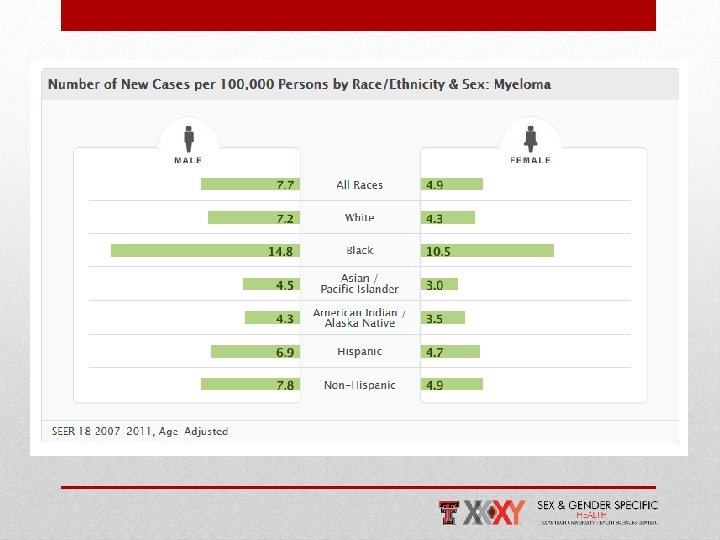
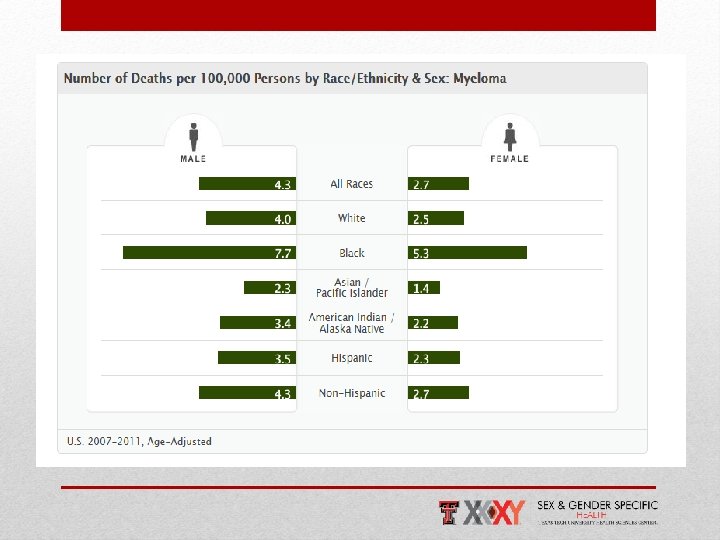
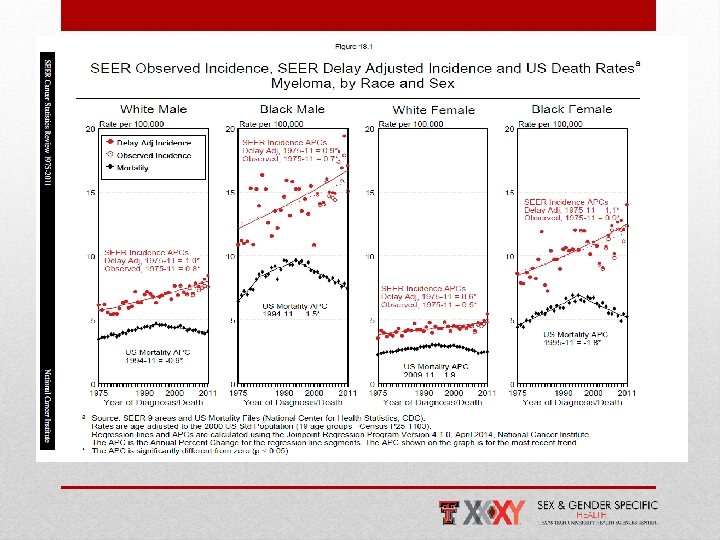
Multiple Myeloma (MM) is “a malignant disorder of the monoclonal plasma cells. ” • Is characterized by lytic bone lesions, infiltrate in the bone marrow, hypercalcemia, renal failure, anemia, and a monoclonal protein in the serum or urine 2 • Remains an incurable neoplasm of plasma cells that affects more than 20, 000 people annually in the United States 3 Men and African Americans have twice the incidence of MM as Women and Whites, respectively!!4 Introduction
• MM accounts for 1% of all malignancies and is the 2 nd most common hematologic malignancy with prevalence of around 10%. • The prevalence of MM was around 64, 615 in 2008. 1 Epidemiology
Natural History of Myeloma
Plasma Cells Pathogenesis • MM represents a stepwise process of malignancy: • Premalignant Stage: Monoclonal gammopathy of undetermined significance (MGUS), with a number of cytogenetic and gene abnormalities 1. • Malignant Stage i. Includes: • Induction of angiogenesis 3 • Suppression of cell immunity 3 • Involvement of cytokines such as IL-6 and VEGF. 5 Patho-Biology
Cytogenetic Alterations: • It has been well documented that all MM develops from MGUS, and the initial event required for transformation to MGUS provides the first step. 1 • The most common alteration is hyperdiploidy. 2 • Additional recurrent abnormalities include loss of chromosome 13. 2 Cytogenetics Chromosomal Frequency Alteration (%) Genes Included Hyperdiploidy 50 -60 Unclear Hypodiploidy 20 Unclear del(17 p) 8 P 53 t(4: 14) 15 FGFR 3, MMSET t(11; 14) 20 Cyclin D 1 del(13) or (13 q) 50 Unclear
Growth of the MM Cell in the BM Microenvironment • Myeloma cells interact with BM stromal cells, leading to cytokine production and adhesion signaling changes. • This change affects the migration and localization of the myeloma cells in the BM. 1, 2 • Moreover, proliferative and antiapoptotic signaling cascades activated in myeloma as a result of these interactions include PI 3 K/Akt, MAPK kinase (MEKK)/ERK, JAK 2/STAT 3, and NFκB pathways. MM In The Bone Marrow
• The progression of MGUS to myeloma is characterized by the development of bone lesions. • The pathogenetic mechanisms involved are complex and involve a combination of osteoclast activation coupled with osteoblast inhibition. 2 • There are several important mechanisms that mediate increased osteoclast activation. • There is an increase in NF-κB ligand RANKL expression by osteoblasts and possibly plasma cells. 3, 4 MM In The Skeleton
The same type of screening is recommended for Male (XY) and Female (XY)1 • Screen for multiple myeloma every 6 to 12 months in patients with a diagnosis of MGUS. 1 • Recognize that MGUS precedes symptomatic MM. 2 • CBC, Ca++ level, Cr. level, Serum free light chains, and 24 -hour urine protein electrophoresis. 3 Screening
Ancillary Studies • If the serum M-spike is >1. 5 g/d. L, obtain a bone survey and a bonemarrow aspirate. 1 • If these studies are normal, repeat the serum protein electrophoresis, CBC, creatinine, and calcium at 6 months if <2. 0 g/d. L and at 3 months if ≥ 2. 0 g/d. L. 2, 3 • If values remain stable, reduce screening frequency to yearly in the <2. 0 g/d. L group and every 6 months in the ≥ 2. 0 g/d. L group. 2, 3 Screening
• A thorough history to look for manifestations of the disease and its complications. • Although the symptoms of MM can be nonspecific they are usually more pronounced in FEMALES. 1 • Symptoms of MM can reflect: • Anemia, hypercalcemia, lytic bone lesions, hyperviscosity or thrombocytopenia, softtissue plasmacytomas, or hypogammaglobulinemia. 2 Diagnosis H & P Sign/Symptom Note H Fatigue and Fever In approximately 32% of patients with MM. May be due to anemia, hyper. Ca, hyperviscosity, or renal failure. H Bone Pain Reported in 58% of patients. May be due to osteolytic bone disease or fractures. H Infections Due to hypogammaglobulinemia. P Visual Disturbance Can result from hyperviscosity P Pallor Anemia P Lumps Plasmacytomas
Patient Criteria M-protein Monoclonal plasma cells in bone marrow, % End-organ damage MGUS[1, 2] Smoldering Myeloma[1] Symptomatic Myeloma[1] < 3 g/d. L spike ≥ 3 g/d. L spike and/or In serum and/or urine[2] < 10 ≥ 10[2] None ≥ 1 CRAB* feature[3] *C: Calcium elevation (> 10. 5 mg/L or ULN) R: Renal dysfunction (serum creatinine > 2 mg/d. L) A: Anemia (Hb < 10 g/d. L or 2 g < normal) B: Bone disease (lytic lesions or osteoporosis) Diagnostic Criteria for Myeloma
Use laboratory studies to confirm the diagnosis of MM and differentiate it from other plasma-cell disorders!1, 2, 3 Test you must have: üCBC üSerum calcium and creatinine üSerum Protein Electrophoresis üSerum free light chains üQuantitative immunoglobulins ü 24 -hour urine PEP üSerum β-2 microglobulin üRadiographic bone survey! Lab-Work
A Osteolytic Lesion • The most common symptoms are fatigue and bone pain. 1 • Osteolytic bone lesions can be detected on routine x-rays, MRI, CT, or combined FDG-PET/CT. 2 • Bone pain may present as an area of persistent pain or be migratory. • Often in the lower back and pelvis. • Pain may be sudden in onset when associated with a pathological fracture and is often precipitated by movement. 2 Bone Tests
• Performed to quantify the monoclonal proteins present in myeloma. 1 • 70% is Ig. G • 20%, it is Ig. A • 5% to 10% is light chains only 2 • After recognition of a localized band suggestive of an M protein on SPEP, immunofixation is necessary for confirmation and to determine the heavy- and lightchain class of the M protein. 3 Protein Electrophoresis
Risk-stratify patients with MM using established staging systems and prognostic factors 1 • Use clinical and lab data to stage patients with MM using the Durie. Salmon Staging System or the International Staging System. 1, 2 • Classify as stage I, II, or III, • Stage I having the most favorable prognosis 3 • Understand that important prognostic factors include 3, 4: • Albumin, Hb, Ca++, β 2 microglobulin • M-component production rate • Bone x-ray results| International Staging System Stage I Features Median Survival (Months) Serum β 2 microglobulin <3. 5. Albumin >3. 4 62 II Not stage I or III 44 III Serum β 2 microglobulin >5. 4 mg/dl 29 Staging – Risk Stratification
Initial Approach to Treatment of Myeloma
• First-in-class proteasome inhibitor • Bortezomib • Carfilzomib • Via inhibition of proteasomal degradation of regulatory proteins, it fosters the following • Antiproliferation • Proapoptosis • Antiangiogenesis Proteasome Inhibitors: Mechanism Of Action
• Immunomodulators • Thalidomide • Lenalidomide • Pomalidomide • Induction of • Apoptosis • Antiproliferative effects • Inhibition of • Angiogenesis • Tumor necrosis factor • Interleukin-6 • Male and female have similar outcomes Immune Modulating Agents: Mechanism Of Action
• Melphalan alkylates the DNA nucleotide, guanine, and causes linkages between strands of DNA. • This chemical alteration inhibits DNA synthesis and RNA synthesis functions necessary for cells to survive. • These changes cause cytotoxicity in both dividing and non-dividing tumor cells. 1 Alkylating Agents
• Physiological changes during pregnancy affect drug distribution, metabolism, and excretion. • No pharmacokinetic studies have been conducted that aim to assess whether pregnant women should be treated with different chemotherapy doses. 1 • Most cytotoxic agents are known to cross the human placenta and reach the fetus circulation • Exposure to chemotherapy during the first trimester has been associated with a 10– 20% risk of major congenital malformations and a 33% risk of adverse pregnancy outcomes. 2 MM and Pregnancy
• Standard remains high dose chemotherapy followed by ASCT for patients with good performance status. • Autologous stem cell transplant has shown to improve survival. • Up-front transplantation with novel drug induction can induce high CR rates and increase quality of life • After short-course induction, with relapse after ASCT, patients can experience response to rescue therapies or retreatment. Autologous Stem Cell Transplantation (ASCT)
• Some of the trials fail to provide data on sub group analysis based on Sex and Gender, 1, 2 while the others showed no statistical difference in efficacy of currently practiced therapeutic drugs between males and females. 3, 4, 5 SEX AND GENDER BASED DIFFERENCE IN EFFICACY OF AVAILABLE THERAPEUTIC MODALITIES