Multiple Myeloma Multiple Myeloma Definition Malignant proliferation of






 on X Ray.")





















")
")












 – Preferred Tx in pts NOT going for")


- Slides: 46
Multiple Myeloma
Multiple Myeloma • Definition: Malignant proliferation of plasma cells derived from a single clone • Etiology: radiation; mutations in oncogenes; familial causes; role of IL 6 • Incidence/Prevalence: 14, 400 cases in 1996; incidence 30/1, 000 • Incidence increases with age • Males> females ; Blacks > Whites
Clinical Manifestations • Common – – bone pain and pathological fractures anemia and bone marrow failure infection due to immune-paresis and neutropenia renal impairment • Less common – – – acute hypercalcemia symptomatic hyperviscosity neuropathy amyloidosis coagulopathy
Clinical Manifestations • Bone Pain: – 70%, Precipitated by movement – Pathological fractures – Activation of Osteoclasts by OAF produced by myeloma cells • Susceptibility to infections: – Diffuse hypogammaglob. If the M spike is excluded – Poor Antibody responses , Neutrophil dysfunction – Pneumococcus, S. aureus, GN aerobes. Pneumonia, Pyelonephrits
Clinical Manifestations • Renal failure: 25% – – Multiple contributory factors Hypercalcemia, Hyperuricemia, recuurent Infections Tubular damage produced by Light chains type 2 proximal RTA, Non selective proteinuria • Anemia: 80% – Normochromic/Normocytic – Myelophthisis; Inhibition by cytokines produced by plasma cells. – Leukopenia/thrombocytopenia only in advanced cases.
Bone Disease • Lytic Lesions – 60% • Osteoporosis, Fx, Compression Fx – 20% • Myeloma Cells Produce Cytokines that: – Stimulate Osteoclastic Activity – Inhibit Osteoblastic Activity • Can be Detected by Plain Xray
Lytic lesions(Punched out lesions) on X Ray.
Vertebral collapse secondary to osteoporosis/pathological fracture
Normal bone Lesion Multiple myeloma: lesion in rib – Lab 11
Multiple myeloma: multiple lesions in skull – Lab 11
Renal Disease • Serum Cr Elevated in 50% and >2 in 20% at Diagnosis • Cast Nephropathy (Myeloma Kidney) – Large, Waxy Casts in Distal Tubules composed of Precipitated Light Chains • Not detected on Dipstick – SSA Test – Positive detected as the degree of turbidity when SSA added to urine suggests presence of nonalbumin proteins • Hypercalcemia • Amyloidosis
Case Report of Myeloma nephropathy • Bone marrow biopsy: 70% cellularity, increased atypical plasma cells comprising 60% of cellularity, c/w multiple myeloma
Epidemiology of Myeloma nephropathy • In two large multiple myeloma studies, 43% (of 998 pts) had a creatinine > 1. 5 and 22% (of 423 pts) had a Cr > 2. 0 • The one-year survival was 80% in pts with Cr < 1. 5 compared to 50% in pts with a Cr > 2. 3 • Prognosis is especially poor in pts who require dialysis
Causes of renal failure in MM • • Cast nephropathy Light chain deposition disease Primary amyloidosis Hypercalcemia Renal tubular dysfunction Volume depletion IV contrast dye, nephrotoxic meds
Myeloma Kidney • Two main pathogenetic mechanisms: – Intracellular cast formation – Direct tubular toxicity by light chains • Contributing factors to presence of renal failure due to multiple myeloma: – High rate of light chain excretion (tumor load) – Biochemical characteristics of light chain – Concurrent volume depletion
Cast Nephropathy • Most common pathological diagnosis on renal biopsy in multiple myeloma • Due to light chains binding with Tamm-Horsfall mucoprotein, which is secreted by tubular cells in ascending loop of Henle, forming casts • Multinucleated giant cells surround the casts • Dehydration worsens cast nephropathy due to decreased flow in tubules, increased concentration of light chains
Cast Nephropathy
Cast Nephropathy
Cast Nephropathy
Minimal diagnostic criteria for myeloma • >10% Plasma cells in bone marrow or plasmacytoma on biopsy • Clinical features of myeloma • Plus at least one of: – – – Serum M band (Ig. G >30 g/l; Ig. A >20 g/l) Urine M band (Bence Jones proteinuria) Osteolytic lesions on skeletal survey
Initial Work-up • CBC w/diff – peripheral smear – Normocytic, Normochromic Anemia most common – Rouleaux Formation >50% of patients • Chemistry (ca, alb, cr, LD, CRP, B 2 M) • SPEP – Monoclonal Protein • Serum Viscosity (if M-protein conc. Is high, >5 g/d. L) or sx of hyperviscosity are present • UA and UPEP • Metastatic bone Survey • Bone Marrow Biopsy
Rouleaux formation
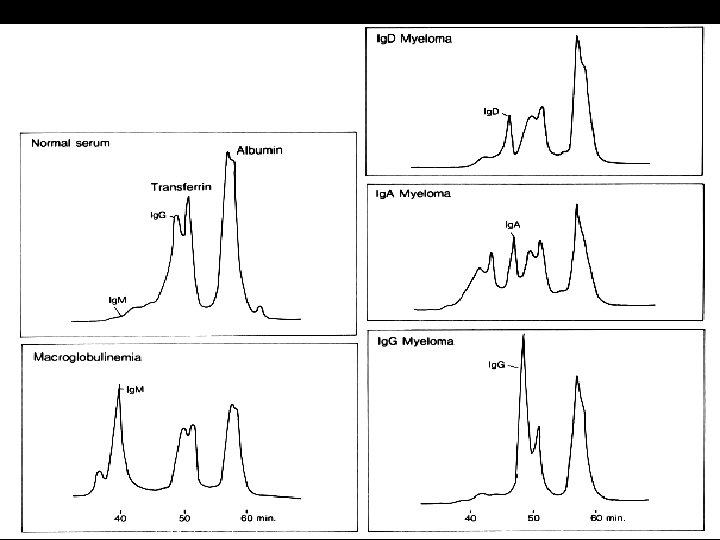
M protein • Amount of the M protein -marker of tumor load • Nature variable: – May be an intact molecule or a fragment – Extramedullary / Solitary plasmacytomas <1/3 have M spike – 20% of Myelomas _ only Light Chains produced – Non Secretory Myelomas_rare – frequency of myelomas : Ig G> Ig. A > Ig. D
1. Normal Plasma 2. Polyclonal Hyperglobulinemia 3. Monoclonal Spike 4. Bence Jones proteins in urine
Plasmapheresis in MM
Diagnostic Criteria • Presence of an M-Protein in serum and/or urine • Presence of clonal bone marrow plasma cells or plasmacytoma • Presence of Related Organ/Tissue involvement – Hypercalcemia, renal insufficiency, anemia, lytic bone lesions
Screening and Diagnosis • • • Blood and urine tests X-rays Magnetic Resonance Imaging (MRI) Computerized Tomography (CT) Bone marrow examination
Normal Cell (5%)
Myeloma Cells (10%)
Plasma Cell
Bone Marrow Aspirate
Bone Marrow Aspirate • Usually >10% plasma Cells, but can be from 5 -100% – ≥ 50% involvement – worse prognosis • Immunoperoxidase staining detects either kappa or lambda light chains, NOT both (confirming proliferation is monoclonal) • Immunophenotyping – Malignant Plasma Cells stain positive for CD 38, CD 56, and CD 138
Bone Marrow Biopsy
Staging • Stage 1 – Low amount of myeloma • Stage 2 – Medium amount of myeloma • Stage 3 – High amount of myeloma • A – Normal kidney function • B – Abnormal kidney function
International Staging System • Stage I – B 2 M <3. 5 mg/L and serum alb ≥ 3. 5 g/d. L • Stage II – neither stage I nor Stage III • Stage III – B 2 M ≥ 5. 5 mg/L
Staging 1. • Hb/Serum Ca/M component level/radiology – Stage I: Hb >10; Serum Ca < 12; Normal Bone survey; Low M component levels – Stage III: HB < 8. 5, Serum Ca >12; Lytic lesions+; High M component levels – Stage II : Intermediate • Divided into A or B depending on Serum Creatinine level < or > than 2 mg/dl.
Staging 2 • Serum b 2 microglobulin levels. • If < 0. 004 g/L : Stage 1; Median survival 43 months • If >0. 004 g/L: Stage II; Median survival 12 months
Prognostic Factors • • Performance status 3 0 r 4 Serum albumin < 3 g/d. L Serum Cr ≥ 2. 0 mg/d. L Platelet Count <150, 000 Age ≥ 70 years Beta-2 -microglobulin >4 mg/L Serum Calcium ≥ 11 mg/d. L Hemoglobin <10 g/d. L
Treatment • Options: – melphalan with or without prednisone – Infusional chemotherapy - vincristine and adriamycin infusion plus either dexamethasone all methylprednisolone – combination therapy - for example, adriamycin, carmustine, cyclophosphamide, and melphalan – weekly cyclophosphamide (“C weekly”)
Treatment • Prompt reduction in bone pain, anemia, hypercalcemia. • M component lags behind -4 -6 weeks to fall • 60% of patients will acieve a 75% reduction in tumor mass. • Treat q 4 -6 weeks for 1 -2 years. • Leads to a plateau phase- relapse within a year. • Maintenance: alpha Interferon ? ? ?
Treatment • Supportive therapy – analgesia – rehydration – treatment and any hypercalcemia – treatment of any renal impairment – treatment of any infection – local radiotherapy if required – chemotherapy – prevention of further bone damage
Treatment • Melphalan and Prednisone (Oral) – Preferred Tx in pts NOT going for BMT – 7 day course repeated q 6 weeks (x 3) – Objective response in 50 -60%, MS of 2 -3 yrs • Melphalan, prednisone, and Thalidomide – RR of 93% with 26% CR – When compared to above regimen, had better CR and RR; however, more toxicity • Thalidomide with or w/o Dexamethasone – Preferred in Candidates for BMT – For pts with Relapsed or Resistent Disease • VAD (Vincristine, Dex, and Adriamycin) • Radiation – Reserved for pts with focal process that has not responded to chemo
Treatment Outcomes • Cure – Not yet been Achieved • Molecular Complete Response – No evidence of Disease • Complete Response – No detectable M protein AND nml % of Plasma cells in Bone Marrow • Progressive Disease – >25% increase in M Protein, new bony lesions, or a new plasmacytoma
MGUS: Monoclonal gammopathy of undetermined significance • • No explained symptoms suggestive of myeloma Serum M protein concentration < 30 g/l < 5 percent plasma cells in bone marrow Little or no M protein in urine No bone lesions No anemia, hypercalcemia, or renal impairment M protein concentration and other results stable on prolonged observation