Multiple Myeloma By Dr Sameh Shamaa Multiple Myeloma

Multiple Myeloma By Dr Sameh Shamaa

Multiple Myeloma Epidemiology: • 1% Of all malignant diseases. • Annual incidence: 3 -4/100 000. • Age: - Median age: 65 y. - The diagnosis of MM in a patient < 30 y should only be made after careful evaluation of all data.
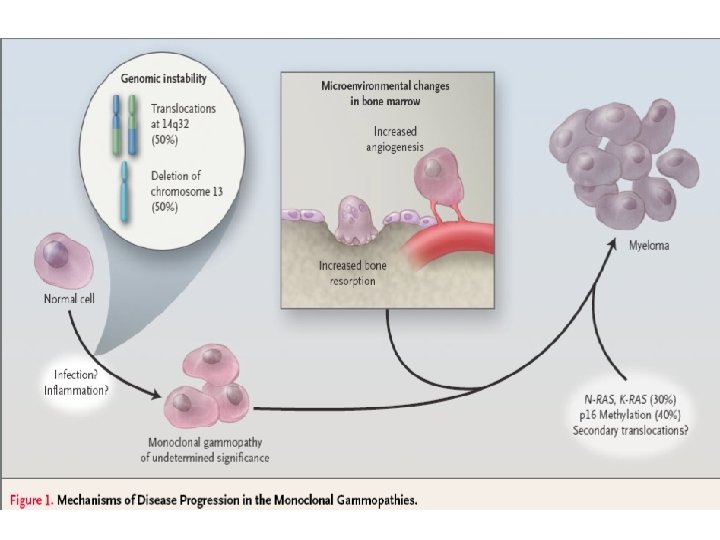
 OSTEOCLAST ACTIVATION OPG/OCIF Osteoclast RANKL/OAF Osteoblast/ stromal cell /tumour")
OC precursor OAF receptor (RANK) OSTEOCLAST ACTIVATION OPG/OCIF Osteoclast RANKL/OAF Osteoblast/ stromal cell /tumour cells/ myeloma Teitelbaum Science 2000

MULTIPLE MYELOMA: Clinical Picture

Bone Marrow Failure: *Anemia: usually normocytic normochromic : due to marrow infiltration and plasma volume expansion. *Neutropenia is frequent(++ susceptibility to infection). *Thrombocytopenia is rare.

Bone Disease: Skeletal lytic lesions, with or without osteoperosis, wedging or collapse of vertebral bodies or pathological fractures. Renal Failure: In 20 -40% of cases, due to: -BJP, and/0 r hypercalcemia (in 95% of cases). -Other causes: hyperuricemia, hypeviscosity, sepsis& nephrotoxic drugs.

Hypercalcemia: Secondary to osteolysis----->polyurea, and polydypsia may lead to severe dehydration Hyperviscosity: usually associated with Ig. M M-protein---- ocular, hemostatic, and neurological disturbances. Coagulopathy: either: -Hemorrhage: due to interference with action of clotting factors and platelets. -Thrombosis: due to acquired protein C deficiency.

Immune Paresis: -In 70% of patients with Ig. G MM, 40% of Ig. A MM and 20% of acses with BJP MM but cell mediated immunity is intact. So----- incresed risk of bacterial sepsis. Amyloidosis: In less than 5% of MM cases: more common with BJP and Ig. A MM-- deposition of amyloid material-- congesive heart failure, Carpal tunnel syndrome, macroglossia, gastrointestinal disturbances and europathies. , renal amyloidosis.

MULTIPLE MYELOMA Lab investigation : • ESR: very high. • Serum protein electrophoresis: M-band. • Immunofixation or immunoelectrophoresis: are confirmatory studies to define M-protein heavy and light chain classes.

MULTIPLE MYELOMA Lab investigation : • Serum Ca: often. • Serum creatinine: often. • Anaemia (not obligatory): (rouleaux formation of RBCs). • In uninvolved immunoglobulins. • +BJP in 24 hr urine collection (monoclonal light chains).
 • >10 % myeloma cells. .")
MULTIPLE MYELOMA BM PICTURE: (Aspirate & Trephine Biopsy) • >10 % myeloma cells. . • More basophilic cytoplasm. • Increased mitotic figures or multiple nuclei. • Coarse chromatin. • Plasma cell nests.

MULTIPLE MYELOMA Immunophenotyping: • CD 38 +ve. • CD 19, 20, 22 -ve. • Intracytoplasmic Ig +ve. • s. Ig -ve.

MULTIPLE MYELOMA RADIODIAGNOSIS: • Radiological survey of the entire skeleton: is mandatory. • MRI: is superior to CT for screening the vertebral column for osteolytic lesions. • Bone scan: is not indicated (cold lesions). • REMEMBER!! Iodine-containing contrast media may cause acute renal failure in case of paraproteinaemia.

MM: SWOG Criteria for Diagnosis: (At least 1 major + 1 minor or 3 minors) Major Criteria: (1) Plasmacytoma on tissue biopsy (2) Marrow plasmacytosis > 30 %. (3) Monoclonal protein: Ig G > 3. 5 g / dl. Minor Criteria: Ig A > 2 g / dl. BJP > 1 g / 24 hr. (1) Marrow plasmacytosis 10 -29 %. (2) Monoclonal protein present but less than the above levels (3) Lytic bone lesions (4) Decrease in uninvolved Ig: Ig M < 50 mg / dl. Ig A < 100 mg / dl. Ig G < 600 mg / dl.
 Staging (2) -2 microglobulin most significant) (3) CRP (reflect")
MULTIPLE MYELOMA Prognostic Factors (1) Staging (2) -2 microglobulin most significant) (3) CRP (reflect IL-6 activity) (4) PCLI (5) Cytogenetics (6) LDH
 (mo)")
MM: Prognostic Factors Risk Group 2 M & CRP Level M. S. (mg/l) (mo) Low-risk Both <6 54 Intermediate 2 M <6 27 High-risk Both >6 6 or CRP

MM: Prognostic Factors Cytogenetics: • Cytogenetics abnormalities occur in 80 -90% of patients. • FISH is the best technique to discover them. • Del 13 (partial or complete) & t involving 11 q are associated with poor prognosis in ABMT patients only. • Hypodiploidy is associated with drug resistance. • Any abnormal karyotype leads to inferior outcome with standard therapy.

MM Treatment Options • • • Chemotherapy High dose-therapy with transplant Radiation Maintenance therapy (e. g. alpha interferon, prednisone) Supportive care for – Anaemia – Pain – Bone disease (Bisphonates) – Hypercalcemia – Antibiotics – Emergency care (e. g. dialysis, plasmapheresis, surgery) • Management of drug-resistant or refractory disease • New and emerging treatments

Treatment of MM Use of Bisphonate in MM: Mechanism of action: 1. Decrease IL-6 release 2. Direct effect on Myeloma (may slow tumor growth) 3. Effect of angiogenesis

Treatment of MM Radiotherapy: Indications: • Big osteolytic lesions. • Significant osteolytic lesions in weight-bearing bone (for fear of pathological fracture). • Cord compression. • Extramedullary plasmacytoma.

Survival of Multiple Myeloma patients • • No treatment: 3 -6 months Conventional chemotherapy: 3 years Chemotherapy + IFN-α: 3 years ± 6 months Auto transplant: 5 years 25% dies within 1 st year 25% survival 8 years No cure by conventional chemotherapy
- Slides: 24