Multiple Chemical Sensitivity Toxicological Mechanisms and Therapeutic Approaches

, fibromyalgia")












")









. LTP")
 Retrograde Messenger NMDA stimulation (postsynaptic")


















 4. Autism 5. Overtraining Syndrome")
 4. Autism 5. Overtraining Syndrome")

- Slides: 55
Multiple Chemical Sensitivity: Toxicological Mechanisms and Therapeutic Approaches Martin L. Pall Professor Emeritus of Biochemistry and Basic Medical Sciences, Research Director, 10 th Paradigm Res. Group
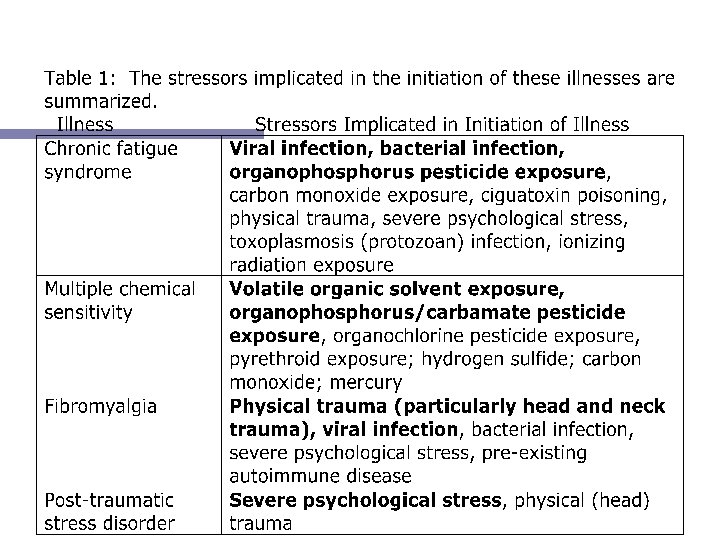
A large number of research groups have proposed that chronic fatigue syndrome (CFS), fibromyalgia (FM), multiple chemical sensitivity (MCS) and, in some cases, posttraumatic stress disorder (PTSD) have multiple overlaps and may share a common etiology (cause). They have: Øoverlapping symptoms Ømany people are diagnosed as having more than one Øcases of each are commonly initiated by a short term stressor presumably inducing these chronic conditions. Gulf War syndrome exhibits elements of all four.
The notion that CFS, MCS. PTSD and FM and several other diseases may share a common etiology has been proposed by Miller, who asked: "Are we on the threshold of a new theory of disease? " Toxicol Indust Health 1999; 15: 284 -294
For example, Buchwald and Garrity concluded in a study of CFS, MCS and FM patients that: "despite their different diagnostic labels, existing data, though limited, suggests that these illnesses may be similar if not identical conditions…. " Arch Inter Med 1994; 154: 2049 -2053.
Donnay and Ziem proposed that CFS, FM and MCS "may simply reflect different aspects of a common underlying medical condition. " J Chronic Fatigue Syndr 1999; 5: 71 -80.
The scientific literature reports that complete recoveries from CFS and FM do occur but are relatively rare. Only about 10% of the CFS and FM patients have a full recovery, although this typically take several years. Full recoveries from MCS rarely if ever occur, although MCS sufferers do report improved symptoms if they are able to avoid exposures to the classes of chemicals that produce sensitivity symptoms.
This talk will focus on MCS. However the comparison with these other multisystem illnesses is also useful with each shedding light on the mechanisms of the others. One of the great puzzles about MCS is how can the diverse chemicals that are implicated in initiating cases of MCS and producing sensitivity responses in those already sensitive, produce a common response in the body? ? Some of the MCS skeptics, including Ronald Gots, have argued that there cannot be a common response to such a broad group of chemicals. I will show here that they are wrong about that.
Chemicals reported to initiate cases of MCS include the following: ØOrganic solvents and related compounds. ØOrganophosphorus/carbamate pesticides. ØOrganochlorine pesticides ØPyrethroid pesticides Ø Ø Ø but also: Hydrogen sulfide Carbon monoxide Mercury
Chemical Action in MCS
We also know that members of each of these four classes of chemicals, the organic solvents and the three classes of pesticides, when tested in experimental animals, the following has been shown: One can greatly lower their toxicity in the body by treating with an NMDA antagonist. This shows not only that increased NMDA activity is produced by these chemicals but that this increased activity has a major role in producing the toxic responses in the body!
What about the other three chemicals that also initiate cases of MCS? ? These are also known to have similar toxicological properties: Hydrogen sulfide, carbon monoxide and mercury (acting through its product, methylmercury) can each produce increased NMDA activity; and one can use NMDA antagonists to lower the toxic responses to all three of these!
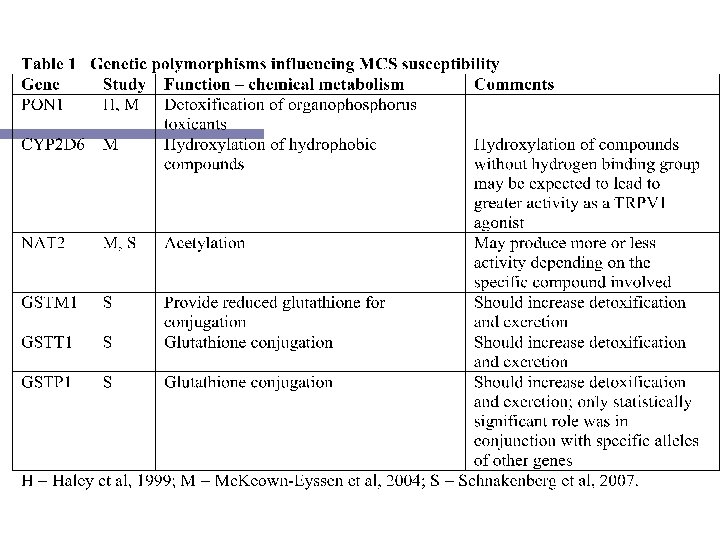
Six other observations supporting an NMDA role in MCS: 1. MCS patients are sensitive to monosodium glutamate and glutamate is the physiological agonist of the NMDA receptors. 2. An allele of the CCK-B receptor gene that produces increased NMDA activity is associated with increased prevalence and therefore incidence of MCS. 3. The NMDA antagonist dextromethorphan is reported from clinical observations to produce lowered response to chemical exposures in MCS patients. 4. Bell and others have proposed that neural sensitization has a key role in MCS and the probable mechanism for such neural sensitization, called long term potentiation, is known to involve increased NMDA activity. 5. Elevated NMDA activity has been shown to play an essential role in several animal models of MCS. 6. Elevated NMDA activity appears to play a role in such related illnesses as fibromyalgia, chronic fatigue syndrome and post-traumatic stress disorder, with the most extensive evidence for such a role being found in fibromyalgia (Pall, 2006 and 2007 a). Compelling evidence for a common toxicological response
One thing that you should note from the preceding discussion is that the receptors for these various toxic chemicals are NOT the olfactory receptors. It has been repeatedly stated that MCS is a response to odors, but this is not the case! And MCS sufferers with their nasal passages blocked off still react to chemicals. Some MCS patients are anosmic, completely lacking any sense of smell. I am not saying that the olfactory system is never impacted in MCS, but rather that the basic mechanism is not olfactory.
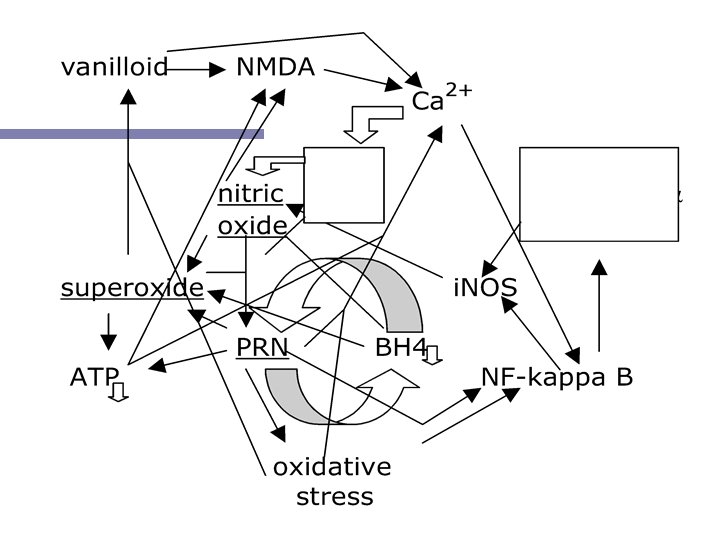
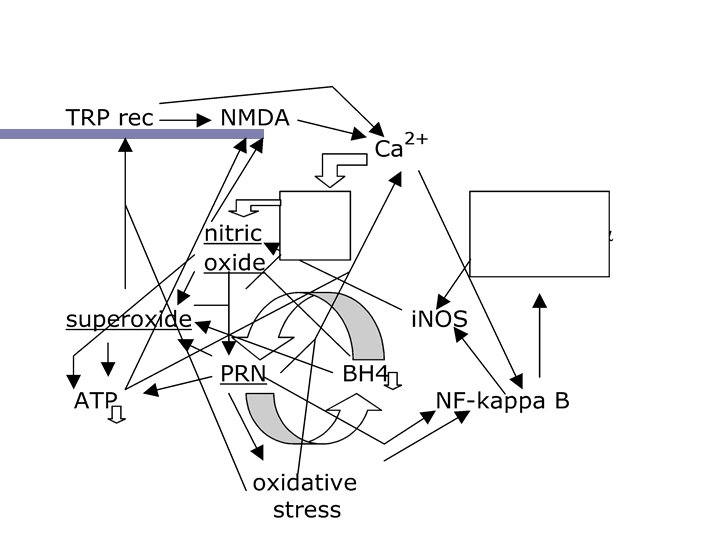
The etiologic theory I will be discussing focuses on nitric oxide and its oxidant product peroxynitrite, a potent oxidant. . NO + . OO- Nitric superoxide ONOO peroxynitrite
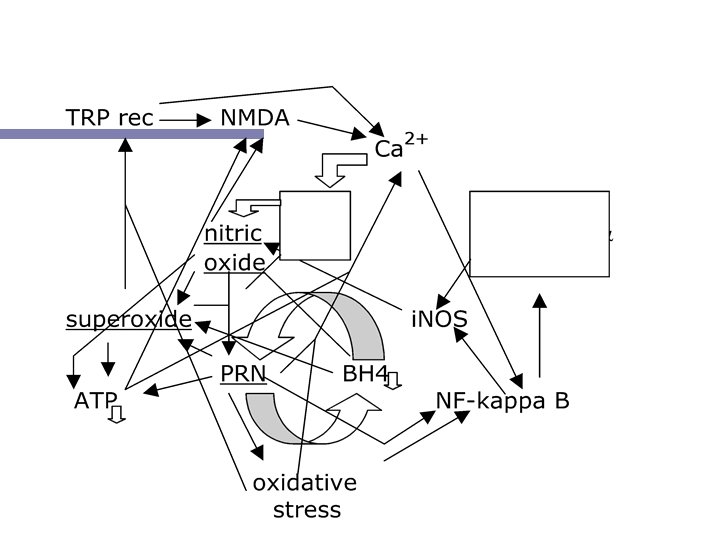
The Nitric Oxide - Peroxynitrite Vicious Cycle (NO/ONOO- Cycle)
Two mechanisms intimately involved with the NO/ONOOcycle Mitochondrial/energy metabolism dysfunction: Peroxynitrite attacks a number of components of mitochondria, including several iron-sulfur proteins. It also depletes NAD/NADH pools through stimulation of poly ADP-ribosylation. Nitric oxide inhibits cytochrome oxidase activity and superoxide also can lead to mitochondrial dysfunction. Nitric oxide synthases become uncoupled when deprived of tetrahydrobiopterin (BH 4), synthesizing superoxide in place of nitric oxide. This can lead to increased peroxynitrite synthesis, which oxidizes, in turn, BH 4 (a potential vicious cycle). This may be the core of the NO/ONOO- cycle!
Five Principles 1. Short-term stressors initiate these multisystem illnesses by stimulating nitric oxide or other cycle elements. 2. The increases in NO and peroxynitrite initiate the NO/ONOO- cycle which then causes these chronic illnesses. 3. The symptoms and signs of these illnesses are caused by the elevated elements of the NO/ONOO- cycle, nitric oxide, superoxide, peroxynitrite, NF-k. B, oxidative stress, vanilloid activity, NMDA activity, etc. 4. The basic biochemistry of the cycle is local, because nitric oxide, superoxide and peroxynitrite have limited half lives in biological tissues and because the positive feedback mechanism that maintain the cycle act at the cellular level. 5. Therapy should focus on down-regulating parts of the NO/ONOO- cycle, rather than on symptomatic relief.
Table 14 -1 Major Disease Paradigms 1. Infectious diseases. 2. Genetic diseases. 3. Nutritional deficiency diseases. 4. Hormone dysfunction diseases. 5. Allergies. 6. Autoimmune diseases. 7. Somatic mutation/selection (cancer). 8. Ischemic cardiovascular diseases. 9. Amyloid (including prion) diseases. 10. NO/ONOO- cycle diseases
Table 14 -1 Major Disease Paradigms 1. Infectious diseases. 2. Genetic diseases. 3. Nutritional deficiency diseases. 4. Hormone dysfunction diseases. 5. Allergies. 6. Autoimmune diseases. 7. Somatic mutation/selection (cancer). 8. Ischemic cardiovascular diseases. 9. Amyloid (including prion) diseases. 10. NO/ONOO- cycle diseases
In Chapter 3 of my book, I discuss sixteen symptoms and signs that occur in some but not all cases of these four illnesses (MCS, CFS, FM and PTSD), providing plausible mechanisms for each based on the action of one or more elements of the NO/ONOO- cycle. Many of these are summarized on the next two slides. It should be noted that these mechanisms for generation of these symptoms and signs are plausible mechanisms, based on known and well-described processes but they have not yet been clearly shown to be demonstrated to occur in these illnesses.
Symptom or Sign: Proposed Cause: Fatigue Peroxynitrite attack on energy metabolism Immune dysfunc. Inflamm. cytokines, oxidative stress, tion, low NK cell superoxide function Learning and Elevated brain nitric oxide, low energy memory dysfunction metabolism in brain Orthostatic intolerance Nitric oxide-mediated vasodilation and nitric oxide influence on autonomic activity. Pain (often multi. Roles for all of the elements of the NO/ Organ) ONOO- cycle Depression Inflamm. cytokines, nitric oxide
Symptom or sign: Anxiety Proposed Cause: Excessive NMDA activity in the amygdala region of the brain Sleep dysfunction Inflamm. cytokines; nitric oxide; NF-k. B Oxidative stress Peroxynitrite Abnormal SPECT Peroxynitrite-mediated oxidative stress; scans (brain) blood flow effects of nitric oxide and peroxynitrite Abnormal PET Energy metabolism effects of peroxy- scans (brain) nitrite; blood flow changes (see above)
Each of these four illnesses also have symptoms that are considered to be specific for that particular illness. I am not going to discuss how the specific symptoms of CFS, FM or PTSD may be generated by the NO/ONOO- cycle; rather the rest of this presentation will focus on the issue of how the specific symptoms of MCS may be generated. There have been many difficult puzzles about the reported properties of MCS. These include: How can people with MCS can be so extremely sensitive to such a broad range of chemicals, on the order of 1000 times more sensitive than normals? And how can previous chemical exposure generate such high level sensitivity?
One of the big breakthroughs in our understanding of MCS came from a comparison of the NO/ONOO- cycle model of these illnesses with the neural sensitization model of MCS developed by Dr. Iris Bell (M. D. , Ph. D. , at the University of Arizona). Bell argued that the most important mechanism of MCS was neural sensitization in the hippocampus region of the brain. This is the same region that has key functions in learning and memory. The idea Bell developed was that the synapses in the brain, the contacts between neurons by which one stimulates another, may become both hypersensitive and hyperactive in response to chemical exposure. The basic idea here is that this process of neural sensitization which is involved on a very selective basis in learning and memory, appears to be activated massively in MCS.
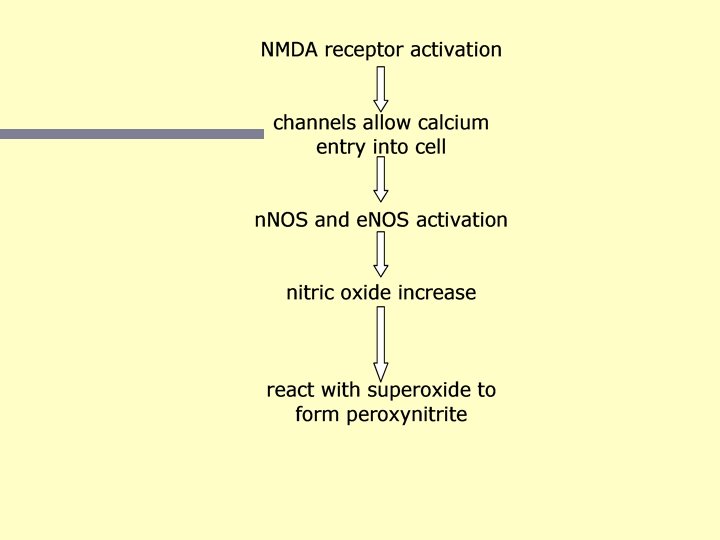
The main mechanism of neural sensitization is known as long term potentiation (LTP). LTP is known to involve increased NMDA receptor activity, increased intracellular calcium nitric oxide and also superoxide. So one immediately sees major connections between the NO/ONOO- cycle mechanism and the neural sensitization mechanism developed by Bell. So by having chemicals producing increased NMDA activity, one can see how they could greatly stimulate the long term potentiation mechanism. Several of the elements of the NO/ONOOcycle have roles in LTP, including NMDA activity, intracellular calcium, nitric oxide and superoxide. An oversimplified diagram of how some of this may play out is shown on the next slide.
Neural Sensitization Cycle Stimulation of Neurotransmitter Release (presynaptic cell) Retrograde Messenger NMDA stimulation (postsynaptic cell) Increased Nitric Oxide Increased Peroxynitrite ATP (energy) depletion
There are 7 mechanisms that may have important roles in generating the chemical sensitivity reported in MCS: Chemical action to increase NMDA activity in regions of brain where the NO/ONOO- cycle is already up-regulated due to previous chemical exposure. Nitric oxide acting as a retrograde messenger, increasing NMDA stimulation. Peroxynitrite acting to decrease energy metabolism, producing increased NMDA sensitivity to stimulation. Peroxynitrite acting to decrease energy metabolism, producing less transport of glutamate, leading to increased NMDA stimulation. Nitric oxide, acting to inhibit cytochrome P 450 metabolism of chemicals, leading to increased chemical accumulation. Peroxynitrite, producing breakdown of the blood brain barrier, leading to increased chemical access to the brain. Oxidants and superoxide, leading to increased vanilloid activity, producing increased sensitivity to organic solvents.
Dr. William Meggs, a physician scientist on the medical faculty in North Carolina has described studies that he and others have made showing chemical sensitivity in other regions of the body. This peripheral sensitivity occurs in the lower lungs, in the upper respiratory tract, in the skin and in the gastrointestinal (GI) tract. These sensitivity responses are initiated by previous chemical exposure and the chemicals involved are similar to those involved in central (brain) sensitivity. This suggests that similar mechanisms are involved. Some MCS patients have each of these peripheral regions involved but others lack sensitivity in each of these regions. Meggs and also Heuser have reported two additional mechanisms involved in these peripheral sensitivities--called neurogenic inflammation and mast cell activation. Both of these are compatible with the NO/ONOO- cycle mechanism.
Are there any properties that one can measure that appear to clearly distinguish MCS patients from others? Bell (in Arizona) has reported on changes in brain EEG patterns in response to low level chemical exposure. Kimata (in Japan) has reported on changes in both NGF levels and histamine levels that may also be specific in MCS. Millqvist (in Sweden) has reported on increased cough sensitivity to the compound capsaicin in MCS patients. Shinohara (in Japan) reported chemical hypersensitivity reactions and Joffres (in Canada) reported changes in skin conductivity with low level chemical exposure. There a number of studies with nasal lavage measurements, showing that chemically sensitive individuals respond with increased inflammatory markers on chemical exposure. Each of these may be specific changes in MCS patients and each is compatible with the NO/ONOO- cycle model. These should be considered as possible “specific biomarkers” for MCS.
Therapy: Almost all of the relevant clinical trial studies have been on CFS and/or FM patients, rather than with MCS. Still, these studies have provided substantial important evidence supporting the NO/ONOO- cycle mechanism. For example, the antioxidants flavonoids, Ecklonia cava extract and ascobate have all be reported to be helpful, showing that oxidative stress has a substantial causal role in these illnesses. Similarly, several NMDA antagonists have been shown to be helpful; so has magnesium which lowers NMDA activity and pregabalin, an agent that indirectly lowers excitotoxicity including NMDA activity. All of these provide substantial evidence that excessive NMDA activity has a substantial causal role.
Agents lowering mitochondrial/energy metabolism dysfunction have been shown to be useful, including acetyl-carnitine/ carnitine and Coenzyme Q 10; hyperbaric oxygen and D-ribose also probably help with this, as well. It may be inferred that mitochondrial dysfunction has an important causal nrole in these illnesses as well. The potent nitric oxide scavenger hydroxocobalamin has been shown in a clinical trial to be helpful to CFS-like patients; there is evidence that it is not acting to allay a B 12 deficiency, suggesting that it may act to lower nitric oxide levels. Fish oil has been shown to be useful in clinical trials and it is known to be an effective antiinflammatory, lowering i. NOS induction and inflammatory eicosanoid synthesis; this suggests that excessive inflammation has an important causal role.
High dose, intravenous ascorbate has been shown to be useful in four clinical trials with CFS and one with MCS. It and also high dose folate which has also been tested in a clinical trial are known to help restore BH 4 levels, suggesting that BH 4 depletion also has a substantial causal role. In conclusion, clinical trials mostly with the CFS and FM with one for MCS, provide evidence for causal roles for each of the following: Oxidative stress, excessive NMDA activity, mitochondrial dysfunction with lesser but still suggestive evidence for a causal role from these studies along for nitric oxide, inflammatory responses and BH 4 depletion. It is difficult to see how this could be true unless the NO/ONOO- cycle or something very similar to it is the causal mechanism of this group of illnesses.
In my book, I discuss five different protocols developed by different physicians and scientists, using from 14 to 18 agents/classes of agents predicted to down-regulate the N/ONOO- cycle biochemistry. These seem to be considerably more effective than the individual agents discussed previously. But from the published descriptions, they still seem to fall short of curing these diseases. I wish to discuss an additional protocol, one that I developed with the Allergy Research Group, a nutritional support protocol that is entirely made up of over-the -counter nutritional supplements. It contains 22 different agents predicted to down-regulate the NO/ONOO- cycle biochemistry. The following is a description of unpublished observations, ones that are derived from physicians clinical observations and anecdotal reports – as with all such information, you should view these with substantial skepticism.
About 80 to 85% of sufferers appear to respond positively to the protocol. This percentage seems to be similar for CFS, FM or MCS patients or for those who suffer from multiple illnesses. Generally, improvements are maintained by those staying on the protocol, that is relapses are rare. The extent of improvement varies among sufferers with some having amazing improvements within three weeks or less, but others requiring longer time to see more modest improvement and some showing no distinct improvement. Surprisingly, many who have been ill for two decades or more and many who have been severely ill respond well to the protocol. Some of these respond quite rapidly. People who have high levels of mercury in their bodies do not tolerate the protocol, presumably because 4 out of 7 of the pills contain alpha-lipoic acid, an agent known to mobilize stored mercury.
I suggest that individuals start with one of the seven supplement combinations, for three days to determine whethere is any difficulty in tolerating it, before adding a second for three days and so forth. That way if there is a problem with tolerating a supplement combination, it can be dropped out before continuing. Not surprisingly, lack of tolerance seems to be most common in the MCS group, but even when two or three or even four are not tolerated, there seem to be improvements produced by those parts of the protocol that are well tolerated. I believe that to get a good clinical response, it is very important to avoid stressors that will otherwise up-regulate the NO/ONOOcycle. In the MCS group, clearly chemical exposure is the most important of these, but allergens including food allergens and psychological stress may play roles. Other illnesses bring other stressors into play, as well.
In general, even though positive and sustained improvement seems to be the rule, we are not seeing any substantial number of cures over periods of six months to a year. And yet if we understand the NO/ONOO- cycle adequately, we should be able to obtain substantial numbers of cures with a properly designed protocol. Why are we not seeing it here? ? My working hypothesis is that the central couplet, the reciprocal interactions of peroxynitrite and BH 4 depletion is not being adequately treated. peroxynitrite BH 4 depletion There agents that are predicted to help lower this couplet, but it is not clear that they work very well!
My candidate for an approach that may adequately down-regulate this couplet is high dose, IV ascorbate (vitamin C), an agent that can work in three ways to help lower this couplet (and note the previously described clinical trials on IV ascorbate): 1. Ascorbate is a peroxynitrite scavenger although it is unclear that it is effective at the normal levels obtained in the blood from oral ascorbate. However IV ascorbate can give levels 30 times or more these levels – may be vastly more effective! 2. The oxidation product produced by peroxynitrite from BH 4 is BH 3 and BH 3 can be reduced back to BH 4 by ascorbate – again high doses may be particularly effective! 3. High dose ascorbate generates hydrogen peroxide in the body which induces the enzyme GTP cyclohydrolase I which is the first and rate limiting enzyme in the de novo synthesis of BH 4. So may help increase BH 4 availability in that way.
Evidence: How much evidence provides support for the NO/ONOOcycle mechanism of MCS? In my key FASEB Journal paper, I described 10 discrete types of evidence for a role of increased nitric oxide and peroxynitrite in MCS. These ranged from evidence that organic solvents can produce increases in nitric oxide, evidence for oxidative stress (presumably from peroxynitrite), evidence from an animal model for an important causal role of nitric oxide and evidence for an important NMDA role (it is known that NMDA stimulation produces increases in nitric oxide and peroxynitrite). More recent evidence, as you have seen, links each of the chemical classes of initiating chemicals to increases in NMDA activity and therefore nitric oxide and peroxynitrite. The reported blood brain barrier breakdown in MCS, presumably caused by peroxynitrite, is a 12 th type of evidence.
Ashford and Miller in their important 1998 book on MCS listed 10 “striking similarities” between MCS and neural sensitization, each providing evidence that neural sensitization has a role in MCS. Dr. Julius Anderson and I have provided 12 types of evidence implicating the TRPV 1 (vanilloid) receptor to MCS in our paper on that receptor. 13 types of evidence implicating increased NMDA activity. There are now at least 47 distinct types of evidence, each providing support for important properties of the NO/ONOO- cycle mechanism of MCS.
A mechanism, like that of the NO/ONOO- cycle must be judged not just by the evidence that may support it, but also as an explanatory model. Can it provide explanations for the puzzling features of whatever it claims to describe? In this case, we need to ask, how well does the NO/ONOO- cycle mechanism explains each of the most puzzling features of MCS? The NO/ONOO- cycle mechanism is stunningly successful as an explanatory model of MCS. It provides explanations, for each of the most puzzling features of MCS. Let’s go through them one at a time.
How do the four classes of chemicals implicated in MCS initiate these illnesses and trigger sensitivity symptoms? They each act via known pathways to produce increases in NMDA activity which produces, in turn, increased nitric oxide and peroxynitrite. Why are MCS patients so exquisitely sensitive to chemicals, on the order of 1000 times more sensitive than normals? Because of the action of six distinct mechanisms, five involving nitric oxide or peroxynitrite and the sixth involving superoxide. It is the combination of these mechanisms acting together that produce this extreme level of sensitivity.
There also five specific puzzles that need to be explained. Most of these we have not discussed. The possible specific responses of MCS patients to chemicals that I discussed as possible biomarkers. Already discussed--each can be explained as a being linked to the NO/ONOO- cycle mechanism. The role of such aspects as neurogenic inflammation and mast cell activation in peripheral sensitivity. Also consistent with mechanism--this was documented in my Environmental Health Perspectives article on MCS. Changes in porphyrin metabolism in MCS patients can also be explained. Also consistent with mechanism - discussed in article.
The role of mold toxins in the initiation of cases of MCS has never been explained. Anderson and I proposed that because some mold toxins are known to stimulate the TRPV 1 receptor, that molds may act by that pathway in this process. The vanilloid receptor also explains the phenomenon of desensitization/masking in MCS (also discussed in the Pall and Anderson article).
Why are the four types of illnesses, MCS, CFS, FM and PTSD so often diagnosed together in the same patients? (Why are they comorbid? ) Because they share a common cause--the NO/ONOO- cycle. Why are these four illnesses all chronic? Because the NO/ONOO- cycle is a vicious cycle, propagating itself over time. How are the symptoms and signs of these illnesses generated? They are produced through the action of the elements of the NO/ONOO- cycle. Why is there so much variation in symptoms from one patient to another? Because of the variation in tissue distribution of the underlying biochemistry. Different patients have different regions of their bodies impacted, and differ from each other in symptoms, for this reason.
1. Tinnitus 2. Post-Radiation Syndrome 3. Multiple Sclerosis (MS) 4. Autism 5. Overtraining Syndrome 6. Silicone Implant Associated Syndrome 7. Sudeck’s Atrophy 8. Post-Herpetic Neuralgia (Pain) 9. Chronic Whiplash Associated Disorder 10. Amyotrophic Lateral Sclerosis (ALS) 11. Parkinson’s Disease 12. Alzheimer’s Disease 13. Asthma 14. Irritable Bowel Syndrome Other proposed NO/ONOO- cycle diseases from my book
1. Tinnitus 2. Post-Radiation Syndrome 3. Multiple Sclerosis (MS) 4. Autism 5. Overtraining Syndrome 6. Silicone Implant Associated Syndrome 7. Sudeck’s Atrophy 8. Post-Herpetic Neuralgia (Pain) 9. Chronic Whiplash Associated Disorder 10. Amyotrophic Lateral Sclerosis (ALS) 11. Parkinson’s Disease 12. Alzheimer’s Disease 13. Asthma 14. Irritable Bowel Syndrome The colored diseases also are initiated by solvents and pesticides.
Table 14 -1 Major Disease Paradigms 1. Infectious diseases. 2. Genetic diseases. 3. Nutritional deficiency diseases. 4. Hormone dysfunction diseases. 5. Allergies. 6. Autoimmune diseases. 7. Somatic mutation/selection (cancer). 8. Ischemic cardiovascular diseases. 9. Amyloid (including prion) diseases. 10. NO/ONOO- cycle diseases