MSQH Accreditation Standards 5 th Edition Training STANDARDS











 12. To")









































 Discussed")










































- Slides: 98
MSQH Accreditation Standards 5 th Edition Training STANDARDS 9 B, 10 and 11 14 th November 2019 MSQH, Wisma Sejarah
SERVICE STANDARD 9 B : CLINICAL SERVICES – SURGICAL RELATED SERVICES
SERVICE STANDARD 10 : Anaesthesia Services
SERVICE STANDARD 11 : Operation Suite Services
MSQH HOSPITAL ACCREDITATION STANDARDS It is a Management Framework that ensures proper utilization of resources, quality control and patient centered care.
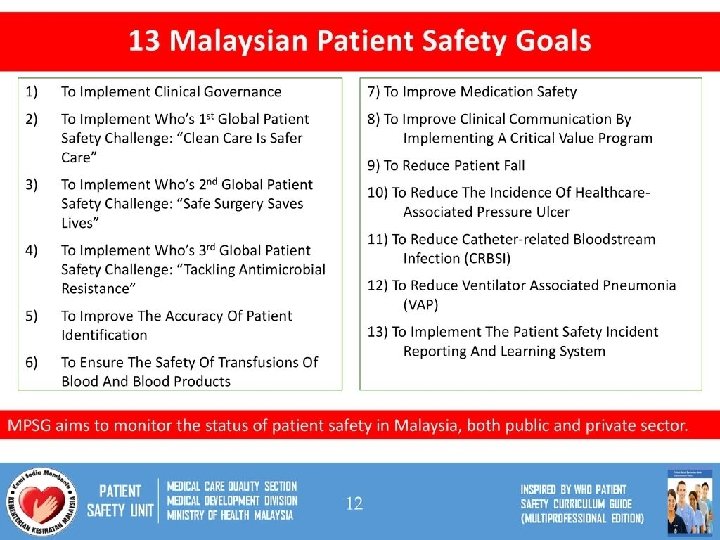
13 Malaysian Patient Safety Goals 1. To implement Clinical Governance Clinical governance is a framework through which healthcare teams are accountable for the quality, safety and satisfaction of patients in the care they deliver. A key characteristic of clinical governance is a culture and commitment to agreed service levels and quality of care to be provided.
13 Malaysian Patient Safety Goals 2. To implement WHO’s 1 st Global Patient Safety Challenge: “Clean Care is Safer Care” 3. To implement WHO’s 2 nd Global Patient Safety Challenge: “Safe Surgery Saves Lives” 4. To implement WHO’s 3 rd Global Patient Safety Challenge: “Tackling Antimicrobial Resistance”
13 Malaysian Patient Safety Goals 2. To implement WHO’s 1 st Global Patient Safety Challenge: “Clean Care is Safer Care” Deals with the challenge of reducing health care-associated infections (HCAIs). To promote best hand hygiene practices globally, at all levels of health care, as a first step in ensuring high standards of infection control and patient safety
13 Malaysian Patient Safety Goals 5. To improve the accuracy of patient identification 6. To ensure the safety of transfusions of blood and blood products 7. To improve medication safety
13 Malaysian Patient Safety Goals 8. To improve clinical communication by implementing a critical test and critical value program * 9. To reduce patient fall 10. To reduce the incidence of healthcare- associated pressure ulcer
To improve clinical communication by implementing a critical test and critical value program § Critical Test Measurement Parameter: Elapsed time from the time the test was ordered to the time the result (whether normal or abnormal) is reported to a responsible licensed care giver (that is, the turnaround time of the critical test). § Critical Result Measurement Parameter: Elapsed time from when the critical (abnormally high or low) result was determined to be critical to the result is first known to the time it is reported to the licensed responsible caregiver (that is, the
13 Malaysian Patient Safety Goals 11. To reduce Catheter-Related Bloodstream Infection (CRBSI) 12. To reduce Ventilator Associated Pneumonia (VAP) 13. To implement the Patient Safety Incident Reporting and Learning System
Definition of Accreditation The process of which an entity, separate and distinct from the hospital, (usually nongovernmental), assesses the hospital to determine if it meets a set of standards designed to improve quality and safety of patient care
Why the need for Accreditation? To ensure the correct implementation of health interventions according to established norms and procedures, which satisfy the health system’s clients and maximize health outcomes without creating health risks or unnecessary costs.
Benefits of Accreditation § Facility commitment to high professional standards of care § Allows a structured and comprehensive analysis of facility’s performance § Enhance safety, effectiveness and efficiency of operations. § Enhancement of teamwork and staff morale
Benefits of Accreditation § Identification of strengths and weaknesses as a source of information, guidance and support for improving the quality of its service. § Accountability to stakeholders the facility’s commitment to continuous quality improvement and safety in health care.
Areas for Assessment: 5 th Edition Format 1. Organization and Management 2. Human Resource Development and Management 3. Policies and Procedures 4. Facilities and Equipment 5. Safety and Quality Improvement Activities 6. Special Requirements
1. Organization and Management
STANDARD 9 B. 1. 1 ORGANIZATION AND MANAGEMENT § The Surgical Services shall be organised, directed and coordinated with other services in the Facility to provide a high standard of inpatient and outpatient care to the community in a safe, efficient, effective, evidence based and caring manner and with due regard for the needs, dignity and privacy of patients and confidentiality of their personal information. The Surgical Services shall be easily accessible and continuity of care assured.
1. Organization and Management § Looks at leadership and governance § Departmental activities – Resource management – Training/CME – Set Goals – Track Achievements – Review Progress § Evidenced by Minutes of meeting, etc
What documents does your Department need?
24
§ Your organizational documents – Describes your functions and services you provide § Your operational policies – Describes how you do deliver services § Your Protocols/ Work flows – Describes how work is carried out in step-wise manner § Your Work Census/Manpower – Describes how you organize your resources – Statistics need to displayed and tracked § Your Personnel Information – Personnel and Job Descriptions § Your KPI’s/ NIA’s – Describes how you ensure quality § Your Incident Reports – Describes how you manage failures
Organization and Management 1. 3 Criteria for Compliance § Regular staff meetings are held between Head of Service and staff to discuss issues and matters pertaining to the operations of the Services § Minutes are kept; decisions and resolutions made during meetings made accessible & communicated to all staff and implemented
Conducting Department Meetings § Call letter/Memo § Minutes of Previous Meetings § Agenda – Fixed matters for discussions • Issues related to dept. management, quality, patient care – AOB (=Any other business) § Attendance Sheet (+Absent/Representative)
Conducting Department Meetings § § Call letter/Memo Minutes of Previous Meetings Agenda Attendance Sheet (+Absent/Representative) § Order of Meeting Review of previous minutes Follow-up on actions taken § Matters discussed Actions to be taken Person responsible
Issues Organisation and Management Requirements Organisation chart Updated, reviewed and endorsed by PIC/HOD -At least once every 3 years Mission, Vision Updated, reviewed and endorsed by PIC/HOD Similar as Hospital’s mission and vision Goals and objectives Updated, reviewed and endorsed Regular department/unit meetings At least 2 x/ year Minutes acknowledge by staff MDAC meeting Know where to get copy of minutes Facility with educational programme Trained staff provide supervision, Memorandum of Understanding with institution, List of Clinical Instructor
Organization Chart § Show work responsibilities and reporting relationships. § Allow leadership to more effectively manage growth or change. § Allow employees to better understand how their work fits into the organization's overall scheme. § Improve lines of communication. § Create a visual employee directory
Dr Khalid Bin Ibrahim PENGARAH HOSPITAL Puan Suraya binti Mohammad Elias SETIAUSAHA PEJABAT GRED N 27 (PENGARAH) Dr Wan Nurzaty Iwanie bt Wan Mohamad En. Mohd Rizal Bin Abdullah Dr Aminuddin Bin Tauhid Pegawai Tadbir dan Diplomatik Gred M 52 TIMBALAN PENGARAH (PERUBATAN 1) TIMBALAN PENGARAH (PERUBATAN 2) Dr Ahmad Fahmi bin Ahmad Sahray TIMBALAN PENGARAH (PENGURUSAN) KETUA PENGARAH (KLINIKAL) Dr Norizan binti Rosli En. Muhammad Zhafir bin Mohd Noor KETUA UNIT CRC Puan Suzana bt Landahari (KEJURUTERAAN & PENSWASTAAN) SETIAUSAHA PEJABAT GRED N 27 (TIMB. PENGARAH) PENGURUSAN PERKHIDMATAN PERUBATAN Datuk Dr Christopher Lee (KETUA JABATAN PERUBATAN AM) Dr Ahmad Zabidin bin Zakaria PERKHIDMATAN PEMBEDAHAN Dr Mohammad Shukri Bin Jahit (KETUA JABATAN PEMBEDAHAN AM) Dr Lim Wee Leong (KETUA JABATAN ANAESTESIOLOGI & RAWATAN RAPI) (KETUA JABATAN PSIKIATRI & KESIHATAN MENTAL) Dr Akmal Hafizah Zamli (KETUA JABATAN PERUBATAN REHABILITASI) Dr Radhiah binti Mustafar @ Mokhtar (KETUA PENGARAH KANAN (PKKN)) Dr. Norli Marwayne bt Mohammed Noor ( KETUA JABATAN DERMATOLOGI) Dato’ Dr Azmin Kass Bin Rosman (KETUA JABATAN PEMBEDAHAN NEUROSURGERI) (KETUA JABATAN KECEMASAN DAN TRAUMA) Dr Sobani Bin Din (KETUA JABATAN OTORINOLARINGOLOGI) Dr Yun Sii Ing (KETUA JABATAN RADIOLOGI) Dr Afifah binti Haji Hassan (KETUA JABATAN PATOLOGI) Dr Shahidan Bin Md Noor (KETUA JABATAN FORENSIK) PERKHIDMATAN WANITA DAN KANAK PERKHIDMATAN SOKONGAN KLINIKAL Dr Norashikin binti Abdul Fuad Dr. Syamhanin bt Adnan (KETUA JABATAN OBSTETRIK & GINEKOLOGI) Dr Jamaluddin bin Haji Mohamad (KETUA JABATAN PEDIATRIK) Dr Kalaiarasu a/l M. Periasamy (KETUA JABATAN PEADEODONTIK) Dr Syed Iqbal bin Syed Husman (KETUA JABATAN MAXILO FASIAL) TARIKH KEMASKINI : 19 February 2018 (KETUA JABATAN DIETETIK DAN SAJIAN) Puan Rosalina Sabirin (KETUA JABATAN KERJA SOSIAL PERUBATAN) (Matron Harnake Kaur a/p Mehar Singh) Dr Salina Ibrahim (KETUA JABATAN OFTALMOLOGI) Encik Syamhairil bin Mohamed (KETUA UNIT PENDIDIKAN KESIHATAN) (KETUA JABATAN ORTOPEDIK & TRAUMATOLOGI) Dr. Shamala a/p Rethnasabapathy (KETUA JABATAN FARMASI) Puan Wan Ermiyati Wan Mohamad Dato’ Dr Zamyn Zuki Bin Mohd Zuki (KETUA JABATAN PEMBEDAHAN PLASTIK & REKONSTRUKTIF) Dr Sabariah Faizah Jamaluddin PERKHIDMATAN KLINIKAL DIAGNOSTIK (KETUA PENYELIA JURURAWAT) ORGANISATION Diluluskan Oleh : CHART En Mazlan bin Zakariya (KETUA PENYELIA HOSPITAL) (Matron Harnake Kaur a/p Mehar Singh) (KETUA UNIT PUSAT PENSTORAN PENSTERILAN) KJ Rozita binti Bahari (KETUA UNIT KAWALAN INFEKSI) PERKHIDMATAN SOKONGAN Dr Dang Siew Bing (KETUA UNIT KESIHATAN PEKERJAAN) Dr Geethapriya a/p Navaretnam (KETUA UNIT KLINIK KELUARGA & KESEJAHTERAAN) Dr Norazila bt Md Zainal Puan Hasanah Alamin KPP (PENGURUSAN & KEWANGAN) Puan Noorhafza bt Abu Bakar AKAUNTAN GRED W 44 (KETUA BHG, AKAUN) En. Nasrul Izani bin Ramli PENTADBIRAN & PEMBANGUNAN En. Zailan bin Othman (KETUA BHG. PEROLEHAN) (KETUA UNIT KUALITI) En. Balasuparmaniam a/l Narayanan (KETUA UNIT KESIHATAN AWAM) Pn Hamidah Karim (KETUA JABATAN REKOD PERUBATAN) Puan Faizatul Najwa binti Mohamad Rosni (KETUA BHG. SUMBER MANUSIA) Norhayati binti Jasni (KETUA UNIT KAUNSELING) Pn Kavitha A/P Somanaidu (KETUA BHG. TEKNOLOGI MAKLUMAT) Puan Shahrina Binti Abd Samad (KETUA PERHUBUNGAN AWAM)
Organizational Chart Design § Solid line - depict a formal and direct relationship between positions. § Rectangle - represents a person, position, or department. In a hierarchical organizational chart, the Chief Officer or is the top rectangle. The level underneath the chief officer contains high-level managers or executives, and each succeeding level includes the subordinates of the line above. § Dashed line - indicate an advisory or indirect relationship between positions, while arrows indicate the flow of communication.
STATISTICS OPERATIONS Hospital Sungai Buloh towards Accreditation Survey 7 -9 th May 2018
2. Human Resource Development and Management
2. Human Resource Development and Management § Looking at a Competent workforce § Qualifications, Licensing of healthcare providers, etc § Skills and competency, Credentialing and Privileging, Staffing ratios § Staff development, Continuous education Employee rights, work conditions
Human Resource Development and Management Issues Requirements PIC/HOD/Staff Appointment letter, TOR, qualification (APC, NSR, C&P) Continuing education plan Schedule available for all staff, training Staffing pattern Qualification, workload C&P All clinical staff Of surgeons made available in public folder with list of procedures privileged to do in OT/Daycare ‘Fail Meja’ For each staff (biodata, qualification, training records, leave, competency records, privileging, confidentiality) Orientation programme Policy, Hospital and specific to service, attendance Facility with external education programme C&P for outside specialist/consultant
Credentialing and Privileging Appropriately trained Achieved desired level of competency to perform the duties expected for the care giver.
Credentialing and Privileging To ensure competency requirements are met for specialists, medical officers, allied healthcare staff and those handling special equipment
Human Resource § Qualified Staff – Credentialling and delineation of privileges § Authorities and Responsibilities § Staff skill and knowledge development Programme § CME § Orientated
HUMAN RESOURCE AND MANAGEMENT 1. 2. 3. 4. 5. Credentialing and Privileging Job Description (File Meja) for all categories of staff Training, Education, Appraisal and Research Staffing level and Competency Staff Orientation Programme
CME’s/CNE’s
Credentialing …. a process whereby a professional preparation program meets the specific standards established by a credentialing body Ensures that the healthcare giver is competent to perform the duties expected of them
Certification and Privileging § Goal is for quality and safety § Credentialing verifies whether provider meets certain criteria relating to professional competence and conduct § Privileging authorizes access and delineates scope
Depending on the skills expected: Credentialing may take the form of: § Formal training and certifications • Lectures, training, exams • (Specialist, Post-basic ICU nursing, etc) § Institutional Training programmes – Supervised training (eg handling equipment) – For specific set of skills (APS nurse)
Certification § …a process by which a professional organization grants recognition to an individual who, upon completion of a competency-based curriculum, can demonstrate a predetermined standard of performance.
Certification “of competency” § Establishes a standard § Attests to individual’s knowledge and skills § Assists employers in identifying qualified and trained practitioners § Sense of pride and accomplishment § Promotes continued professional development
Nursing C&P § Formal Post-Basic Nursing Qualifications
CRITERIA FOR CREDENTIALING OF NURSES AND ASSISTANT MEDICAL OFFICERS 1. PERI-OPERATIVE CARE 2. INTENSIVE CARE NURSING 3. OPHTHALMOLOGY 4. EMERGENCY MEDICINE & TRAUMA SERVICES 5. DIALYSIS CARE: HAEMODIALYSIS / PERITONEAL DIALYSIS 6. PRE HOSPITAL CARE SERVICES 7. ENDOSCOPY SERVICES 8. GENERAL PAEDIATRIC NURSING 9. NEONATAL NURSING 10. ORTHOPAEDIC SERVICES 11. CARDIOVASCULAR PERFUSION 12. ANAESTHESIOLOGY & INTENSIVE CARE SERVICES: ANAESTHESIA / PERI-ANAESTHESIA / INTENSIVE CARE 13. PERI-ANAESTHESIA CARE (P. A. C)
3. Policies and Procedures
3. Policies and Procedures § Looks at management and patient care documents
Written POLICIES
REMEMBER Patient and Family rights policy applies across the board
STD 6 – Patient & Family Rights 1. Equal Access To Care Respect And Dignity 2. Privacy 3. Confidentiality 4. Consideration 5. Safety And Security 6. Pain Management 7. Information 8. Communication 9. Consent 1. Refusal of treatment and DAMA (Discharge against medical advice) 2. Transfer and Continuity of care 3. Hospital Charges 4. Organ Donation 5. Make Decisions About End-Of-Life Care 6. Agree or refuse to take part in
Procedures § § § § Flowcharts Protocols Care plans Regimens, tables, charts Fail Meja CPGs, Akta Garispanduan
Why documents are important § Directs how a service is to be delivered § Describes roles, duties and functions of caregivers § Ensures uniformity and quality in care provided § Addresses issues like: • Patient rights • Patient safety
Policies and Procedures Issues Requirements Policies and Procedures Updated, reviewed and endorsed (periodic) Discussed in meeting Acknowledge by staff Hospital wide policies made available in public folder Examples of general policies -Blood transfusion -Handling prisoner patients -Pain management policy -Incident report policy -C&P policy -Pharmacy policy including drug prescription, dispensing and administration -End of life care policy -Policy of handling unknown patients
Documents Protocols Policies Auditable General Plans/Manuals Procedures Operationa l Requireme nt Work Instruction Check List, Calculation sheet, Specific
Benefits of good documentation on how a service is to be P&Ps delivered • Ensures that laws/regulations are complied • Reduce errors or mistakes • Prevents irritation, complaints, frustration due to various interpretations 59
Know what the documents are intended for § Organization-wide § Department / Team § Job-specific • For administration • For health-care givers • For patients • Rights and Responsibiblties 60 P&Ps
Policies: Policies vs. Procedures: • Specific steps • Guidelines, and actions philosophies, principles • Give • State a position instructions/ protocol • Broad • Narrower, more • Why & what focused • How, when, who 61
Policies Procedures § Have widespread Application § Are nonnegotiable, change infrequently § Are expressed in broad terms § Are statements of what and/or why § Answer major operational issues § Have a narrower focus § Are subject to change and continuous improvement § Are a more detailed description of activities § Are statements of how, when and/o r who &
Why documents are important
What is a Policy A policy is a guiding principle used to set direction in an organization. It should be used as a guide to decision making under a given set of circumstances within the framework of objectives, goals and management philosophies. Usually reviewed once very three years or earlier if necessary
What is a Procedure? Procedures aim to describe how, when, and who of processes
What is a Procedure? A procedure is a particular way of accomplishing something. It should be designed as a series of steps to be followed as a consistent and repetitive approach or cycle to accomplish an end result
What are Clinical Practice Guidelines? § “Clinical practice guidelines are systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances. ” (Institute of Medicine, 1990)
4. Facilities and Equipment
4. Facilities and Equipment § Looks at physical structures, layout and equipment
Facilities and Equipment Issues Requirements Adequate facilities and equipment Proper space, storage, functionality Specialized equipment List of staff credential, privileged to use, letter of authorization Scheduled PPM & calibration For all equipment Exit route Clear route, signage Asset inventory Stickers, Complaint records Relevant standards and building by laws Eg SIRIM standards, OSHA, JKKP, Bomba Regulations, EPA waste collection and removal Space Adequate and proper utilisation Risk management Error prevention & recovery mechanism (contingency plan)
Facilities & Equipment § Adequate facilities and equipment available for running of service – Adequate number – Functionality – Serviced and calibrated § Documented evidence that equipment used comply with standards (SIRIM)
Facilities & Equipment § Qualified staff operates equipment § General safety of the facilities – Fire, electrical, water, gases – UPS and Emergency supplies – Monitoring & alarm system – Error prevention – Rescue & recovery
Includes environment
Infection Control in the ICU The most important part of tuberculosis infection control is getting the patient into the isolation room. Wurtz, 1996, ICHE
TRANSMISSION-BASED PRECAUTIONS CATEGORIES § Contact Precautions are designed to reduce the risk of transmission of microorganisms by direct or indirect contact. § Examples of Diseases: gastrointestinal infections (including diarrhea of unknown origin), wound and skin infections (e. g. impetigo) and colonization with multidrugresistant bacteria (e. g. methicillin-
TRANSMISSION-BASED PRECAUTIONS CATEGORIES § Droplet Precautions are designed to reduce the risk of droplet transmission of infectious agents. Infectious droplets are released when the infected person sneezes or coughs and the large droplet spray may spread as far as three feet. § Examples of Diseases: Influenza, meningococcal meningitis, mumps, rubella, diphtheria, pneumonic plague, pertussis and infections caused by
TRANSMISSION-BASED PRECAUTIONS CATEGORIES § Airborne Precautions are designed to reduce the risk or eliminate the airborne transmission of infectious agents. The infectious particles are so small that they can remain suspended in the air for long periods of time and are carried on air currents. § Examples of Diseases: varicella (chickenpox), tuberculosis, measles.
Isolation Rooms Negative air pressure § Prevent airborne diseases from escaping the room and infecting other people. § In a negative air pressure room, you may be able to feel air being sucked into the room under a closed door or through a slightly opened window. Positive air pressure § When a person has a weakened immune system, positive air pressure may be used. This is done to keep contagious diseases
Airborne transmission isolation room • Negative Pressure Isolation room • One Isolation room per 6 ICU beds • Negative pressure (2. 5 Pa) • > 12 air changes per hour • Exhaust air outside or re-circulated HEPA filters • Dedicated hand-washing facilities • Decontamination zone • Ask for Policies and Protocols
5. Safety and Quality Improvement Activities
Fire safety: Fire Escape Route
Fire safety
Fire safety
Fire safety: Wet cell batteries supply to UPS short-circuited
5. Quality Improvement Activities § Clinical care • Clinical indicators, Infection control, etc § Quality improvement and Safety § Reduction in medication errors, etc
Safety and Performance Improvement Activities Issues Requirements Performance Improvement Activities Planned, minutes of meetings, mortality/morbidity review Incident Reporting System in place for every department/unit, trained in RCA, minutes of meetings, remedial measures (some standards made this as CORE criteria) Specific Performance Indicators According to your standard, please monitor 2/3 indicators stated in the criteria as this field is CORE in every standard (requirement from MSQH) -must have tracking & trending -minutes of meetings -audit and remedial measures
Quality Improvement
Quality Improvement Activities § Planned and systematic QI Efforts – Monitoring – data – Assessment – problem identification – Evaluation – effectiveness of actions – Feedback – communication of results § Appropriate documentation with confidentiality
QI Activities
QI Activities
Standards § Standards are mandatory actions or rules that give formal policies support and direction.
What are Key Performance Indicators? § A healthcare KPI is a well-defined performance measurement that is used to monitor, analyze and optimize all relevant healthcare processes to increase patient satisfaction § Different service departments will normally have different KPI’s
Special Requirements
Special Requirements § Specific for each standard § Mainly dealing with specialized services provided by the department/ unit § Radiotherapy; Medical Oncology; Transplant, etc § Usually have specific policies for the service provided, equipment use with PPM, training needs with regular assessment
Questions?
Exercise on OT Services § Does your hospital have a policy on OT services? § How is the chairman of OT services appointed § Are OT committee meetings planned or called on ad hoc basis? § Who are invited into OT committee meetings? § What do you discuss at OT committee meetings? § Is the OT committee chairman
SERVICE STANDARD 11 : OPERATING SUITE SERVICES PREAMBLE The Operating Suite Services have combined multidisciplinary healthcare personnel, e. g. surgeons, anaesthetists, nurses, theatre technician and other support staff in delivering a high standard of comprehensive patient care to those who require operative procedures during their stay in Healthcare Facility. The multidisciplinary teams working in the operating suite provide operative care, anaesthetic, theatre care and recovery. Each aspect works together to provide a coherent working
SERVICE STANDARD 11 : OPERATING SUITE SERVICES PREAMBLE The operating suite promotes a culture of safe and evidence based practice that is monitored to meet: a) expectations of patients; b) compliance with regulatory and statutory requirements; c) WHO Patient Safety Solutions - Safe Surgery Saves Lives