MSQH Accreditation Standards 5 th Edition Training Quality










")






































- Slides: 59
MSQH Accreditation Standards 5 th Edition Training Quality Standards 9 B, 10 and 11 Improving Efficiency, Safety and Performance 14 th November 2019 MSQH, Wisma Sejarah
MSQH Survey Item: Section 5 Developing a Culture for Safety
MSQH Survey Item: Section 5 The quality component of the MSQH survey looks at how well you have integrated and implemented the first four components of the accreditation processes into clinical practice
MSQH Survey Item: Section 5 The quality component of the MSQH survey looks at how well you have integrated and implemented the first four components of the accreditation exercise into clinical practice
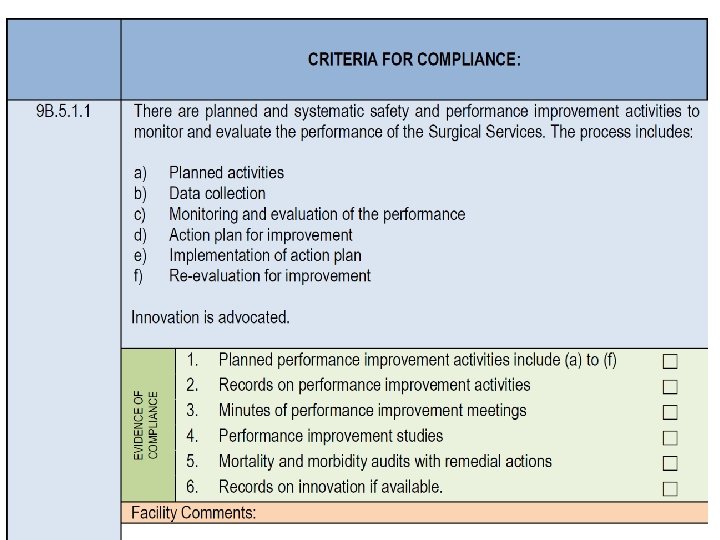
SERVICE STANDARD 9 B : CLINICAL SERVICES – SURGICAL RELATED SERVICES Topic 9 B: 5 Safety and Performance Improvement Activities The Head of Surgical Services shall ensure the provision of quality performance with staff involvement in the continuous safety and performance improvement activities of the Surgical Services. The Head of Surgical Services shall ensure compliance to monitoring of specific performance indicators.
Every Surgical Department has an officer for their QA programmes
Incident Reporting needs to be taken seriously
Steps in Root Cause Analysis 1. 2. 3. 4. 5. Charter the team Document and research Identify root causes Develop actions Establish outcome measures
Reporting & Learning System • Can detect latent errors • Provide multiple perspectives over time • Can be a standard procedure
You need a Quality Management Programme
You need to track and trend your Key Performance Indicators (KPI’s)
You need to look at your data and look for opportunities to improve your service
Confidentiality and Non-punitive Approach: to encourage reporting
That is all we ask from you!
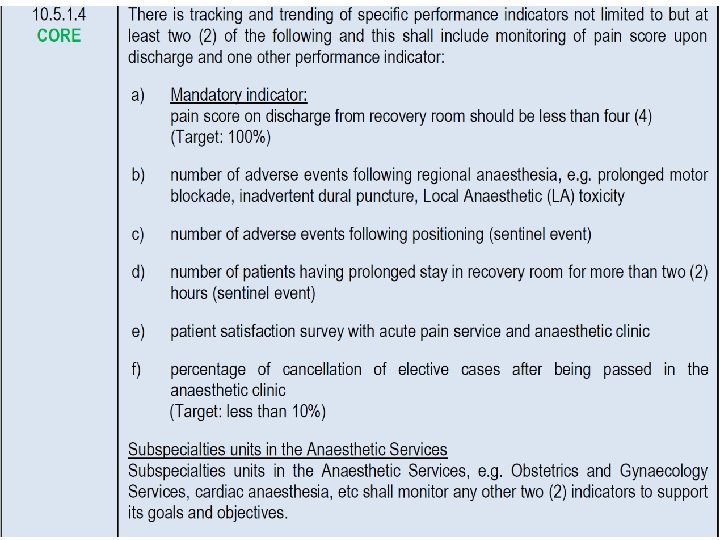
SERVICE STANDARD 10 : Anaesthesia Services
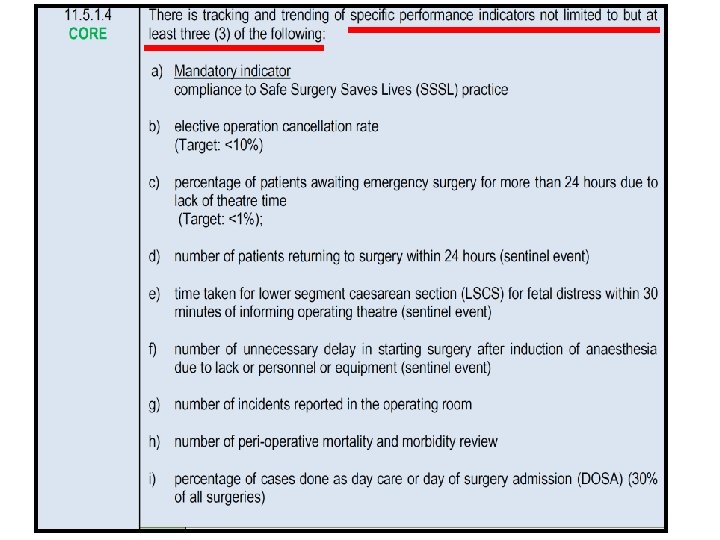
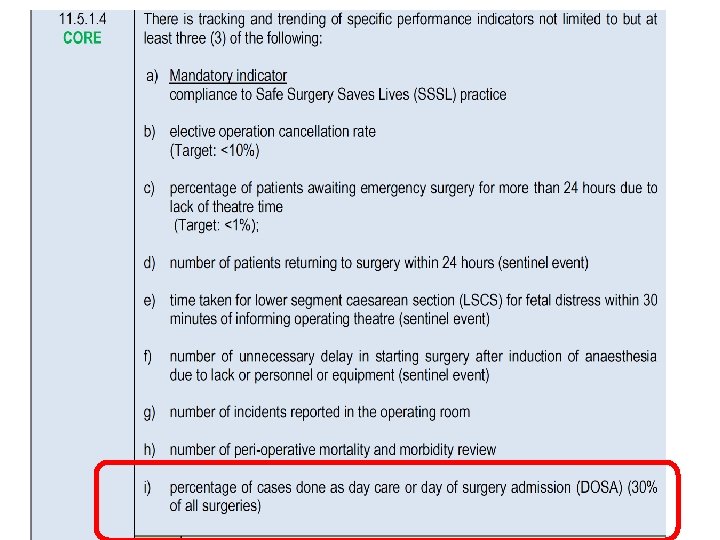
SERVICE STANDARD 11 : Operation Suite Services
The Head of OT Services is also responsible for OT’s QA programme
Day Care Surgery/Day of Admission Surgery. A cost saving and bed efficiency practice How many % of surgeries should we target for daycare surgery?
Endoscopy and other surgical procedures under sedation A quality Assurance Issue
The good old days
Endoscopy: A Diagnostic and Therapeutic Procedure
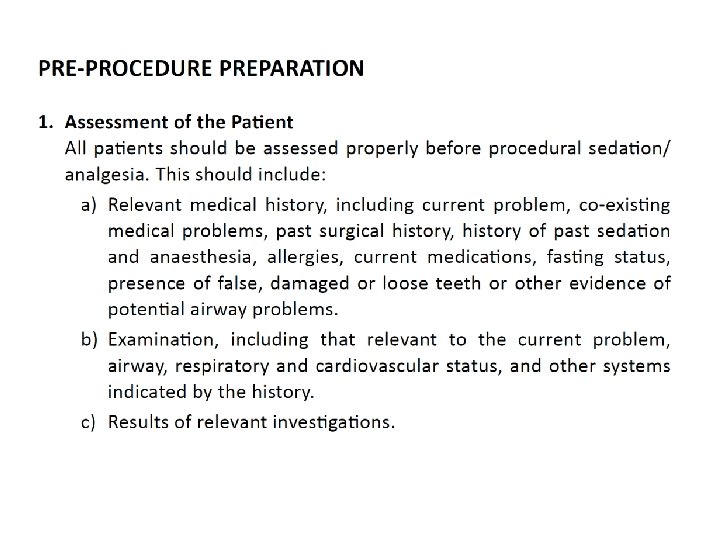
A good history is mandatory to patient safety
IV access and Sedation for procedure is usually required
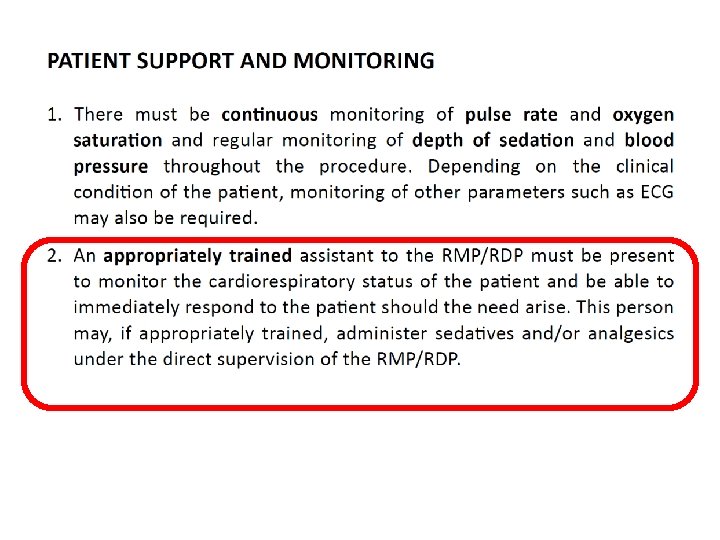
Monitoring during the procedure is required
Always guard the airway
Observation in recovery after the procedure
Ensure full recovery before discharge
Endoscopic procedures carried our under sedation carries a low but definite mortality risk
Endoscopic procedures carried our under sedation carries a low but definite mortality risk The incidence of cardiac arrest during and immediately after the procedure (recovery area) for all endoscopies was 3. 92 per 10, 000; of which, 72% were airway management related.
44 year old man dies during dental procedure
He was the son-in- law of our DPM
What went wrong?
Root Cause Analysis A root cause analysis is a process used to identify the primary source of a problem. In social and behavior change communication (SBCC), a root cause analysis is used to examine why there is a difference between the desired state of a health or social issue (vision) and what is happening now (current situation).
Root Cause Analysis § What happened § Why it happened § Ways to prevent it from happening again § How you will know you are safer
Root Cause Analysis § What happened § Why it happened § Ways to prevent it from happening again § How you will know you are safer
Root Cause Analysis Should look at failures in: § Governance and Management (Licensing and Regulations) § Qualifications, Credentialing and Privileging (i. e. Skills and Training) § Policies and Procedures (Protocols, Patient care standards, etc) § Facilities and Equipment (patient monitoring and resuscitation)
Root Cause Analysis Failures in: § Governance and Management The facility was only licensed to perform dental procedures under LA. (For sedation/GA, need a license for Day Care Medical Centre set-up) § Qualifications, Credentialing and Privileging (Locum doctor employed to give sedation)
Root Cause Analysis Failures in: § Policies and Procedures (Did not follow clinical practice guidelines for administering sedation) § Facilities and Equipment (Inadequate patient monitoring and resuscitation equipment)
Charged in court and found guilty
MSQH expects you to understand follow clinical practice guidelines issue by the Medical Academic Organizations of Malaysia
Minimal Monitoring Standards for Anaesthesia
They are both patient safety and medicolegal documents
Trial of clinic where DPM’s son-in-law died continues FMT June 8, 2017 7: 25 KUALA LUMPUR: A witness told the Sessions Court here yesterday that a medical practitioner had to be registered with the Malaysia Medical Academy (MMA) and have experience before he or she could be allowed to anaesthetise a patient. Head of the anaesthesia and intensive care department at Sungai Buloh Hospital, Dr Lim Wee Leong, 59, said besides having to be supervised by a specialist anaesthetist, the medical practitioner was also required to observe procedures and to have the necessary equipment.
Can a nurse give the IV sedation?
What kind of patient monitoring is required during the procedure?
What kind of patient monitoring is required during the procedure? i. e. Sp. O 2 Monitor, BP monitor, +/ECG, Sedation score
Personal Observation: Medical record keeping is often very poorly done
MSQH Survey Item: Section 5 The quality component of the MSQH survey looks at how well you have integrated and implemented the first four components of the accreditation processes into clinical practice