MRCP technique and interpretation 10 rules in MRCP

 NON-FATSAT TE 60 TE 360")


 • Thin-section MRCP • Scout for")








 MRCP")












 - limitations in spatial")
")












- Slides: 43
MRCP: technique and interpretation “ 10 rules in MRCP” Lieven Van Hoe MD Ph. D OLV Hospital Group Aalst - Belgium lievenvanhoe@hotmail. com www. lievenvanhoe. com
Procedure Axial and coronal double echo HASTE (5 mm) NON-FATSAT TE 60 TE 360
10% of your patients has focal liver lesions Double echo HASTE: lesion characterizarion SI SI TE 60 TE 300 -400 cyst ++ / +++ as bright as CSF hemangioma + / ++ not as bright as CSF solid ± / + ± isointense
solid 360 msec hemangioma
Axial and coronal double echo HASTE (5 mm) • Thin-section MRCP • Scout for breath-hold single-slice MRCP
Procedure Single-slice MRCP – – – RARE sequence slice thickness 3 cm, TE 1100 3 sec / image breath hold = overview images
Procedure Axial non-FATSAT turbo. FLASH T 1 = magic tool for detection of pancreatic cancer and focal liver lesions Liver white Pancreas white Tumor dark
Procedure Multiphase contrast-enhanced VIBE • Problem-solving tool • Pancreatic lesions • Only if required T P
Rule N° 1 Never use MRCP without crosssectional imaging
Man, 43 -year, elevated liver enzymes, previously papillotomy for biliary stone disease. Stone?
Aerobilia Always correlate with axial T 2 weighted images !! Air-fluid level Extensive air may make MRCP nondiagnostic
Liver function abnormalities
Missed pancreatic carcinoma Never perform MRCP without cross-sectional imaging never, never TFLASH: 700 msec/slice – HASTE: 400 msec / slice
Rule N° 2 Use dynamic (repetitive) MRCP
May 13, 2003 10 hr: 12 min: 15 sec May 13, 2003 10 hr: 12 min: 23 sec
Temporal variability in shape of the sphincter of Oddi It works ! Only possible with breath-hold singleslice MRCP
Rule N° 3 Use the correct slice thickness Not 10 cm !
10 cm 2 cm 5 cm 3 cm
Rule N° 5 Be aware of biliary flow phenomena on axial images
axial T 2 Flow void in common bile duct Compare with single-slice MRCP Believe single-slice MRCP if results are different
Rule N° 6 Be aware of the pseudo-calculus sign
Pseudocalculus sign 30 sec later
Rule N° 7 Small stones not surrounded by fluid are invisible
Does the patient has stones in distal CBD ? ? Not included in slice Normal size
Impacted stone May be difficult diagnosis ! No surrounding fluid Repetitive imaging useful
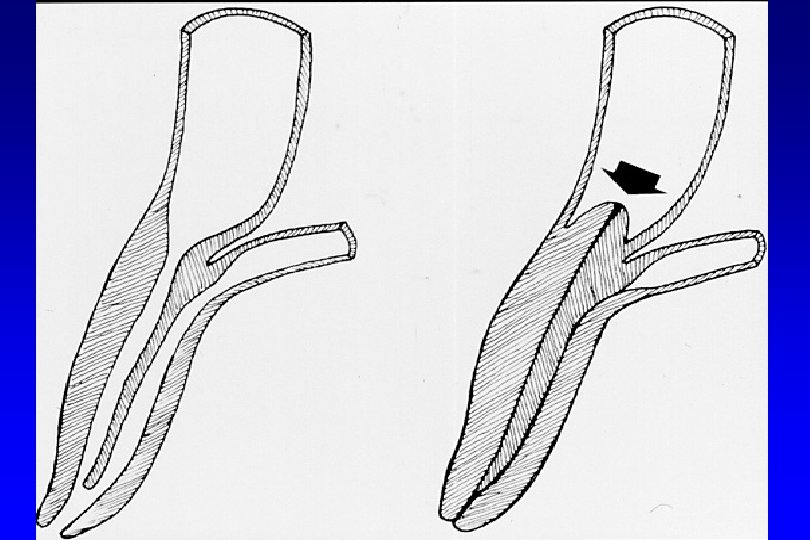
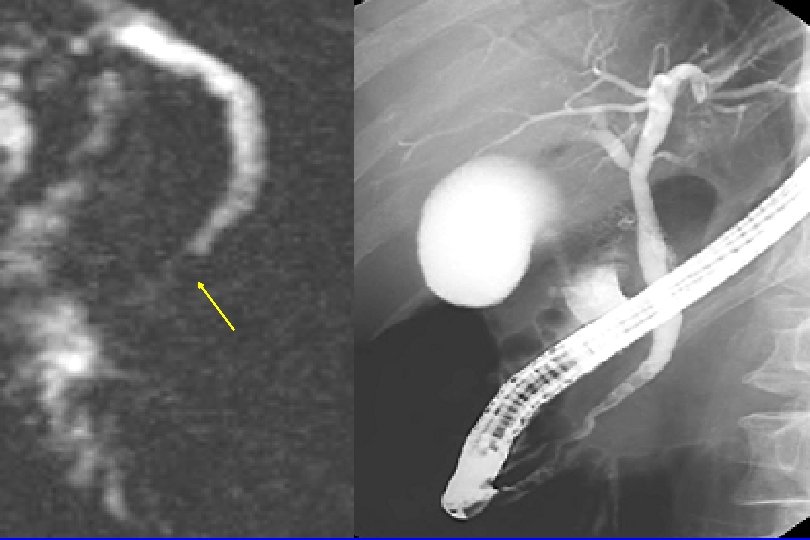
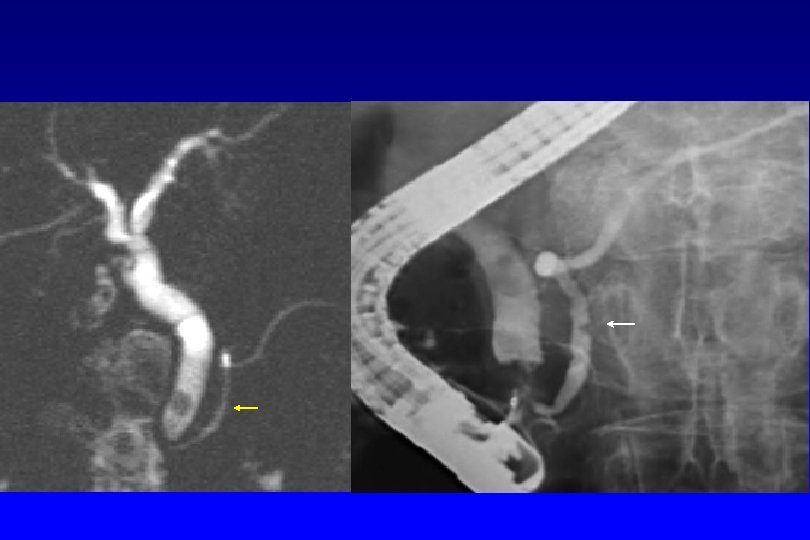
Rule N° 8 Anticipate differences between MRCP and ERCP images
MRCP: - imaging in the physiologic state (no ductal distention) - limitations in spatial resolution • Low-grade stenoses can be missed • The length of stenoses can be overestimated (physiologic collapse) • Small polypoid ductal lesions can be missed
MRCP – ERCP The same things look different !! (distention)
Aberrant right posterior duct
Rule N° 9 For lesion characterization, use all information available (T 1, T 2, MRCP, multiphase contrast-enhanced images)
Cirrhosis. Incidental finding.
The double duct sign can be caused by chronic pancreatitis with pseudomass. Refer to axial T 1 and T 2 -weighted images for differentiation with carcinoma.
Rule N° 10 Be aware of susceptibility artifact
Watanabe et al. Radio. Graphics 1999 19: 415 -429
Susceptibility artifact air metal
Thank you !!
The double duct sign can be caused by chronic pancreatitis with pseudomass. Refer to axial T 1 and T 2 -weighted images for differentiation with carcinoma.
Rule N° 4 Be careful with MIP images
The patient recently underwent laparoscopic gallbladder surgery and now suffers from jaundice. Injury to CBD?
MIP Projects 3 D reality on 2 D image Pathology may be masked