Motivational Interviewing Helping Patients Change Behavior Motivational Interviewing

Motivational Interviewing Helping Patients Change Behavior

Motivational Interviewing As a physician, why should I care?
, 2007.")
Schroeder, NEJM; 357(12), 2007.

Why do people develop negative habits?

Why do people develop negative habits?

Why do people develop negative habits? External factors: life stresses Internal factors: depression, boredom So what do they do to feel better?

Why do people develop negative habits? External factors: life stresses Internal factors: depression, boredom So what do they do to feel better? Coping strategies: adaptive and maladaptive

Dr. David Waters: Every problem was once a solution.

Lessons We Have Learned Information alone often doesn’t work! Why is that?

Dr. David Waters: When you meet resistance that does not make sense, think deficit. When you see won’t, think can’t.

Contrary to our instincts…. u u Attempts to persuade create resistance Attempts to persuade just increase the stress! Why is that?

Tough Love Approach

Motivational Interviewing What is it?

The “Spirit” of Motivational Interviewing u Collaboration

The “Spirit” of Motivational Interviewing u Collaboration vs. Confrontation

The “Spirit” of Motivational Interviewing u Collaboration u Evocation vs. Confrontation

The “Spirit” of Motivational Interviewing u Collaboration vs. Confrontation u Evocation vs. Imposition

The “Spirit” of Motivational Interviewing u Collaboration vs. Confrontation u Evocation vs. Imposition u Autonomy

The “Spirit” of Motivational Interviewing u Collaboration vs. Confrontation u Evocation vs. Imposition u Autonomy vs. Authority

Stages of Change
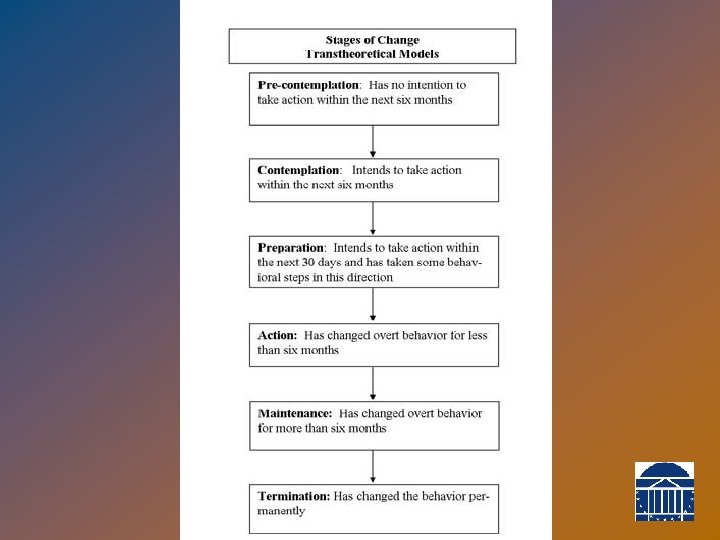

Physician’s role in behavior change • Goal = Help patient move ahead to the next stage u u u • First, understand the patient. Accurately assess patient’s current stage. Then, facilitate movement towards the next stage. Adult learning happens best when: • Self-initiated and Self-directed • Practical, useful, applicable to real life • Incorporates feedback about efforts • To promote behavior change, physician should be: • partner, not expert; • coach, not parent; • mirror, not magic bullet.
: This is either a denial of the problem, or an awareness")
Pre-Contemplation (resisting change): This is either a denial of the problem, or an awareness of the problem with an unwillingness to change. Strategies:
: This is either a denial of the problem, or an awareness")
Pre-Contemplation (resisting change): This is either a denial of the problem, or an awareness of the problem with an unwillingness to change. Strategies: • Seek permission just to talk about it for a minute. • Open ended questions; thoughts and feelings. • Empathetically reflect the ambivalence. • Resist the righting reflex. • Reinforce the willingness to even talk about it. • Rate importance. Understand patient priorities. • Elicit patient goals. Link behavior to goals. • Role with resistance. • Seek permission to offer information.
: There is an awareness of a problem, an understanding")
Contemplation (change on the horizon): There is an awareness of a problem, an understanding of the pros and cons of change, yet there is a fear of change. Strategies: •
: There is an awareness of a problem, an understanding")
Contemplation (change on the horizon): There is an awareness of a problem, an understanding of the pros and cons of change, yet there is a fear of change. Strategies: • Elicit Change-Talk. • Pros and Cons • Develop Discrepancy (values vs current behavior) • Role with resistance. Avoid Argument. Rating importance and confidence. • Explore aspects of confidence and importance • Understand barriers.

Confidence Ruler Not important to make a change No confidence in ability to change Very important to make a change Very confident in ability to change
: There is a clear awareness of the problem and the need")
Preparation (getting ready): There is a clear awareness of the problem and the need to learn how to change. Strategies:
: There is a clear awareness of the problem and the need")
Preparation (getting ready): There is a clear awareness of the problem and the need to learn how to change. Strategies: • Have patient reiterate motivation for change • Look over fence. • Discuss previous attempts (learn from experience) • Plan specific strategies (actions); • SMART goals—very small • Explore concerns and barriers • Problem solve barriers • Enlist supports • Set a date

SMART goals • Specific • Meaningful • Assessable • Realistic • Timed
: The person starts to terminate unhealthy behaviors and develop new,")
Action (time to move): The person starts to terminate unhealthy behaviors and develop new, more positive behaviors. Strategies: • .
: The person starts to terminate unhealthy behaviors and develop new,")
Action (time to move): The person starts to terminate unhealthy behaviors and develop new, more positive behaviors. Strategies: • Review pros and cons. • Reassess how SMART the goals are; adjust • Assess barriers; problem solve. • Assess adequacy of supports. • Resist cheerleading; take other side of the ambivalence.
: action behaviors are practiced and continually reinforced until they become automatic")
Maintenance (staying there): action behaviors are practiced and continually reinforced until they become automatic and last for an extended period of time. Strategies: • .
: action behaviors are practiced and continually reinforced until they become automatic")
Maintenance (staying there): action behaviors are practiced and continually reinforced until they become automatic and last for an extended period of time. Strategies: • Review pros and cons. • Assessing difficulty of maintaining • Predict and plan for tough spots. • Predict and plan for relapse. • Be proud and encouraging, but • Resist cheerleading.

The Effective Physician

Questions?

The End On a scale of 0 to 10, how important is it to you to be skilled in M. I. ? On a scale of 0 to 10, how confident are you in your M. I. skills?

Skills Practice Paying attention to our own mental, spiritual, and physical health. • Resilience. • More likely to engage patients. • Increases empathy.


Behavior change = Adult learning • How do adults learn best?

What is readiness? High Importance Low High Confidence

Rate it! • On a scale of 1 to 10, how important is it for you to…. . • On a scale of 1 to 10, how confident are you that you could …… • That’s interesting - why are you a 6 and not a 2? • What would have to change that would make you an 8 instead of a 5?

Link Behavior with Outcome; Establish the Patient’s Agenda • The patient’s agenda! u Ask directly about patient’s goals. u Link patient’s desired health outcome to a specific patient behavior: “You have [condition] …. . . And that is causing your [symptom or problem]. I think it might help to consider [behavior change]. . . ……” u Establish patient’s agenda: “What do you think? ” Avoid assigning physician’s agenda.

Linking Behaviors

Double DARES • • • Develop Discrepancy Avoid Argument Roll with Resistance Express Empathy Support Self-efficacy
 Have patient describe the discrepancy between their current behavior and")
Develop Discrepancy; (Establish Ambivalence) Have patient describe the discrepancy between their current behavior and what they have told you is important to them: ambivalence. u Have them present the reasons for change in terms of their desired outcome

Establish Ambivalence; Pros and Cons Examine pros and cons - help patient identify problem area or area of concern • Good things less good things about current behavior • Re-state their reasoning for and against change Other strategies • • • Scaling Explore concerns Hypothetical look over fence

Avoid Arguing • Be aware of threat of loss of freedom • “It should never be you against the patient; it should be the part of the patient that wants to change against the part that doesn’t…. ”

Roll with Resistance • Arises whenever there is tension or disagreement • Results from traps: u u u Taking control away Misjudging importance, confidence or readiness Meeting force with force

Roll with Resistance • Manifests in: u u u u ignoring, inattention, discounting, excusing, blaming, hostility, splitting, etc. • It is a sign that rapport needs attention.

Roll with Resistance • Resistance is your cue to change strategies. u Strategies: Emphasize personal choice and control Reassess stage and/or readiness (importance, confidence) • Back off and come alongside the patient • Stay committed but curious. • “It’s like dancing - you have to stay relaxed. ”

Decision Balance If the physician takes one side, the patient will take the other. Which side do you want to take?

Express Empathy u Express empathy without accepting the status quo. “I can understand that you might feel that way. ” u “Yes, it sounds pretty difficult, doesn’t it? ” u

Support Self-efficacy Confidence in ability to make specific change in behavior Ñ Ñ Ñ Goals Strategy Target Scaling Brainstorm solutions Past efforts: successes and failures Reassess confidence Ñ Avoid - “Yes, but”

Skills Practice Doctor- Patient Scenarios

Evoking Commitment to Change
- Slides: 57