MORNING REPORT Jennifer Katada R 1 Synovial Fluid


 • Trauma • Osteochondritis dissecans (osteonecrosis) • Neuropathic arthropathy")
 • Reactive arthritis")






 infection")


- Slides: 15
MORNING REPORT Jennifer Katada R 1
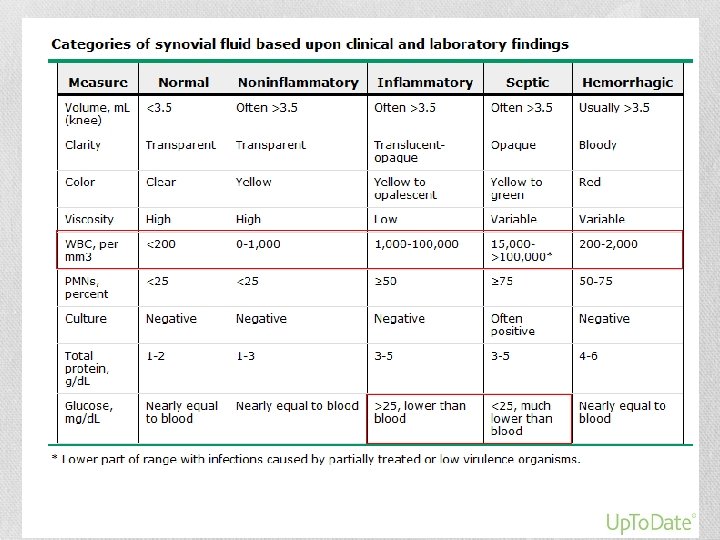
Synovial Fluid Analysis- Indications • American College of Rheumatology clinical guidelines • Febrile patient with acute flare of arthritis • Unexplained joint, bursa, or tendon sheath swelling • Suspected crystal-induced arthritis
Noninflammatory effusions • DJD (OA) • Trauma • Osteochondritis dissecans (osteonecrosis) • Neuropathic arthropathy • Early or subsiding inflammation • Hypertrophic osteoarthropathy • Also- Rheumatic fever, SLE, chronic sarcoidosis, and scleroderma
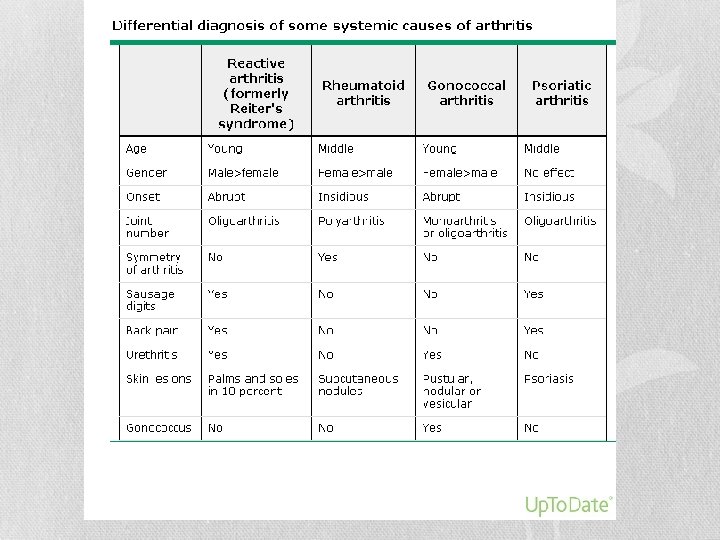
Inflammatory effusion • RA • Acute crystal-induced synovitis (gout, & pseudogout) • Reactive arthritis (Reiter syndrome) • Ankylosing spondylitis • Psoriatic arthritis • Arthritis associated with inflammatory bowel disease • Rheumatic fever • Systemic lupus erythematosus • Sarcoidosis • Hypertrophic osteoarthropathy • Systemic sclerosis
Septic effusion • Due to bacteria, mycobacteria, or fungus • Gram staining • Nongonococcal bacterial arthritis- sensitivity of gram stain is 50 -70% • Gonococcal arthritis- sensitivity is <10% • For clinical suspicion of infection- a culture should be performed for staphylococci, streptococci, and gram negative rods • If suspicion for Gonococcal infection- must be plated with Thayer-Martin media
Hemorrhagic effusion • Hemophilia • Anticoagulation or other hemorrhagic diathesis • Scurvy • Trauma (with or without trauma) • Neuropathic arthropathy • Tumor
When to send for unusual organism? • Hx TB exposure • Hx of trauma or animal bite • Travel or living in endemic area with fungal infection or lyme • Immunosuppression • Monoarthritis that is refractory to conventional therapy
Viruses that cause arthritis • Hepatits A- rash and arthralgia 10 -14%; arthritis rare (but typically in patient with vasculitis, and high cryoglobulin level) • Hepatitis B- acute infection or prodromal stage. M>W; symmetric, migratory, or additive and arthritis • Hepatitis C- immune complex mediated leading to deposition in joint and arthritis • Parvovirus- similar to SLE and arthritis occurs in 60% of adults with parvovirus infection, typically symmetric polyarthralgias • Rubella and rubella vaccine virus- grow in synovial fluid->arthritis; ~2 weeks after immunization. Similar to Rheumatic feversymmetric, migratory, and additive with resolution of symptoms in 2 weeks affecting small joints. • Mumps- uncommon, migratory polyarhtralgia
Viruses that cause arthritis • Alphaviruses- mosquito-borne. Africa and Asia. One example. Chikungunya. Triad- fever, arthritis, and rash. Dx via ELISA testing. • Dengue- acute febrile illness, headache, muscle and joint pain. • Enterovirus- coxsackie and echovirus; arthritis is uncommon • Adenovirus- nonspecific viral symptoms with arthritis • Herpes virus- including varicella, EBV, and simplex • CMV- polyarthritis • HIV infection- acute infection and increased risk for other causes
Treatment for inflammatory arthritis • Generally supportive and treatment with NSAIDS or aspirin • If directed treatment to etiology available- treat underlying cause
Rheumatic Fever- Jones Criteria • ARF is characterized by group A streptococcal (GAS) infection followed by clinical manifestations outlined below • The five major manifestations are: • • • Migratory arthritis (predominantly involving the large joints) Carditis and valvulitis (eg, pancarditis) Central nervous system involvement (eg, Sydenham chorea) Erythema marginatum Subcutaneous nodules • The four minor manifestations are: • Arthralgia • Fever • Elevated acute phase reactants (erythrocyte sedimentation rate [ESR], C-reactive protein [CRP]) • Prolonged PR interval • Need 2 Major or 1 major with 2 minor criteria AND evidence of GAS infection
References • Uptodate- article on synovial fluid analysis • Guidelines for the initial evaluation of the adult patient with acute musculoskeletal symptoms. American College of Rheumatology Ad Hoc Committee on Clinical Guidelines. Arthritis Rheum 1996; 39: 1 • Uptodate- article on disseminated gonoccocal infection • Uptodate- article on specific viruses that cause arthritis • Uptodate- article on clinical manifestations and diagnosis of acute rheumatic fever • Guidelines for the diagnosis of rheumatic fever. Jones Criteria, 1992 update. Special Writing Group of the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young of the American Heart Association. JAMA 1992; 268: 2069 • Jones TD. The diagnosis of rheumatic fever. JAMA 1944; 126: 481
Thank you