Morbimortalidade neonatal em prematuros extremos pequenos para a

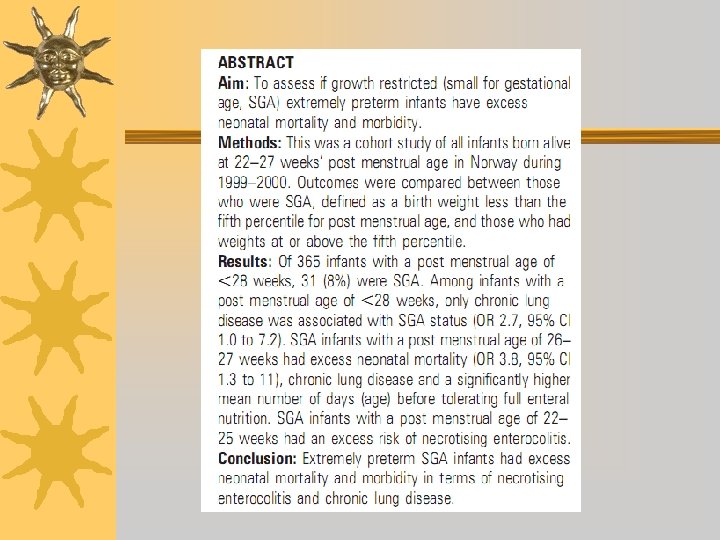
Morbimortalidade neonatal em prematuros extremos pequenos para a idade gestacional: um estudo de base populacional Neonatal mortality and morbidity in extremely preterm small for gestational age infants: a population based study S H Westby Wold, K Sommerfelt, H Reigstad, A Rønnestad, S Medbø, T Farstad, P I Kaaresen, R Støen, K T Leversen, L M Irgens, T Markestad. (Noruega) Arch. Dis. Child. Fetal Neonatal Ed. 2009; 94; F 363 -F 367 Internos: Carolina de Melo, Diego César Vieira e Francine Deola Pimentel Orientador: Dr. Paulo R. Margotto 22/9/2009

Ddos Francine, Carolina e Diego

Introdução ¬A influencia da redução do crescimento intra-uterino não tem sido estudada extensivamente no recém-nascido prematuro extremo ¬Há evidências que a redução do crescimento esteja associada com uma menor mortalidade

Objetivo ¬ Avaliar se a redução do crescimento aumenta a morbimortalidade em recémnascidos prematuros extremos.

Métodos ¬ Estudo de coorte ¬ RN entre 22 -27 semanas ¬ Peso 500 -999 g ¬ Avaliados entre 1 de janeiro do 1999 e 31 de dezembro de 2000 ¬ Idade gestacional avaliada por ultrassonografia (17 -18 sem. ) ou data da última menstruação ¬ Foram considerados pequenos para a idade gestacional os RN abaixo do percentil 5 ¬ Padrão usado: Noruega

Métodos ¬Foram comparados RN com percentil >=5 X percentil <5 ¬O percentil 5 foi escolhido par focar a restrição do crescimento por causas maternas (placentária) e não genéticas.

Análise estatística ¬ Foram comparados os RN PIG X AIG utilizando o X 2 e o teste de Fisher para variáveis categóricas e t-students para variáveis continuas. ¬Os RN foram estratificados em dois grupos: <25 sem. e 26 -27 sem. de idade gestacional ¬Usado regressão logística para ajuste do efeito de confundimento ¬Aprovado pelo comitê de ética ¬Utilizado consentimento informado.

Resultados ¬ 119. 611 nascimentos ¬ 638 com idade gestacional < 28 s ou peso < que 1000 g ¬ 174 (27%) natimortos ou RNs mortos na sala de parto ¬ 3 RNs foram excluídos devido a malformações letais ¬ 2 pais não aceitaram participar
 RNs permaneceram no estudo ¬ 94 tinham > 28 s")
Resultados ¬ 459 (99%) RNs permaneceram no estudo ¬ 94 tinham > 28 s e < 1000 g ¬ 55 (59%) eram PIG com média de idade de 29 s ¬ 39 (41%) eram AIG com média de idade de 28 s ¬ 365 tinham < 28 s e foram incluídos na análise principal ¬ 31 (8%) eram PIG
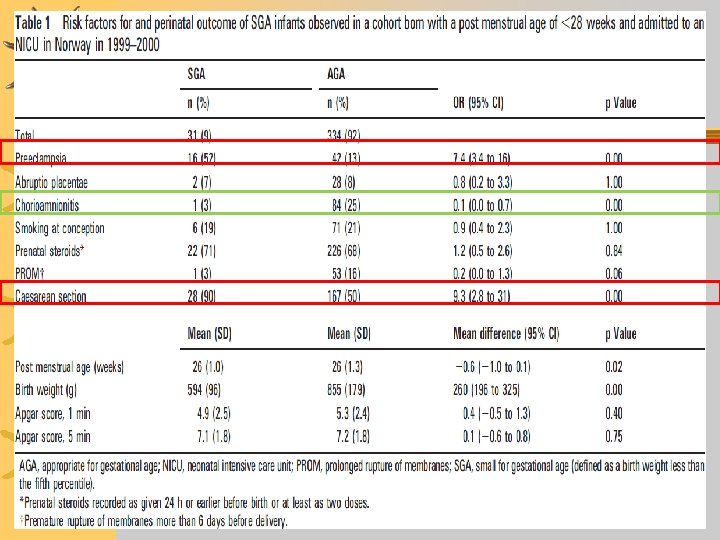

Resultados Observamos nesta tabela ¬-a pré-eclampsia, assim como a cesariana, ocorreram significativamente mais nos RN PIG (em inglês: SGA) ¬-a corioamnionite ocorreu significativamente mais nos RN AIG

CLD, chronic lung disease; NEC, necrotising entercolitis; NICU, neonatal intensive care unit; PDA, persistent ductus arteriosus; PVL, periventricular leucomalacia; ROP, retinopathy of prematurity; SCH, severe cerebral haemorrhage; SGA, small for gestational age. *Excluded those who died before 28 days after birth in the PVL analyses, and excluded those who died before 36 weeks after birth in the ROP and CLD analyses. {More than or two cysts limited to one side. Only included infants surviving at least 28 days. {Infants only included if surviving until at least 36 weeks’ post menstrual age. 1 Need for oxygen supplementation or assisted ventilation at 36 weeks’ post menstrual age.
 ocorreu significativamente mais")
Resultados ¬Observamos nesta tabela ¬- A displasia broncopulmonar (em inglês: CLD) ocorreu significativamente mais nos RN PIG (significância bordeline: observe o limite inferior do intervalo de confiância: 1, 02 -7, 2)
 morreram ¬")
Resultados ¬ Dos 365 RN com < 28 s: 1. 75 (21%) morreram ¬ 10 PIG ¬ Causas: cerebrais (04), respiratórias (05), complicação aguda (03), sepse (01) e ECN (01) ¬ 65 AIG ¬ Causas: cerebrais (20), respiratórias (29), complicação aguda (07), sepse (12) e ECN (05)
 e após análise multivariada,")
Resultados ¬ Incluindo os RNs com > 28 s (94) e após análise multivariada, controlando o efeito da idade gestacional, PIG x AIG: ¬ Mortalidade (OR 3. 9, 95%, CI 1. 8 to 8. 4; p=0. 00) ¬ Risco de ECN (OR 2. 9, 95% CI 1. 1 to 7. 7; p=0. 03) ¬ Risco de DBP (OR 3. 3, 95% CI 1. 7 to 6. 5; p=0. 00) ¬ Risco de Sepse (OR 1. 9, 95% CI 1. 0 to 3. 6; p=0. 04) ¬ Número de dias antes de tolerar nutrição enteral total (B 9. 1, 95% CI 0. 05 to 18; p=0. 04)
, SEM controle do efeito")
Resultados ¬ Incluindo os RNs com > 28 s (94), SEM controle do efeito da idade gestacional, PIG x AIG: ¬Mortalidade (OR 0. 9, 95% CI 0. 5 to 1. 7; p=1. 00) ¬ECN (OR 0. 6, 95% CI 0. 1 to 2. 7; p=0. 75) ¬DBP (OR 1. 0, 95% CI 0. 6 to 1. 6; p=1. 00) ¬PDA (OR 0. 4, 95% CI 0. 2 to 0. 7; p=0. 00)

Discussão ¬ PIG e < 28 semanas apresentam maior mortalidade neonatal e maior risco para displasia broncopulmonar e enterocolite necrotizante. ¬ Pré-eclâmpsia e cesariana estão associados com PIG. Provavelmente o maior índice de préeclâmpsia e o RCIU levaria ao maior número de cesarianas (conduta mais ativa). ¬ Ruptura prolongada de membranas corioamnionite estão mais associados a AIG. e

Discussão ¬ O excesso de mortalidade em PIG está de acordo com estudos anteriores. ¬ No estudo de Regev RH demonstrou uma mortalidade duas vezes maior em PIG < 32 sem – – 24– 25 sem - OR: 2. 3 (95% CI 1. 1 to 4. 7) 26 -27 sem - OR: 3. 4 (2. 1 to 5. 3) 28 -29 sem - OR: 3. 9 (2. 5 to 6. 0) 30 -31 sem - OR: 1. 7 (0. 8 to 3. 7) ¬ A mortalidade em PIG em < 28 semanas é semelhante ao encontrado neste estudo.

Discussão ¬ PIG não está associado com hemorragia cerebral severa e leucomalácia periventricular, o que está de acordo com a maioria dos estudos. ¬Enterocolite necrotizante é mais frequente em PIG com pré-eclâmpsia. Porém, neste estudo não houve diferença significativa de EC em PIG com ou sem pré-eclâmpsia.

Discussão ¬ PIG está mais associado a displasia broncopulmonar. Neste estudo o resultado encontrado está no limite do intervalo de confiança. ¬Não houve maior risco de sepse em PIG neste estudo.

Conclusão Pré-termo extremo e PIG apresentam excesso de mortalidade e morbidade em termos de enterocolite necrotizante e displasia broncopulmonar.

QUAL É A MENSAGEM? A restrição do crescimento intra-uterino nos recém-nascidos extremamente prematuros associa-se com maior mortalidade (26 -27 semanas) e maior risco de enterocolite necrosante (22 -25 semanas), além de maior tempo requerido para atingir a nutrição enteral plena (26 -27 semanas) Importância -aconselhamento dos pais -planejamento da intervenção: melhor tempo para o nascimento dos RN PIG pré-termos extremos

Referências 1. Ancel PY, Marret S, Larroque B, et al, The Epipage Study Group. Are maternal hypertension and small-for-gestational age risk factors for severe intraventricular hemorrhage and cystic periventricular leukomalacia? Results of the EPIPAGE cohort study. Am J Obstet Gynecol 2005; 193: 178– 84. 2. Bartels DB, Kreienbrock L, Dammann O, et al. Population based study on the outcome of small for gestational age newborns. Arch Dis Child Fetal Neonatal Ed 2005; 90: 53– 9. 3. Korhonen P, Tammela O, Koivisto AM, et al. Frequency and risk factors in bronchopulmonary dysplasia in a cohort of very low birth weight infants. Early Hum Dev 1999; 54: 245– 58. 4. Bernstein IM, Horbar JD, Badger GJ, et al. Morbidity and mortality among very lowbirth- weight neonates with intrauterine growth restriction. The Vermont Oxford Network. Am J Obstet Gynecol 2000; 182: 198– 206. 5. Regev RH, Lusky A, Dolfin T, et al. Excess mortality and morbidity among small forgestational- age preterm infants: a population-based study. J Pediatr 2003; 143: 186– 91. 6. Baschat AA. Doppler application in the delivery timing of the preterm growthrestricted fetus: another step in the right direction. Ultrasound Obstet Gynecol 2004; 23: 111– 18.

Referências 7. The GRIT Study Group. A randomised trial of timed delivery for the compromised preterm fetus: short term outcomes and Bayesian interpretation. BJOG 2003; 110: 27– 32. 8. Markestad T, Kaaresen PI, Rønnestad A, et al. Early morbidity, and need of reatment among extremely premature infants. Pediatrics 2005; 115: 1289– 98. 9. Irgens LM. The Medical Birth Registry of Norway: epidemiological research and surveillance throughout 30 years. Acta Obstet Gynecol Scand 2000; 79: 435– 9. 10. Skjaerven R, Gjessing HK, Bakketeig LS. Birthweight by gestational age in Norway. Acta Obstet Gynecol Scand 2000; 79: 440– 9. 11. Papile LA, Burstein J, Burstein AR, et al. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1500 gm. J Pediatr 1978; 92: 529– 34. 12. Committee for the Classification of Retinopathy of Prematurity. Na international classification of retinopathy of prematurity. Arch Ophthalmol 1984; 102: 1130– 4.

Referências 13. Rønnestad A, Abrahamsen TG, Medbø S, et al. Septicemia in the first week of life in a Norwegian national cohort of extremely premature infants. Pediatrics 2005; 115: 262– 8. 14. Beeby PJ. Risk of death for small for gestational age very preterm infants (letter). Pediatrics 1998; 105: 1497– 8. 15. Veelken N, Stollhoff K, Claussen M. Development and perinatal risk factors of very low-birth-weight infants. Small versus appropriate for gestational age. Neuropediatrics 1992; 23: 102– 7. 16. Sharma P, Mc. Kay K, Rosenkrantz TS, et al. Comparisons of mortality and predischarge respiratory outcomes in small-for-gestational-age and appropriate-forgestational- age premature infants. BMC Pediatr 2004; 4: 9. 17. Zaw W, Gagnon R, da Silva O. The risks of adverse neonatal outcome among preterm small for gestational age infants according to neonatal versus fetal growth standards. Pediatrics 2003; 111: 1273– 7. 18. Leviton A, Paneth N. White matter damage in preterm newborns—an epidemiologic perspective. Early Hum Dev 1990; 24: 1– 22. 19. Garite TJ, Reese C, Thorp JA. Intrauterine growth restriction increases morbidity and mortality among premature neonates. Am J Obstet Gynecol 2004; 191: 481– 7.

Referências 20. Simchen MJ, Beiner ME, Strauss-Liviathan N, et al. Neonatal outcome in growthrestricted versus appropriately grown preterm infants. Am J Perinatol 2000; 17: 187– 92. 21. Bahado-Singh RO, Kovanci E, Jeffres A, et al. The Doppler cerebroplacental ratio and perinatal outcome in intrauterine growth restriction. Am J Obstet Gynecol 1999; 180: 750– 6. 22. Hartung J, Kalache KD, Hevna C, et al. Outcome of 60 neonates who had ARED flow prenatally compared with a matched control group of appropriate-for-gestational age preterm neonates. Ultrasound Obstet Gynecol 2005; 25: 566– 72. 23. Kirsten GF, van Zyl N, Smith M, et al. Necrotizing enterocolitis in infants born to women with severe early preeclampsia and absent end-diastolic umbilical artery doppler flow velocity waveforms. Am J Perinatol 1999; 16: 309– 14. 24. Bardin C, Zelkowitz P, Papageorgiou A. Outcome of small-for-gestational age and appropriate-for-gestational age infants born before 27 weeks of gestation. Pediatrics 1997; 100: 4. 25. Lal MK, Bradley NM, Draper ES, et al. Chronic lung disease of prematurity and intrauterine growth retardation. A population-based study. Pediatrics 2003; 111: 483– 7. 26. Thompson PJ, Greenough A, Gamsu HR, et al. Ventilatory requirements for respiratory distress syndrome in small-for-gestational-age infants. Eur J Pediatr 1992; 151: 528– 31.

Obrigado!! Ddos Francine, Carolina e Diego e Dr. Paulo R. Margotto
- Slides: 28