Morbidity and Mortality Conference 4242018 Presentation in ED

Morbidity and Mortality Conference 4/24/2018

Presentation in ED: 4/11/2018 HPI Patient ES is a 51 year-old male with history of alcohol abuse, GERD, diabetes, hypertension, hyperlipidemia, recent intracranial and subarachnoid hemorrhage (secondary to fall while intoxicated, discharged 4/3/2018 from Kenmore Mercy) who presents in the ED vomiting bright red blood for the past 3 -4 hours. Since being discharged from Kenmore Mercy he has had a significant stable headache, and he has been drinking large amounts of alcohol to try to alleviate the pain. He has intermittently been experiencing lightheadedness, dizziness, and a “flashing lights” visual disturbance. He experienced shortness of breath and abdominal pain before he started vomiting.

Surgical: none Social: Current smoker, 30 pack-year history; daily alcohol use from waking until sleep; former cocaine use Histories Medications: atorvastatin 80 mg QHS, gabapentin 800 mg TID, lactulose 30 m. L BID, lisinopril 20 mg daily, pantoprazole 40 mg daily, Januvia (sitagliptin) 100 mg daily, thiamine 100 mg daily Allergies: none Recent admission to Kenmore Mercy on 4/3/2018: intracranial hemorrhage and subarachnoid hemorrhage secondary to fall while intoxicated. Managed without neurosurgical intervention. Full code

General: A sedated, middle-age male, mechanically ventilated. Neuro: Withdraws to pain, does not respond to voice. Physical Exam Cardiac: S 1/S 2/S 3 heard, grade II/VI systolic murmur. No peripheral edema. Respiratory: Mechanically ventilated. Lungs clear to auscultation bilaterally, good air entry throughout Abdomen: Soft, non-tender, markedly distended. Skin: Marked jaundice throughout.

ED Course In the ED, the patient vomited approximately 1 liter of blood, with clots the size of golf balls. Systolic pressure dropped to the 80 s, and he received 2 x 1 L saline boluses, an octreotide bolus, and was started on an octreotide drip. He was given a total of 8 mg IV Zofran. 4 U of blood were ordered. GI was contacted for emergent endoscopy. Anesthesia was called to intubate for airway protection. STAT CT head/abdomen/pelvis was ordered. Admitted to ICU

Initial Labs 4/11/2018 6. 9 10. 3 30. 6 108 142 110 23 ***** 21. 0 0. 88 INR: 1. 5, Albumin 3. 2, Bilirubin 3. 1, ALP 236, ALT 35 155

EGD was done by GI EGD revealed multiple bleeding esophageal varices. Banding was completed, but not all bleeding could be stopped. IR was called for TIPS evaluation Procedures At this point 2 U PRBC had been transfused, with 3 more units ordered and pending post-transfusion CBC Patient was hypotensive during procedures and was placed on Levophed Into the morning of the next day: TIPS was attempted unsuccessfully. As a temporizing measure the varices were coil embolized

AM Labs 4/12/2018 9. 0 8. 2 24. 1 60 146 114 31 4. 9 22. 0 0. 90 Albumin 2. 6, Bilirubin 3. 9, ALP 163, AST 85, ALT 41 163

At this time patient remained mechanically ventilated Octreotide and PPI ordered Q 4 hr H&H ICU Course 4/13/2018 Morning of 4/13, patient developed severe anemia and hyperkalemia (Hb 6. 2, K 7. 2) Kayexalate 60 g PR 2 g IV calcium gluconate 1 amp HCO 3 D 50 + 10 U insulin Transfused 4 U PRBC that morning 500 cc NS bolus BP still dropped to 65/45, Levophed titrated to max and Neosynephrine added TIPS re-attempted that day, successfully
 By")
Patient developed metabolic acidosis secondary to lactic academia ICU Course 4/13/2018 (continued) By later in the day he required 3 pressors Troponinemia with peak of 0. 75, not a candidate for any interventions Developed oliguric renal insufficiency likely secondary to contrast nephropathy. Nephrology consulted.

Hemoglobin history during hospital course: 12 10 8 4 2 TIPS 6 coiling ICU Course 4/14/2018 0 Early morning of 4/14/2018, patient went into cardiorespiratory arrest, and death was pronounced at 5: 55 AM

Conclusion Questions/discussion

Alcoholic Liver Disease

Definition of Cirrhosis Chronic liver disease characterized by fibrosis, disruption of the liver architecture and widespread nodules in the liver. Fibrous tissue replaces damaged or dead hepatocytes, distorting the anatomy Decreased blood flow through the liver with subsequent hypertension in portal circulation (ascites, edema, splenomegaly, varicosities) Hepatocellular failure that leads to impairment of biochemical function (decreased albumin synthesis, decreased clotting factor synthesis, decreased metabolism of estrogen)
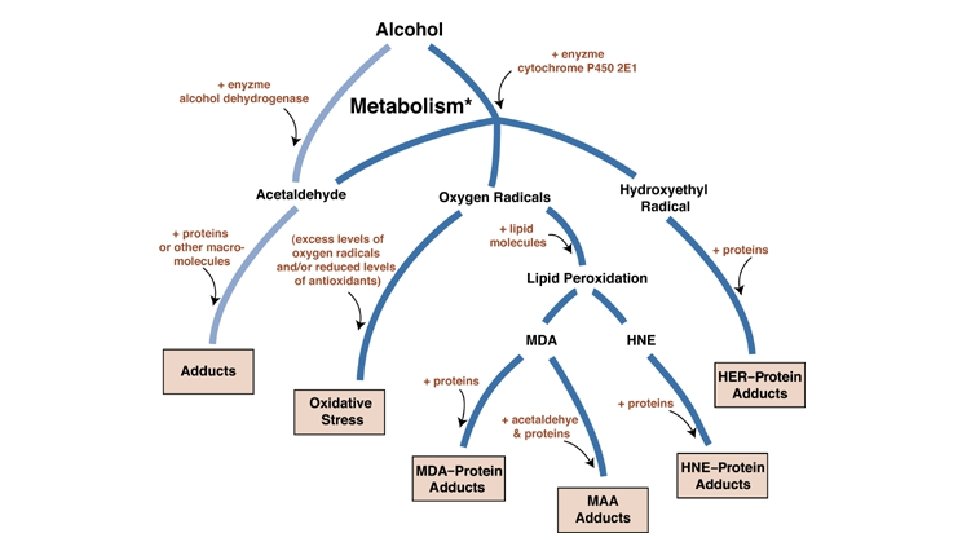
 Steatosis: accumulation of")
Cirrhosis is often preceded by hepatitis and steatosis (reversible damage) Steatosis: accumulation of fatty acid in liver cells due to increased NADH/NAD+ ratio from alcohol metabolism Alcohol Metabolism NADH induces fatty acid synthesis Decreased NAD+ decreased fatty acid oxidation

Leads to diversion of ethanol from the major metabolic pathway Minor pathways (in the mitochondria, microsomes and Kuepfer cells) produce intermediates that more easily react with reactive oxygen Increased Alcohol Consumption Alcohol also increases inducible NO levels. NO with reactive oxygen produces toxic compounds in the liver. Greater burden than what Kuepfer cells are capable of maintaining, thus there is spill over of white cells and inflammatory cells into the parenchyma, causing further damage Mallory bodies, ballooning degeneration and necrosis

8 -20% of alcoholic liver disease progresses to cirrhosis Progression to Cirrhosis Risk Factors: ongoing alcohol use, daily vs binge drinking, smoking, obesity, female, superimposed liver disease (hepatitis B or C) Ongoing hepatic inflammation (marked by presence of inflammatory makers, especially neutrophils)

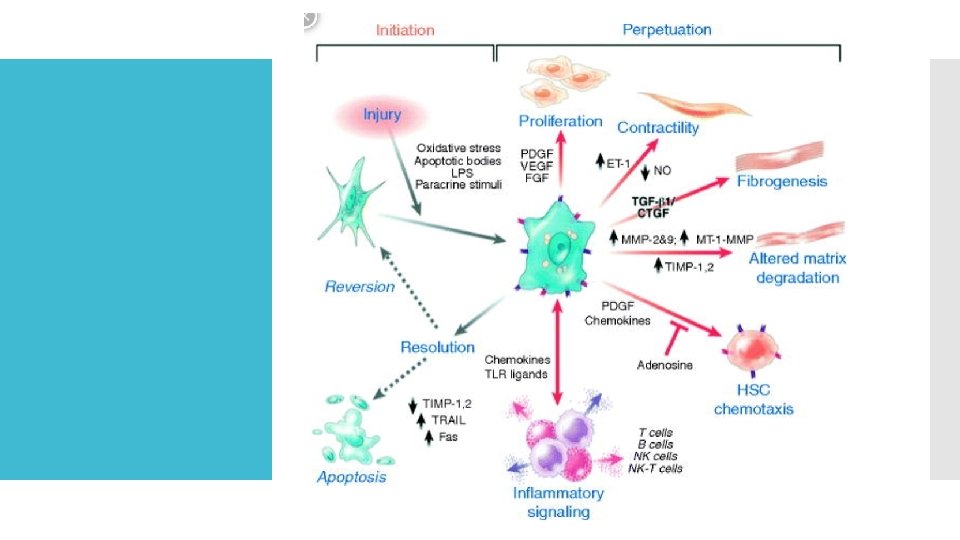
Scar tissue replacing normal parenchyma, which blocks portal flow of blood, increasing pressure and distorting normal function Damage and inflammation activates stellate cells to Secrete TGF-beta 1 Secrete TIMP 1 & 2 Produce Myofibroblasts Pathophysiolo gy of Cirrhosis

Complications of Cirrhosis

Albumin Decreased Protein Synthesis Ascites, edema Clotting Factors: 2, 7, 9, 10 Bleeding risk Increased INR Vitamin K will not work in a diseased liver Treat with FFP

Decreased ability to process toxins Ammonia accumulation Hepatic Encephalopathy Symptoms: confused, altered metnal status, asterixes, hyperreflexia Treatments: lactulose, rifaxinin, zinc, low protein diet Often precipitated by alkalosis, hypokalemia 9 diuretics), dsedative drugs, GI bleed, infection and hypovolemia

Symptoms: gynecomastia, palmar erythema, spider angiomata, testicular atrophy Estrogen Metabolism

Jaundice

Hepatorenal Syndrome Progressive renal failure secondary to hypoperfusion from vasoconstriction of renal vessels Symptoms: azotemia, oliguria, hyponatremia, low urine sodium (<10) Liver transplant is only treatment

Portal Hypertension Ascites Hemorrhoids Splenomegaly Varices

Ascites

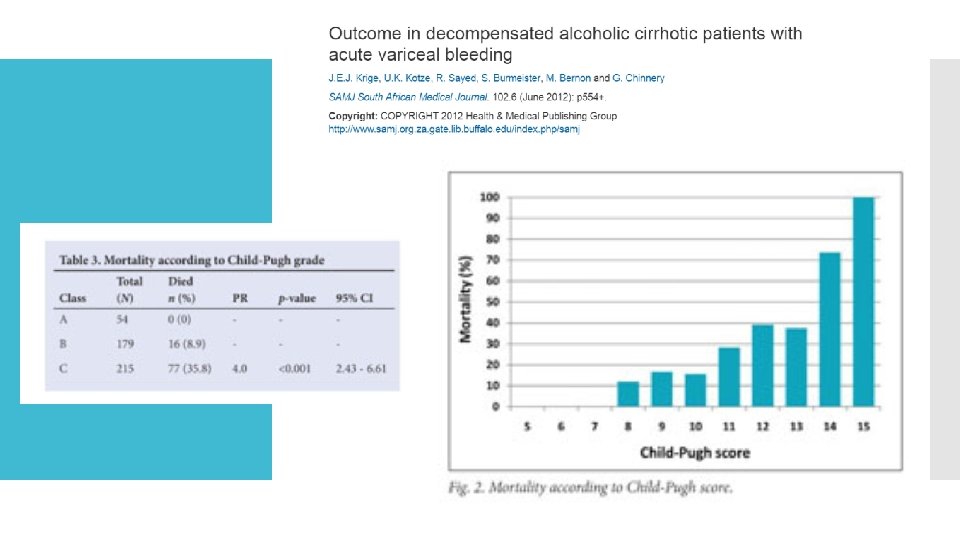
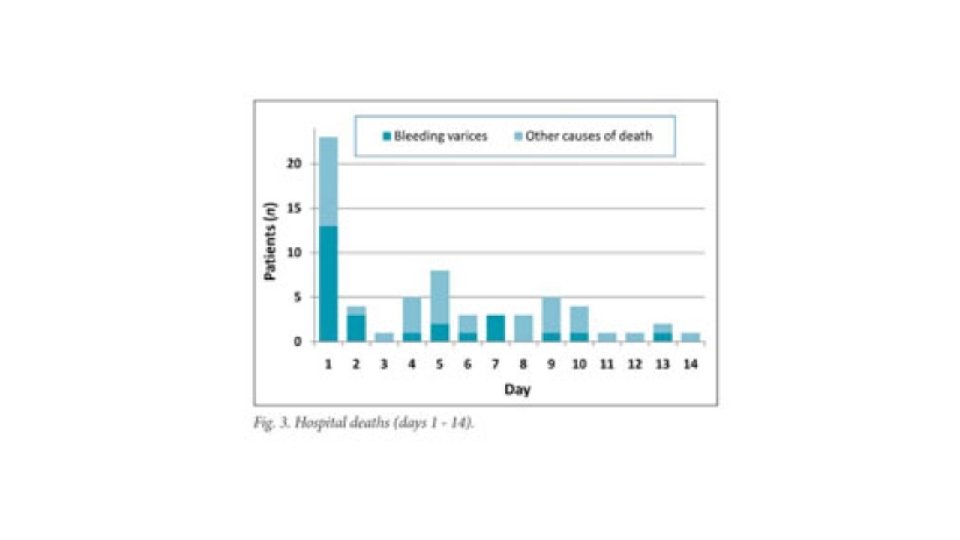
All patients with cirrhosis should be screened for varices 90% are esophageal, 10% gastric Treatment of asymptomatic varices: nonselective beta blocker (propranolol, nadolol) Variceal hemorrhage associated with high mortality rate Varices
 Octreotide Treatment of Acute Variceal Bleed Ligation/banding Sclerotherapy Long")
Fluids and antibiotics (ceftriaxone) Octreotide Treatment of Acute Variceal Bleed Ligation/banding Sclerotherapy Long term use of beta blockers Rebleeding Esophageal Balloon Tamponade Repeat Sclerotherapy TIPS

MELD Score

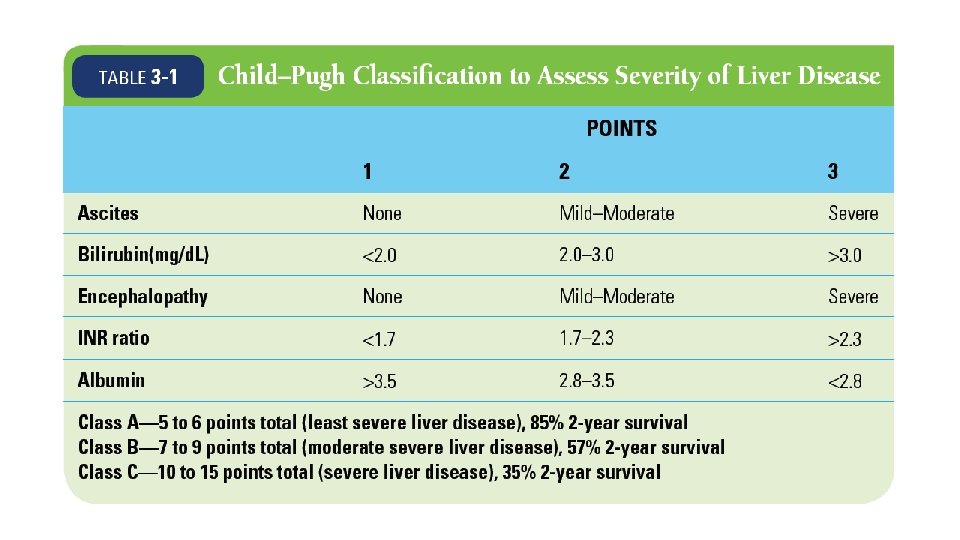
CHILDS-PUGH
- Slides: 35