MOOD DISORDERS YARD DO DR N BERFU AKBA

MOOD DISORDERS YARD. DOÇ. DR. N. BERFU AKBAŞ YEDİTEPE ÜNİVERSİTESİ PSİKİYATRİ AD
 %10 -25 women, %5 -12 men")
1 -DEPRESSIVE DISORDERS -MAJOR DEPRESSIVE DISORDER( MDD ) %10 -25 women, %5 -12 men - Persistant depressive disorder 2 - BIPOLAR DISORDERS
,")
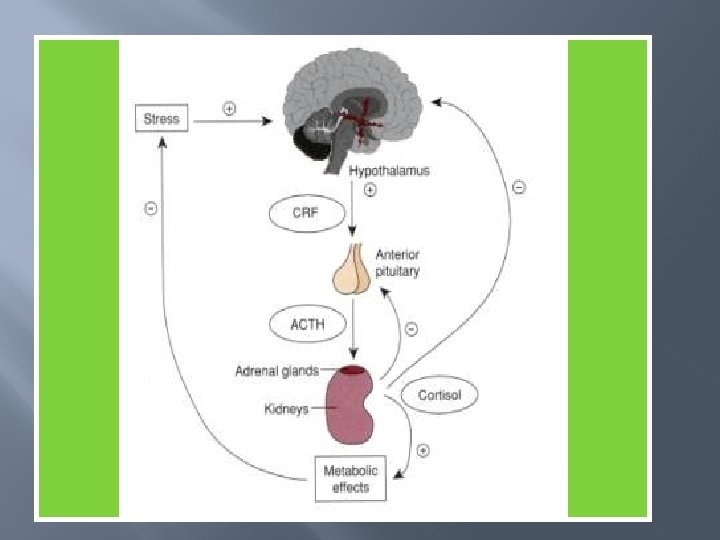
Neurobiological approaches to aetiology Monoamine hypothesis: Serotonin, noradrenaline, dopamine, Aminoacid neurotransmitters Glutamate ( ), GABA( ) Endocrine abnormalities HPA axis

DSM 5 CRITERIA for DEPRESSION � � � � � For at least 2 weeks, at least 5 of the below symptoms should be present: Depressed mood* Decreased interest or pleasure in activities* Change in apetite Sleep changes Pscyhomotor agitation or retardation Fatigue or loss of energy Feelings of worthlessness or guilt Concentration difficulties Thoughts of death
 � Neuroendocrine Regulation Adrenal axis (")
ETIOLOGY Biogenic Amines ( norepinephrine, serotonin, dopamine ) � Neuroendocrine Regulation Adrenal axis ( cortisol hypersecretion) Thyroid axis ( hypotyroidism) Growth hormone ( sleep abnormalities) � Limbic system, basal ganglia and hypothalamus most affected � Genetic factors � Psychosocial factors ( stress, personality) �
")
SPECIFIERS DESCRIBING MOST RECENT EPISODE � � � Psychotic features Melancholic features (endogeneous depression) Atypical features (overeating, oversleeping. . . ) Catotonic features ( immobility, negativism, mutism) Postpartum onset

� � DYSTHYMIA Depressed mood for at least 2 years + 2 of the following; Apetite changes, sleep changes, low energy, low self-esteem, poor concentration, feelings of hopelessness. “İll humored”, most cases early onset DOUBLE DEPRESSION: dysthymia + MDD
, clomipramine ( anafranil ), amitriptiline")
TREATMENT � � Pharmacotherapy: Tricyclic antidepressants: İmipramine ( tofranil), clomipramine ( anafranil ), amitriptiline ( laroxyl ), ( side effects: hypotension, arrithmias, seizures ) Serotonin reuptake inhibitors: Fluoxetine ( prozac), citalopram ( cipram), sertraline ( Lustral ), paroxetine ( paxil), essitalopram ( cipralex ) ( side effects: GI disturbance, bleeding? Bruxism? ) ECT

BIPOLAR DISORDERS BIPOLAR 1 DISORDER: � %0. 4 -1. 6, equal prevelance among sexes. � Onset is earlier than depression � 1 parent Bipolar: %25 risk in the sibling � Dx: At least 1 manic episode lasting for 1 week � Mania: at least 3 of following: -Grandiosity - psychomotor agitation -Decreased need for sleep - excessive activities -Talking -Flight of ideas -distractibility �

Manic Patients are: � � � Excited, talkative, sometimes amusing Cannot be interrupted while speaking, loud Delusions occur in %75 ( grandiose ) %75 assaultive or treatening Unreliable, lying

BIPOLAR II DISORDER � � � � � Presence of one or more depressive episodes Presence of at least one hypomanic episode Hypomania: at least 4 days 3 of the following; Grandiosity Decreased need for sleep Talkative Flight of ideas Distractibility Psychomotor agitation Excessive pleasurable activities

TREATMENT � � � Depressive attacks: antidepressants Manic attacks: mood stabilizers+ antipsychotics + benzodiazepines Mood Stabilizers: Lithium Antiepileptics These drugs are used chronically

CYCLOTHYMIC DISORDER -Episodes of hypomania and mild depression for 2 years. -%1 life time prevalance, 15 -25 years onset - F/M=3/2 - ınstability in relationships - Changes in mood are irregular, abrupt - Common substance use disorders - Tx: mood stabilizers - Antidepressants switch to mania
- Slides: 14