Molar Pregnancy GTD T ALLAMEH MD ASSOCIATED PROFESSOR


 Invasive mole Choriocarcinoma Placental site trophoblastic tumor Epithelioid trophoblastic tumor")










 Detected by pelvic sono")






 Beta adrenal blocking agent may be required before")



 Will fail to normalize and remain elevated at low")



 Partial mole (1 -5 %)")



- Slides: 37
Molar Pregnancy GTD T ALLAMEH MD ASSOCIATED PROFESSOR OF OB& GYN FELLOWSHIP OF GYNECOLOGY ONCOLOGY
GTD Complete hydatidiform mole Partial hydatidiform mole Benign & premalignant
Gestational Ttophoblastic neoplasia (GTN) Invasive mole Choriocarcinoma Placental site trophoblastic tumor Epithelioid trophoblastic tumor
Hydatidiform mole Originate in villous trophoblast Abnormal chorionic villi Trophoblastic hyperplasia Overexpression of paternal genes
Complete hydatidiform mole 80% homozygous 46 XX( duplication of single sperm following fertilization of an ovum in which the maternal chromosomes are lost) 20% 46 XX or 46 XY (dispermic fertilization ) Rarely biparental , autosomal recessive condition ( recurrent HMS, ovum donation )
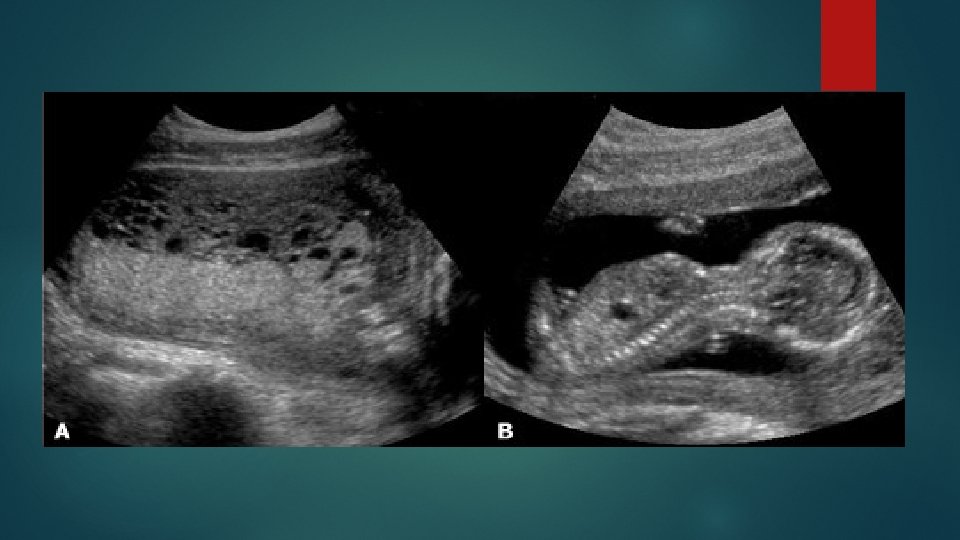
Partial hydatidiform mole Triploid (fertilization of an normal ovum by two sperm 69 XXX or 69 XXY or 69 XYY) Presence of a fetus Amniotic fluid is present Placenta in enlarged and cystic Increased transverse diameter of gestational sac Theca lutein cyst are usually absent h. CG levels of generally lower than complete mole
Epidemiology North American & European countries 66 -121/100, 000 pregnancy Latin American , Asian and Middle East 23 -1299/ 100, 000 pregnancy
Risk factors Maternal age < 15 and > 35 pr Prior molar pregnancy *After the first mole 1 to 1. 5% (10 to 15 times *After two mole 11 - 25% Decreasing levels of dietary carotene ↑ )
Clinical features High h. CG Vaginal bleeding Pelvic pressure or pain Uterine size greater than gestational age Hyperemesis gravidarum Hyperthyroidism Ovarian theca lutein cyst Preeclampsia <20 weeks Anemia Passage of hydropic vesicles
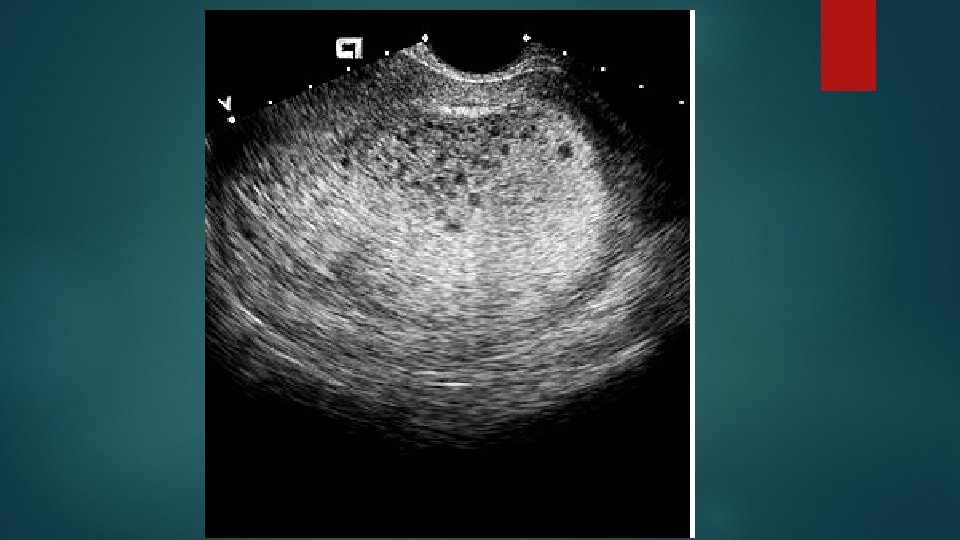
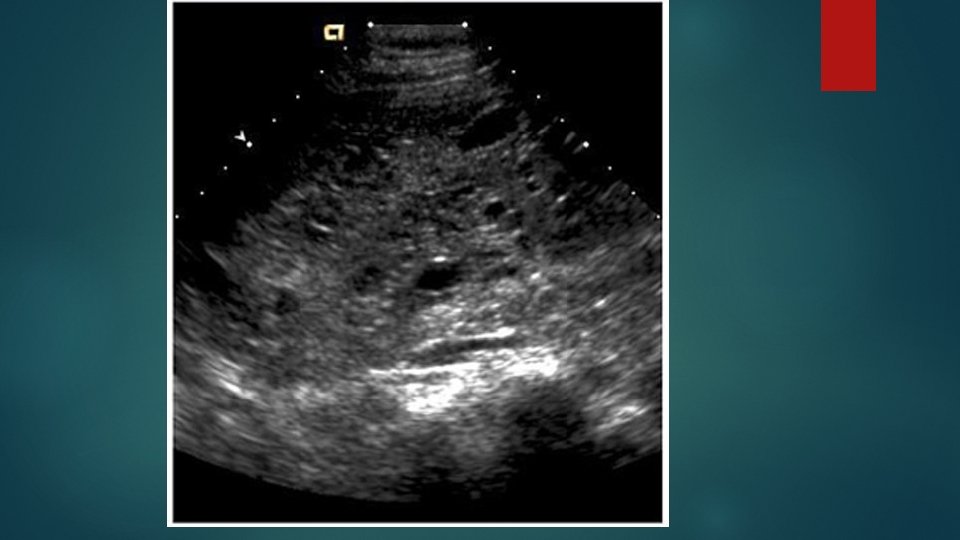
Diagnostic evaluation History Physical examination (vagina should be examined for metastases common sites of metastases include the vagina, lungs, liver, CNS) Pelvic ultrasound (snow storm or Swiss cheese pattern )
Theca lutein cysts
Laboratory evaluation h. CG if more than 100, 000 TVS should be performed – if apparently normal singleton gestation , sono and h. CG should be repeated in 1 week( normal fetus and co-existent molar pregnancy) Blood type and antibody screen Chest radiograph if the patient has pulmonary symptoms
Multiple gestation Normal co-twin with a mole(1/20000 to 1/100000 pregnancy) Detected by pelvic sono Preeclampsia , hemorrhage , thyrotoxicosis Preterm delivery , GTN - 57% delivered alive baby at 34 weeks - 26. 7% GTN developed These patients may continue the pregnancy under careful monitoring
Familiar recurrent molar pregnancy Biparental molar Typically familial Related genes are at choromosoms 19 q 13. 3 - 13. 4
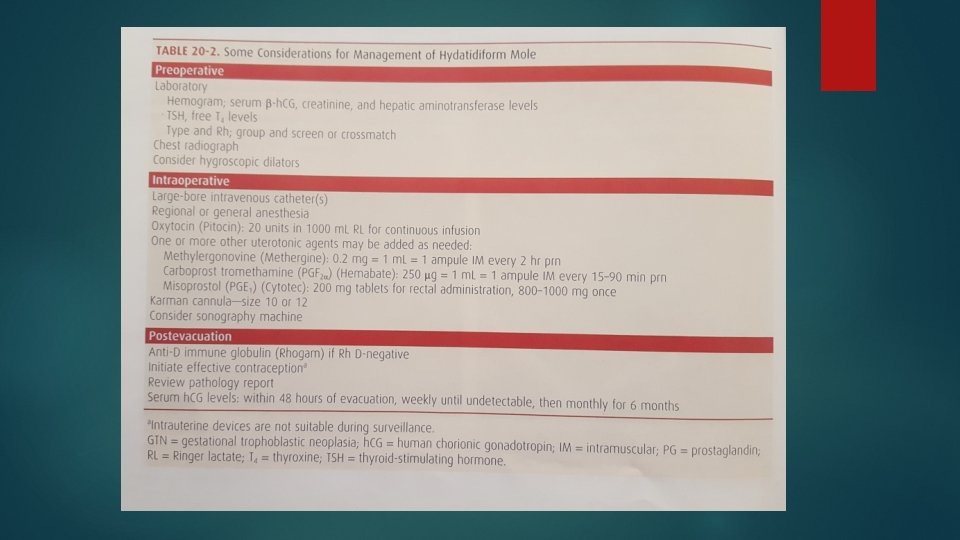
Management of hydatidiform mole Surgical uterine evacuation Medical uterine evacuation Hystrectomy
Surgical uterine evacuation * suction curettage * Laminaria * fundal massage if uterus is larger than 14 weeks * We do not use prostaglandins for cervical ripening * starting at the time of anesthesia induction , oxytocin infusion (10 units in 1 liter ringer lactate solution at 50 drops/min )
Medical uterine evacuation medication –only methods , misoprostol, mifepristone, oxytocin are controversial because of increase risk of trophoblastic embolization and obtaining a specimen for pathology 26% required uterine curettage 9% required chemotherapy ( 4 -6% after uterine curettage)
Hysterectomy For women with HM who are > 40 y and have completed child bearing. In one study GTN developed in 54% women treated with dilatation and evacuation and in non of the hysterectomy patients If h. CG levels > 175000 (ultra high risk ) Prophylactic chemo or TAH Eliminate local invasion and reduce GTN The ovaries may be preserved ( ovarian metastases are rare ) Large theca lutein cyst can be aspirated
Prophylactic chemotherapy High risk women Hormonal follow up unavailable or unreliable Do not impact future fertility Methotrexate or actinomyycin D 63% reduction in the risk of GTN ( delay in diagnosis of GTN ? )
Management of complication Hyperthyroidism (antithyroid ) Beta adrenal blocking agent may be required before the induction of anesthesia Ovarian theca lutein cyst ( regress over 2 -4 months, may need aspiration ) Preeclampsia (resolves promptly after molar evacuation ) Cardiopulmonary symptoms ( resolve within 72 h after evacuation)
Follow up Serial h. CG *Every week until non detectable for 3 weeks , then *Every month for 6 months *Trying to become pregnant
Shorter duration of monitoring Allow patients to become pregnant after achieving 3 consecutive weekly Followed by 3 consecutive monthly undetectable h. CG level
Diagnosis of GTN h. CG levels plateau ( remain within + percent of the previous result) Over a 3 weeks period( days 1, 7, 14 and 21) h. CG level increases > 10% over a 2 weeks duration(days 1, 7 and 14) Persistence of detectable h. CG for more than 6 months after molar evacuation
Persistent low h. CG(quiescent GTN) Will fail to normalize and remain elevated at low levels ( <200 at least 3 months) Absence of any clinical or radiological evidence of GTN May develop after partial mole , invasive mole or choricarcinoma Small focus of highly differentiated non invasive syncytiotrophoblast
Quiescent GTN Foci of disease are not readily identifiable clinically h. CG level is unresponsive to therapy The measurement of hyper glycosylated h. CG ( h. CG-H) has been proposed in patients with quiescent GTN. h. CG- H is produced by cytotrophoblast and is associated with trophoblast invasion growth of cytotrophoblast cells and promotion of placental implantation h. CG- H is a promoter of choriocarcinoma , tumorigenesis and is the main form of h. CG produced in active GTN
h. CG - H Low level indicate quiescent GTN Increasing levels indicate the development of active GTN that requires GTN Patients with quiescent GTN should be monitored with monthly h. CG and avoid pregnancy Active GTN should be diagnosed and treated If h. CG –H rises to greater than 20 % of total h. CG or if total h. CG has 2 doublings
Contraception Hormonal contraception Barrier methods IUD should not be used before the h. CG normalizes (uterine perforation )
Gestational trophoblastic neoplasia GTN Complete mole (15 -20 %) Partial mole (1 -5 %)
Risk factors for GTN Complete mole with signs of trophoblastic proliferation ( uterine size greater than gestational age , h. CG>100000 ) Ovarian theca lutein cysts > 6 cm Age >35 -40 y
Subsequent pregnancy Patients with MH can anticipate normal reproductive outcomes Repeat molar pregnancy * After 1 molar pregnancy 1 - 1. 9% * After 2 molar pregnancy 15 -17. 5 %
Obstetric management First trimester ultrasound to confirm normal pregnancy Measurement of h. CG at 6 weeks after the completion of pregnancy ( term or abortion) , to exclude choriocarcinoma Placenta should be examined and sent to pathology Product of conception from abortions should be examined pathologically