Module 3 Triage Unit Leader Triage Crews Porters




 Implements")














- Slides: 24
Module 3: Triage Unit Leader Triage Crews Porters and Morgue Manager
1 st Arriving Engine OIC EMS Branch Director (EMS BC or 3 rd arriving EMS Supervisor) Medical Group Supervisor (1 st arriving EMS Supervisor) Patient Transportation Group Supervisor (2 nd arriving EMS Supervisor) Medical Supply Coordinator (MCSU OIC) Triage Unit Leader (1 st arriving Engine OIC) Treatment Unit Leader (1 st arriving Medic OIC)
First arriving suppression unit after hazards are addressed
1 st arriving Engine Company must assign triage function to another arriving suppression company if they need to engage in suppression related duties and/or have to retain command
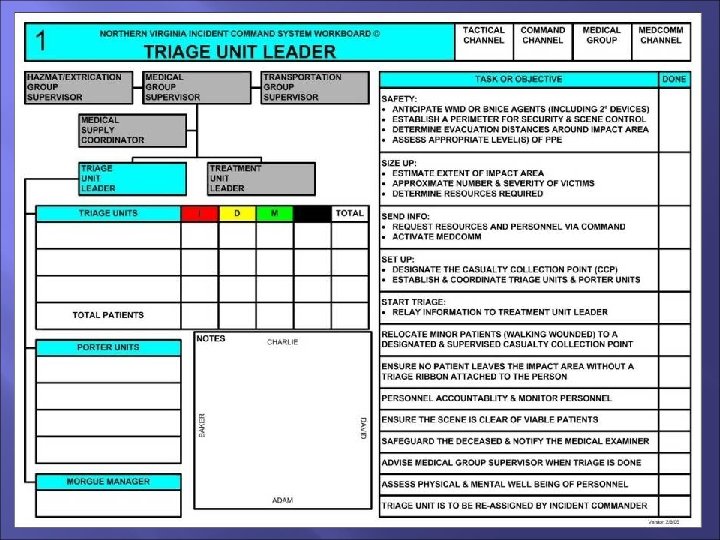
Identifies Staging Area, stages all units Identifies Casualty Collection Point (Treatment Area) Implements Triage Only essential life saving BLS interventions occur in triage area Care performed in treatment areas No EMS Transport Units to Impact Area Report to Casualty Collection Point (Treatment Area)
Generally is crew from 1 st arriving engine company Triages patients with triage ribbon Provides essential life-saving BLS treatment to patients prior to movement as incident conditions dictate
� Suppression Unit OIC �Bring Triage Board �Radio �Nextel �Traffic Vest �Clipboard �Pens �Markers
� Triage Crew �Wear Traffic Vest �Radio �Triage Ribbons �Extra Gloves �Hand Lights if needed
Tie appropriate ribbon around a wrist
� � If they can get up, are walking and talking they are initially Green If they lying on ground, crying, bleeding, rolling around and cannot get up they are Yellow If they are lying on ground, unconscious/semi-conscious, SOB, heavy bleeding, shock-like s/s they are RED No Pulse or Respirations they are Black (DOA)
� If they are Minor � Assign FRD member to them and remove from impact area � Consider moving them out of view of Yellow/Red Treatment areas � Place green ribbon on their wrist � Communicate to Triage Unit Leader number of green tags � Consider transport by bus to various hospitals Coordinate with RHCC � Re-triage once you have gained control over group Re-Triage every 15 minutes
� Move them from Impact Area to Treatment Areas � � � Immediate-First Delayed-Second Delayed Limited Patient Care � � Airway Positioning Bleeding Control � Do not waste time splinting extremity fractures � Use Engine, Truck and Rescue Personnel � Use whatever you can to move patients
C-Spine Immobilization is nice but goal is to quickly remove viable injured out of Impact Area (Bombing Event, Active Shooter)
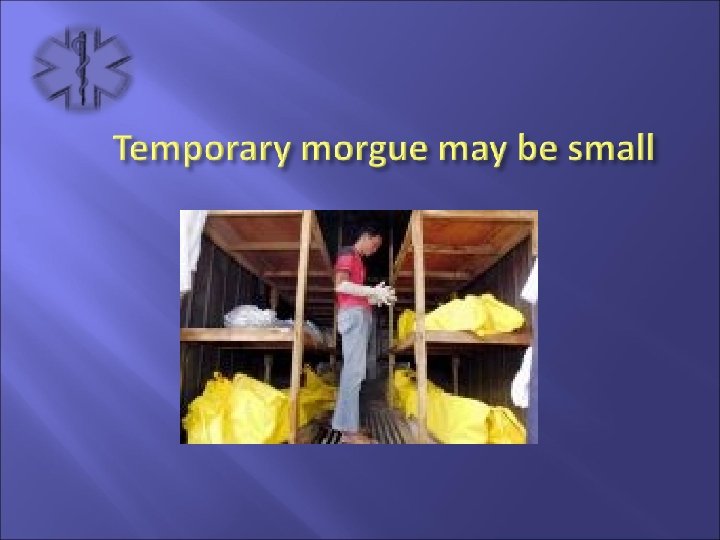
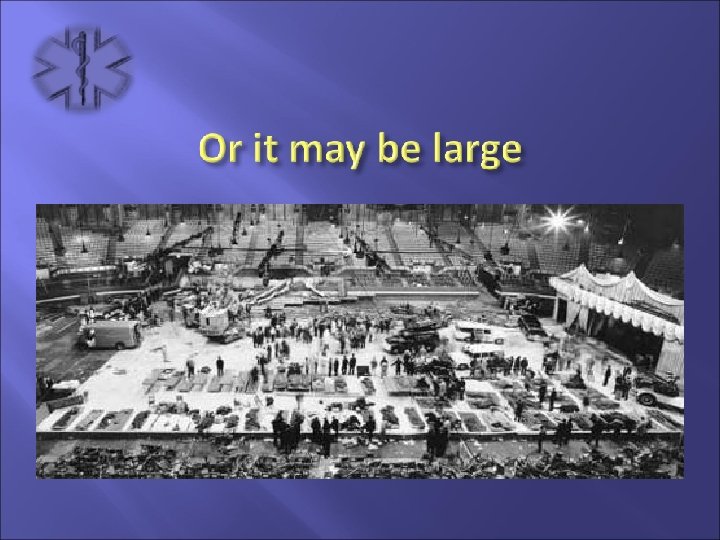
Establish temporary morgue away from viable patients
� � � Ensure identity of deceased persons is kept confidential Be ready to accept deceased patients from treatment area Once police department arrives on scene, turn temporary morgue over
� Either way - should be established in secluded area � Keep area off limits to all but authorized personnel � Use place that can be easily secured to limit access
So be respectful of the dead